Introduction
The major purpose of root canal therapy is to reduce
the intracanal microorganisms. Chemo-mechanical preparation is an
essential and indispensable step in disinfecting the root canal
system (1). During endodontic
treatment, the roots are susceptible to dentinal damage. Various
factors, including the physical properties of the teeth, the
endodontic instruments and the preparation technique used,
contribute to this damage (2).
In addition to stainless steel hand files, several
rotary nickel-titanium (Ni-Ti) file systems have been introduced
for the preparation of root canals (3). Ni-Ti instruments have numerous
advantages over conventional files, including increased flexibility
and a shorter working time (3).
However, these systems have different tip designs, tapers and
cutting blade configurations that place stress on the root canal
walls and may lead to microcracks or craze lines, which may develop
into fractures due to repeated stress from occlusal forces
(4) and may then lead to tooth loss.
Three recently introduced single-file Ni-Ti systems, including
WaveOne (WO), OneShape (OS) and Reciproc (RE), enable canal
preparation using only one instrument and require less time in
comparison with full-sequence rotary instrument systems. However,
Kishen (5) reported that cracks may
also form in untreated teeth due to the patient age (6), gender, masticatory function or occlusal
trauma. Certain studies have indicated that root fracture is
connected with dentinal removal (3,7,8), whereas other researchers have not
supported this theory (9,10). The movement caused by the preparation
method, the design and taper of the file, and the preparation time
lead to different degrees of microcracks (9,11–13).
The primary techniques currently used to observe
dentinal microcracks are stereoscopic microscopy (14), scanning electron microscopy (SEM),
staining, infrared imaging and micro-computed tomography
(micro-CT). SEM is typically used to observe the slice of a root
(11,15,16);
however, cracks may be formed at the root during both sample
preparation and the period of observation. Since microcracks can
extend through every slice or remain on the surface, SEM may miss
microcracks in the slices, which limits its use in dentinal
microcrack observation. Furthermore, stereoscopic microscopy,
staining and infrared imaging do not reveal cracks with a
micro-scale resolution (17,18).
Micro-CT is a multi-functional three-dimensional
scanning method that offers high resolution; thus, the use of
micro-CT in dental analyses is increasing. In recent years,
micro-CT has enabled novel possibilities for endodontic research by
allowing nondestructive volumetric quantitative and qualitative
assessments prior to and following different endodontic procedures
(9,19).
The present study evaluated the alterations observed
in dentinal microcracks following root canal preparation with three
different single-file Ni-Ti file systems using micro-CT analysis. A
hand k-file system was used as a reference technique for
comparison.
Materials and methods
Selection of the specimens
A total of 100 human mandibular first molars with
completely separated roots, which were extracted for reasons
unrelated to the present study, were obtained from a pool of teeth
between April 2016 and June 2016 from a total of 92 patients at the
Guanghua School and Hospital of Stomatology (Guangzhou, China).
Teeth were stored in 0.9% normal saline at 5°C. All patients (aged
20–70 years old; 52 male:40 female) provided informed consents, and
the experiments were approved by the local ethics committee of
Guanghua School and Hospital of Stomatology, Sun Yat sen
University.
For the selection of samples, the roots were
initially inspected by stereomicroscopy under a magnification of
×12 to exclude teeth with pre-existing craze lines or cracks. A
digital radiography scan in a buccolingual direction was performed
to determine the curvature angle of the mesial root using an
open-source image analysis program (Fiji version 1.47n software;
Fiji, Madison, WI, USA). Only teeth with a moderate curvature of
the mesial root (ranging between 10° and 20°) were selected. Teeth
without patency for the canal length, as determined by a size 10
k-file (Dentsply Maillefer, Tulsa, OK, USA), were also discarded.
The coronal portions and distal roots of all teeth were removed
using a low-speed saw (IsoMet; Buehler, Lake Bluff, IL, USA) with
water cooling. Mesial roots of ~11±1 mm in length were left to
prevent the introduction of confounding variables. As a result, 100
specimens were selected and stored in 0.9% normal saline at
5°C.
