Introduction
Tumor development depends on numerous reciprocal
interactions between the tumor environment and tumor cells. Tumor
immune cells are among the major components of the tumor
microenvironment (1,2). The antitumor immune response consists
of a series of stepwise events that are regulated by stimulatory
and inhibitory factors (3). Previous
evidence has suggested that the immune response to tumors typically
does not function correctly, which results in tumor cells escaping
from the surveillance of the immune system (3). Immune checkpoint proteins, which
include inhibitory receptors and ligands such as programmed cell
death (PD) 1/PD-ligand 1 (L1) and cytotoxic T-lymphocyte-associated
protein 4 (CTLA4)/B7, are key inhibitors in suppressing the
initiation and function of tumor immunity. Immune checkpoint
blockade therapy (ICBT) uses drugs that can interrupt the
inhibitory checkpoints to enhance tumor immunity and induce cancer
regression. ICBT has increased the five-year survival rate by 15%
from 30% in certain cancer patients, including patients with
melanoma (4,5). However, certain patients with renal
cancer do not respond to ICBT (5,6),
indicating the urgency to decrease intrinsic tumor resistance to
therapeutic agents.
Cluster of differentiation (CD) 103 (αE integrin) is
a subunit of the heterodimeric integrin molecule αEβ7. CD103 is
widely expressed in intraepithelial lymphocytes, tumor infiltrating
lymphocytes and certain dendritic cells (7–9).
Previous studies have demonstrated that CD103 serves an important
role in the cell lysis caused by tumor-specific infiltrating
lymphocytes via interacting with its ligand, E-cadherin, on the
tumor cells, triggering lytic granule polarization and exocytosis
(10,11). Furthermore, the ligation of CD103 and
E-cadherin promotes the adhesion of T cells to tumor cells and
induces co-stimulation in activated cytotoxic T cells (12). These findings suggest that CD103 may
be a target for enhancing tumor immunity.
Renal cell carcinoma (RCC) is ranked as the seventh
most common cancer type in males and the ninth most common cancer
type in females worldwide, accounting for 2–3% of all adult
malignancies (13). The primary
treatments for RCC remain surgery-oriented and these strategies are
not optimal for patients with advanced RCC. To date, no adjuvant
therapies have been identified to be of a significant benefit to
patients with RCC (14). Previously,
ICBT drugs have been tested in clinical trials; however, <30% of
patients with RCC responded to these treatments (15). Thus, there is a requirement to
enhance the sensitivity of RCC to ICBT. In the current study, the
prognostic value of CD103 in patients with RCC was examined, and
the potential therapeutic value of combining CD103 with ICBT was
evaluated in a RCC mouse model.
Materials and methods
Patient samples
A total of 200 RCC tumor samples were obtained from
the archive of Tianjin Nankai Hospital (Tianjin, China). Samples
collected between August 2015 and January 2016 were formalin-fixed
and paraffin-embedded (FFPE). The patients were diagnosed between
April 2004 and April 2010. Informed consent was provided by all
patients or their legal representatives. None of the patients
received chemotherapy or radiotherapy prior to the collection of
tissue samples by laparoscopic radical nephrectomy. In the present
study, all patients were randomly assigned to a training group
(n=100) or testing group (n=100) to increase the accuracy of the
results. The training group underwent relaxation training,
including mindfulness and music relaxation for 1 h per day. For
many cancer patients, physical symptoms, including sleep
difficulties or level of fatigue are severely affected by surgery
and chemotherapy, which may be influenced by the immune system
(16). Patients were divided into
two groups and only patients aged between 30–75 with no signs of
diseases of the immune system were included. The
clinicopathological features of the patients included in the
present study are summarized in Table
I. The tumor-node-metastasis (TNM) system of the American Joint
Committee on Cancer and the histological grading criteria of the
World Health Organization were used to evaluate the tumors
(16).
 | Table I.Clinicopathological features and
CD103+ cell count of the patients with renal cell
carcinoma included in the present study. |
Table I.
Clinicopathological features and
CD103+ cell count of the patients with renal cell
carcinoma included in the present study.
| A, Training group
(n=100) |
|---|
|
|
| CD103+
cell count |
|
|---|
|
|
|
|
|---|
| Parameter | Low, n (%) | High, n (%) | P-value |
|---|
| Age, years |
|
|
|
|
<61 | 26 (38.2) | 42 (61.8) | 0.161 |
|
≥61 | 17 (53.1) | 15 (46.9) |
|
| Gender |
|
|
|
|
Male | 14 (36.8) | 24 (63.2) | 0.330 |
|
Female | 29 (46.8) | 33 (53.2) |
|
| Grade |
|
|
|
|
I+II | 17 (41.5) | 24 (58.5) | 0.796 |
|
III+IV | 26 (44.1) | 33 (55.9) |
|
| T stage |
|
|
|
|
T1+T2 | 16 (50.0) | 16 (50.0) | 0.332 |
|
T3+T4 | 27 (39.7) | 41 (60.3) |
|
| Lymph node |
|
|
|
|
N0-N2 | 17 (37.0) | 29 (63.0) | 0.260 |
|
N3-N4 | 26 (48.1) | 28 (51.9) |
|
| Metastasis |
|
|
|
|
Negative | 36 (41.9) | 50 (58.1) | 0.568 |
|
Positive | 7 (50.0) | 7 (50.0) |
|
| TNM