Micro-CT scanning
In order to obtain an overall outline of the
anatomic configuration of the mesial canals, specimens were
pre-scanned at a relatively low isotropic resolution (70 mm) using
a micro-CT scanner (µCT 50; Scanco Medical, Brüttisellen,
Switzerland) at 70 kV and 114 mA. Based on this pre-scan set of
images, 80 specimens with type II Vertucci canal configurations
were selected. These specimens were scanned again at an isotropic
resolution of 7.4 mm. Flat-field correction was performed prior to
the scanning procedure in order to correct for variations in the
camera pixel sensitivity. Scanning was performed by 360° rotation
around the vertical axis with a rotation step of 0.5°. The X-ray
source was an air-cooled, sealed, microfocus X-ray tube with a
focal spot size of 5 µm. X-rays were filtered with a 0.5-mm
aluminum filter, and the X-ray tube was operated at 70 kV and 228
µA. The X-ray detector comprised a 2,048×2,048 pixel, 16-bit
charge-coupled device camera with fiber-optic coupling to an X-ray
scintillator. The system, which was controlled with a PC
workstation running the Microsoft Windows XP Professional operating
system (Microsoft Corp., Redmond, WA, USA), was used to acquire
1,300–1,600 transverse cross-sections per tooth in a bitmap
format.
Root canal preparation
A thin film of polyether impression material was
used to coat the cement surface of the roots to simulate the
periodontal ligament. Each specimen was placed coronal-apically
inside a custom-made epoxy resin holder (diameter, 18 mm) to
further streamline the co-registration processes. Apical patency
was determined by inserting a size 10 k-file (size 10, 0.02 taper)
(9,15) into the root canal until its tip was
visible at the apical foramen, then the length of the file was
measured from the apical foramen to the cross section, and the
working length (WL) was 0.5 mm shorter than the length of the file.
Subsequent to establishing glidepaths with a length up to the WL
using a size 15 k-file (size 15, 0.02 taper) (Dentsply Maillefer),
the specimens were randomly assigned to three experimental groups
and a control group (n=20 per group) according to the system used
for root canal preparation. The groups were as follows: WO group,
in which the WO Ni-Ti reciprocating instrument (Dentsply Maillefer,
Tulsa, OK, USA) was used; OS group, in which the OS Ni-Ti rotary
instrument (Micro-Mega, Besançon, France) was used; RE group, in
which the Reciproc Ni-Ti reciprocating instrument (VDW GmbH,
Munich, Germany) was used; and the control group, in which a
stainless steel root canal file (Dentsply Maillefer) was used.
In all groups, irrigation was performed using 40 ml
(5.25%) sodium hypochlorite. Instruments were driven with the
X-Smart plus motor (Dentsply Maillefer) according to each
manufacturer's protocol, and a single experienced operator
performed all the preparations. The apical sizes and tapers of the
Ni-Ti preparation systems are shown in Table I.
 | Table I.Apical sizes and tapers of different
nickel-titanium preparation systems. |
Table I.
Apical sizes and tapers of different
nickel-titanium preparation systems.
| Preparation
system | Apical size (mm) | Taper (%) |
|---|
| WaveOne | 0.25 | 8 |
| OneShape | 0.25 | 6 |
| RE | 0.25 | 8 |
In the WO group, the WO instrument (size 25, 0.08
taper) was moved in the apical direction using a slow in- and -out
pecking motion of ~3 mm in amplitude with light apical pressure in
a reciprocating motion until the WL was reached. The instrument was
then removed from the canal and cleaned. The specimens in the OS
group were prepared with the OS instrument (size 25, 0.06 taper)
using rotary motion to reach 2/3 of the WL value, the WL-3 mm and
the WL. In the RE group, the Reciproc instrument (size 25, 0.08
taper) was moved as described for the WO group. The control group
was also prepared in a standard manner with a stainless steel root
canal file until the WL was reached. The following sequence was
used: A size 20 k-file (size 20, 0.02 taper) and a size 25 k-file
(size 25, 0.02 taper). Subsequent to four steady strokes, the
instrument was removed from the canal. Next, 17% EDTA was used to
wipe off the smear layer, and 0.9% normal saline was used to finish
the preparation. Micro-CT scans of all samples were then performed
using the aforementioned parameters.
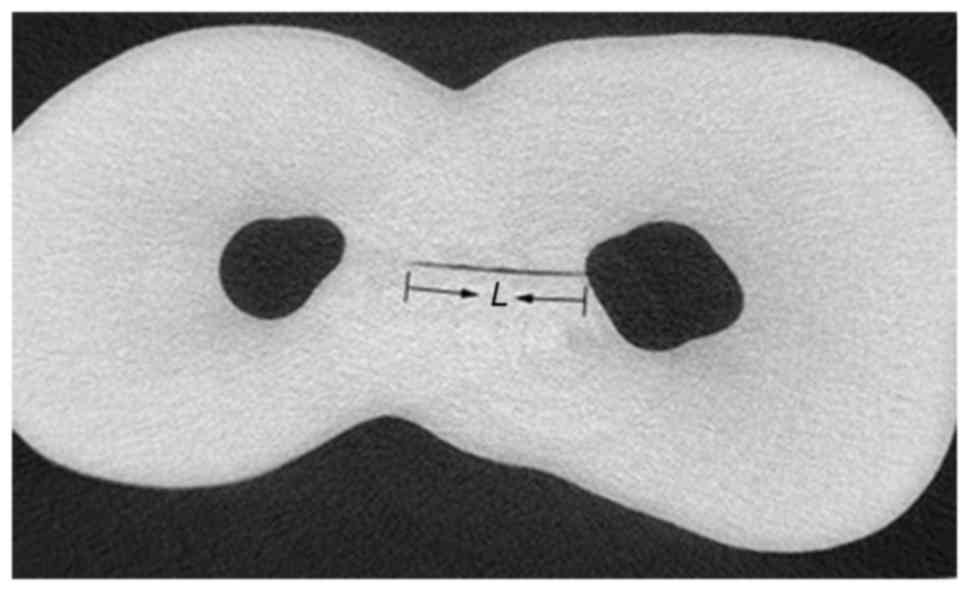
Dentinal microcrack measurement
The cross-section images of the mesial roots from
the furcation level to the apex (n=297,200) were observed with
ImageJ image processing software (National Institutes of Health,
Bethesda, MD, USA) in order to analyze the type and distribution of
microcracks. The images were screened by three ImageJ trained
examiners to measure the dentinal microcrack lengths according to
the length of the black line in the slice that was measured, as
demonstrated in Fig. 1. To validate
the screening process, image analyses were repeated twice at 2-week
intervals. In cases of disagreement among the examiners, the images
were re-examined until agreement was reached. The samples were
divided evenly into the coronal, medial and apical parts. The
percentage, which was determined by the microcrack length of one
part divided by the length of the entire sample, was quantified as
the distribution of microcracks.
Statistical analysis
The data were statistically analyzed using SPSS
software (version 19.0 for Windows; IBM Corp., Armonk, NY, USA).
All data were presented normal distribution and homogeneity of
variance. The lengths of preoperative dentinal microcracks were
analyzed using analysis of variance. Alterations in microcrack
lengths prior to and following preparation within the same group
were analyzed using a paired t-test. Differences in the dentin
microcrack lengths were assessed using a Student-Newman-Keuls (SNK)
test. P<0.05 indicated that the differences were statistically
significant.
Results
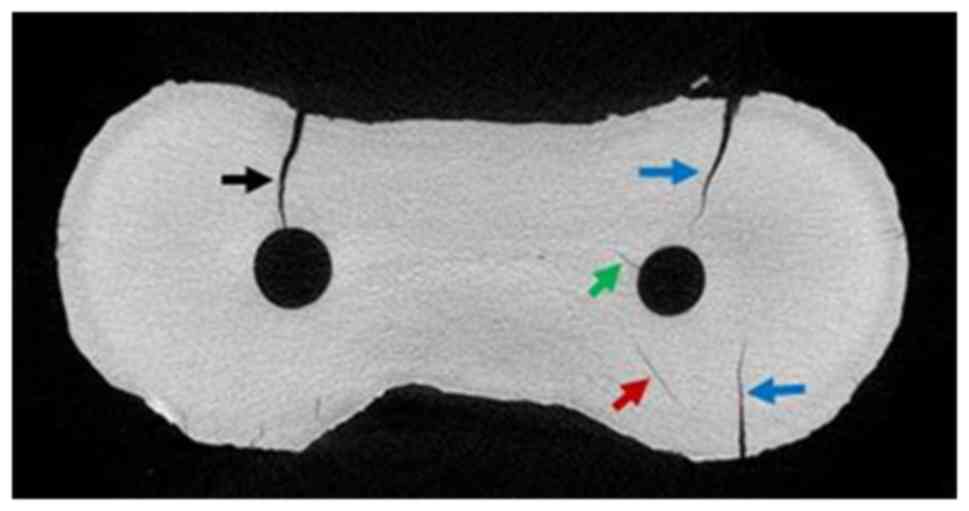
Microcrack classification
ImageJ processing software was used to observe the
morphology of each sample. As shown in Fig. 2, the microcracks were classified as
follows: Complete, originating from the root canal and extending to
the root wall (black arrow); incomplete, originating from the root
canal and not extending to the root wall (green arrow); or
in-dentine, indicating microcracks present only in the dentine or
originating from the root wall without reaching the root canal (red
and blue arrows, respectively) (20).
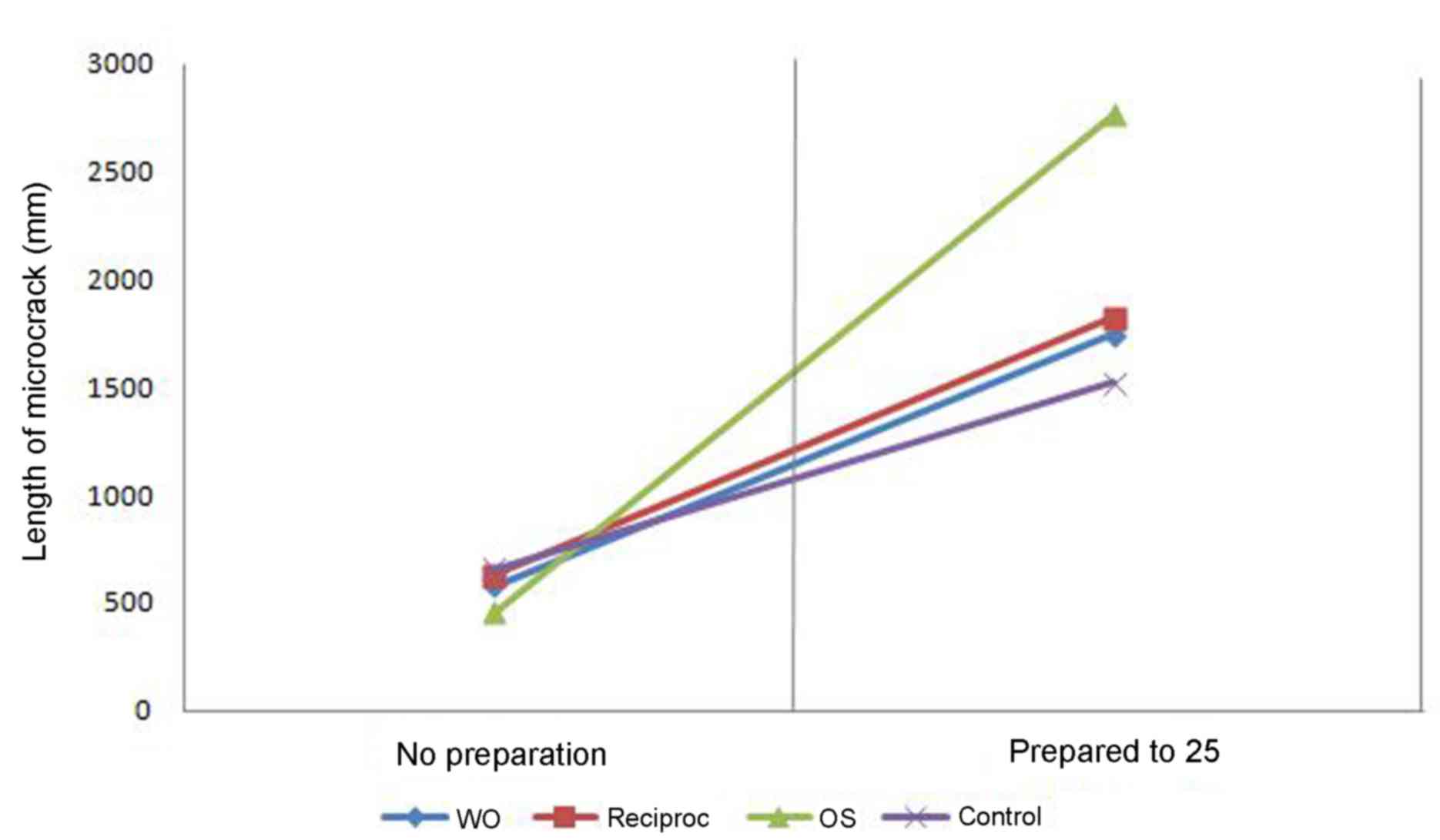
Microcrack length
The lengths of the dentin microcracks without
preparation were not statistically significant (P>0.05). A
paired t test was used to analyze changes in the microcrack length
prior to and following preparation. When compared with the length
prior to preparation, the OS group length was significantly
increased after preparation (P<0.05), whereas there were no
significant changes in the WO, RE and control groups (P>0.05;
Table II). Furthermore, as
determined by the SNK test, the differences in the dentin
microcrack lengths when prepared to size 25 between the three
groups (WO, RE and control) and the OS group were statistically
significant (P<0.05; Table II).
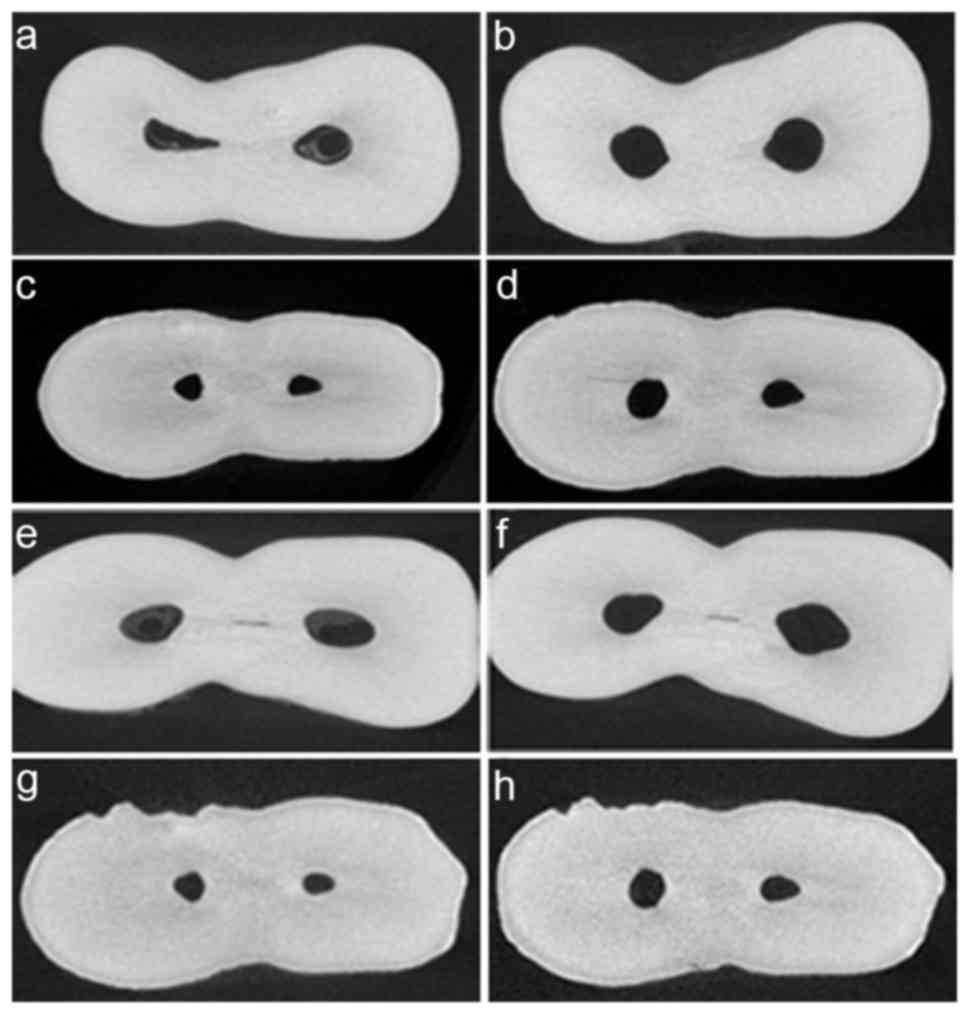
Similarly, Figs. 3 and 4 also indicated the lengths of microcracks
were markedly increased in the OS after preparation compared with
the other groups (Fig 3).
| Table II.Length of microcracks in all
groups. |
Table II.
Length of microcracks in all
groups.
|
| Microcrack
length |
|
|---|
|
|
|
|
|---|
| Group | No preparation,
µm | Prepared to size 25,
µm | P-value |
|---|
| WO |
576.097±233.310 |
1745.492±293.933 | 0.12 |
| OS |
456.928±200.030 |
2763.932±333.685a | 0.011 |
| RE |
626.044±259.122 |
1822.519±370.132 | 0.078 |
| Control |
657.710±202.638 |
1521.711±392.589 | 0.054 |
Distribution of microcracks
Samples were trisected, the length of each section
was collected and the distribution of microcracks as a percentage
of the total length was expressed. As illustrated in Table III, the distribution changes of
microcracks in the OS group was primarily observed in the apical
and coronal parts of the samples. Others groups exhibited no
distribution changes in the apical, coronal or medial parts.
| Table III.Distribution of microcracks prior to
and following preparation (%). |
Table III.
Distribution of microcracks prior to
and following preparation (%).
| Time point | WO | OS | RE | Control |
|---|
| Prior to
preparation |
|
|
|
|
| Coronal
part | 35 | 35 | 36 | 35 |
| Medial
part | 37 | 44 | 37 | 36 |
| Apical
part | 28 | 21 | 27 | 29 |
| Following
preparation |
|
|
|
|
| Coronal
part | 35 | 41 | 36 | 35 |
| Medial
part | 37 | 36 | 37 | 36 |
| Apical
part | 28 | 23 | 27 | 29 |
Discussion
A novel technique that uses reciprocating motion has
been previously proposed for root canal preparation (21). This approach relieves the stress on
the instrument through counterclockwise and clockwise movements
and, therefore, increases its resistance to cyclic fatigue compared
with the traditional continuous rotation motion (22,23). The
WO and RE instruments, which were designed by different
manufactures, are the main examples of commercially available
single-file reciprocating Ni-Ti systems for root canal preparation
that alternate between different values of counterclockwise and
clockwise rotation movements, which allows for 360° preparation
subsequent to a series of reciprocating movements (24,25). In
addition, the OS instrument was designed using a single file and a
rotary movement to complete preparation.
Previous studies have demonstrated a high rate of
dentinal defects caused by the mechanical preparation of root
canals (15,26). Bürklein et al (12) demonstrated that root canal
preparation with both rotary and reciprocating instruments resulted
in dentinal defects. In addition, at the apical level,
reciprocating files produced significantly more incomplete dentinal
cracks as compared with those produced by full-sequence rotary
systems. By contrast, Liu et al (13) used a similar methodology and observed
that the ProTaper multiple-file rotary system caused an increased
number of cracks on the apical root surface and in the canal wall
in comparison with single-file rotary or reciprocating systems.
Ashwinkumar et al (15) also
observed that canal preparation with ProTaper rotary files was
associated with significantly more microcracks compared with the WO
reciprocating system.
Studies correlating mechanical preparation and the
development of dentinal defects are based only on root-sectioning
methods and direct observation by optical microscopy (11,15,16).
These methods undoubtedly have significant limitations associated
with the destructive nature of the experiment, as reported in
previous studies (11–13,15,16). In
previous results in which unprepared teeth were used, their control
groups appeared to be validated as effective control groups;
however, as no dentinal defects were detected, this type of control
does not consider the potential damage produced by the interplay
among the four sources of stress on the root dentin, including
mechanical preparation, a chemical attack with sodium
hypochlorite-based irrigation, sectioning procedures and
dehydrogenation drying procedures (27).
In the present study, micro-CT imaging technology
was used to evaluate the length of dentinal defects at the baseline
and to compare the thickness of the dentine. This highly accurate
and non-destructive method enables the assessment of specimens
prior to preparation. Therefore, pre-existing cracks can be
detected, and it is possible to determine the precise region in
which they were created and/or propagated. However, it may be
argued that any dentin damage occurring between pre- and
post-preparation conditions would be below the spatial resolution
threshold of the micro-CT system, and thus may be overlooked. The
full extension of dentinal microcracks visualized under
conventional stereomicroscopy may also be observed in micro-CT
cross-sectional images, which confirms the reliability of this
novel technology for detecting dentin defects. Notably, while
conventional sectioning techniques allow the evaluation of only a
few slices per tooth with the possibility of missing several
defects along the root, hundreds of slices of each tooth can be
analyzed with micro-CT imaging (9,28).
Another methodologic dissimilarity between the technique used in
the present study and those of previous studies is associated with
sample selection. Although the majority of previous studies used
single-rooted teeth, the present study used mesial canals of
mandibular molars (3,12,13,26,29).
These canals have a constricted anatomic configuration that may
result in increased stress on the dentinal surface during
mechanical preparation and, consequently, increase the potential
for cracks. Therefore, the current results demonstrated a marked
contrast with the findings of previous studies. Comparing dentinal
microcracks only subsequent to preparation demonstrated that the
length increased significantly. This reflected the results
identified in previous studies that did not conduct pre-preparation
comparisons.
Therefore, in the present study, it is hypothesized
that the influence of the prepreparation dentinal microcracks on
microcrack development is significant. The condition of the
prepreparation microcracks is associated with the patient's age,
gender, occlusion habits and occlusion force. However, the data
regarding the length of microcracks prior to and following
preparation exhibited normal distribution and homogeneity of
variance. Therefore, a paired t-test was used to analyze the
increase in the length within the same sample and the SNK test was
conducted to compare the differences between the experimental and
control groups (pre- and post-preparation), respectively.
The paired t-test performed in the current system
indicated that the OS system resulted in the formation of evident
microcracks. By contrast, the WO system, the RE system and the hand
files may not form marked microcracks. It has been reported that
the potential to promote dentinal defects may be associated with
the design of the instrument used (11). According to Bier et al
(3), an increased file taper of
rotary instruments contributed to the formation of dentinal defects
due to the increased stress on the canal walls. However, the
reciprocating instruments, WO and RE systems, had larger tapers in
comparison with the rotary instrument, OS system. According to a
recent study, reciprocating instruments would be more likely to
promote the development or propagation of dentin microcracks and
dentinal damage compared with rotary movement using SEM (12). This supports the argument that root
canal preparation using only a single, large-tapered reciprocating
instrument, which cuts substantial amounts of dentin in a short
time, tends to create or aggravate the dentinal defects when
compared with the conventional preparation that allows for a more
progressive and slower mechanical enlargement. In the present
study, it is speculated that the number of the files, the taper and
the speed and torque had no effect on the formation of microcracks,
whereas the preparation movement may affect the development of
dentinal microcracks.
The different morphologies of dentinal microcracks,
including complete and incomplete microcracks, as well as
microcracks confined in the dentine (Fig. 2), are associated with the stress
intensity, concentration zone and root canal wall thickness. The OS
system generated microcracks in the apical and coronal parts of the
root, and the most common morphology was microcracks confined in
the dentine. The thread design in the medial part of the OS system
is a transition region that changes from three blades to two
(24,30). This design may explain why no
microcracks formed in the medial part. Furthermore, the apical part
rapidly expands from size 10 to size 25 using a single file, which
may have caused an increase in microcracks in this part.
In conclusion, the formation and development of
dentinal microcracks may be associated with the movement caused by
preparation, as opposed to the taper of the files. Among
single-file Ni-Ti systems, WO and RE were not observed to cause
evident microcracks, whereas the OS system resulted in increased
microcracks.
References
|
1
|
Arslan H, Barutcigil C, Karatas E,
Topcuoglu HS, Yeter KY, Ersoy I and Ayrancı LB: Effect of citric
acid irrigation on the fracture resistance of endodontically
treated roots. Eur J Dent. 8:74–78. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ertas H, Sagsen B, Arslan H, Er O and
Ertas ET: Effects of physical and morphological properties of roots
on fracture resistance. Eur J Dent. 8:261–264. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bier CA, Shemesh H, Tanomaru-Filho M,
Wesselink PR and Wu M: The ability of different nickel-titanium
rotary instruments to induce dentinal damage during canal
preparation. J Endod. 35:236–238. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Shemesh H, van Soest G, Wu M and Wesselink
PR: Diagnosis of vertical root fractures with optical coherence
tomography. J Endod. 34:739–742. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kishen A: Mechanisms and risk factors for
fracture predilection in endodontically treated teeth. Endodont
Top. 13:57–83. 2006. View Article : Google Scholar
|
|
6
|
Kubo M, Miura J, Sakata T, Nishi R and
Takeshige F: Structural modifications of dentinal microcracks with
human aging. Microscopy (Oxf). 62:555–561. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Er K, Tasdemir T, Siso SH, Celik D and
Cora S: Fracture resistance of retreated roots using different
retreatment systems. Eur J Dent. 5:387–392. 2011.PubMed/NCBI
|
|
8
|
Saber SE, Nagy MM and Schäfer E:
Comparative evaluation of the shaping ability of ProTaper Next,
iRaCe and Hyflex CM rotary NiTi files in severely curved root
canals. Int Endod J. 48:131–136. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pop I, Manoharan A, Zanini F, Tromba G,
Patel S and Foschi F: Synchrotron light-based µCT to analyse the
presence of dentinal microcracks post-rotary and reciprocating NiTi
instrumentation. Clin Oral Investig. 19:11–16. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sathorn C, Palamara JE and Messer HH: A
comparison of the effects of two canal preparation techniques on
root fracture susceptibility and fracture pattern. J Endod.
31:283–287. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yoldas O, Yilmaz S, Atakan G, Kuden C and
Kasan Z: Dentinal microcrack formation during root canal
preparations by different NiTi rotary instruments and the
self-adjusting file. J Endod. 38:232–235. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bürklein S, Tsotsis P and Schäfer E:
Incidence of dentinal defects after root canal preparation:
Reciprocating versus rotary instrumentation. J Endod. 39:501–504.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Liu R, Hou BX, Wesselink PR, Wu MK and
Shemesh H: The incidence of root microcracks caused by 3 different
single-file systems versus the ProTaper system. J Endod.
39:1054–1056. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Topçuoğlu HS, Düzgün S, Kesim B and Tuncay
O: Incidence of apical crack initiation and propagation during the
removal of root canal filling material with ProTaper and Mtwo
rotary nickel-titanium retreatment instruments and hand files. J
Endod. 40:1009–1012. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ashwinkumar V, Krithikadatta J, Surendran
S and Velmurugan N: Effect of reciprocating file motion on
microcrack formation in root canals: An SEM study. Int Endod J.
47:622–627. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Arias A, Lee YH, Peters CI, Gluskin AH and
Peters OA: Comparison of 2 canal preparation techniques in the
induction of microcracks: A pilot study with cadaver mandibles. J
Endod. 40:982–985. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wright HM Jr, Loushine RJ, Weller RN,
Kimbrough WF, Waller J and Pashley DH: Identification of resected
root-end dentinal cracks: A comparative study of transillumination
and dyes. J Endod. 30:712–715. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Matsushita-Tokugawa M, Miura J, Iwami Y,
Sakagami T, Izumi Y, Mori N, Hayashi M, Imazato S, Takeshige F and
Ebisu S: Detection of dentinal microcracks using infrared
thermography. J Endod. 39:88–91. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
De-Deus G, Silva EJ, Marins J, Souza E,
Ade A Neves, Gonçalves Belladonna F, Alves H, Lopes RT and Versiani
MA: Lack of causal relationship between dentinal microcracks and
root canal preparation with reciprocation systems. J Endod.
40:1447–1450. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Beling KL, Marshall JG, Morgan LA and
Baumgartner JC: Evaluation of cracks associated with ultrasonic
root-end preparation of gutta-percha filled canals. J Endod.
23:323–326. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yared G: Canal preparation using only one
Ni-Ti rotary instrument: Preliminary observations. Int Endod J.
41:339–344. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Pérez-Higueras JJ, Arias A and de la
Macorra JC: Cyclic fatigue resistance of K3, K3XF, and twisted file
nickel-titanium files under continuous rotation or reciprocating
motion. J Endod. 39:1585–1588. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kiefner P, Ban M and De-Deus G: Is the
reciprocating movement per se able to improve the cyclic fatigue
resistance of instruments? Int Endod J. 47:430–436. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Nabeshima CK, Caballero-Flores H, Cai S,
Aranguren J, Britto ML Borges and Machado ME: Bacterial removal
promoted by 2 single-file systems: Wave one and one shape. J Endod.
40:1995–1998. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bürklein S, Hinschitza K, Dammaschke T and
Schäfer E: Shaping ability and cleaning effectiveness of two
single-file systems in severely curved root canals of extracted
teeth: Reciproc and WaveOne versus Mtwo and ProTaper. Int Endod J.
45:449–461. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Shemesh H, Bier C, Wu M, Tanomaru-Filho M
and Wesselink PR: The effects of canal preparation and filling on
the incidence of dentinal defects. 42:1–213. 2009.
|
|
27
|
Shemesh H, Roeleveld AC, Wesselink PR and
Wu MK: Damage to root dentin during retreatment procedures. J
Endod. 37:63–66. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Moeller L, Wenzel A, Wegge-Larsen AM, Ding
M and Kirkevang LL: Quality of root fillings performed with two
root filling techniques. An in vitro study using micro-CT. Acta
Odontol Scand. 71:689–696. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Liu R, Kaiwar A, Shemesh H, Wesselink PR,
Hou B and Wu M: Incidence of apical root cracks and apical dentinal
detachments after canal preparation with hand and rotary files at
different instrumentation lengths. J Endod. 39:129–132. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kim HC, Lee MH, Yum J, Versluis A, Lee CJ
and Kim BM: Potential relationship between design of
nickel-titanium rotary instruments and vertical root fracture. J
Endod. 36:1195–1199. 2010. View Article : Google Scholar : PubMed/NCBI
|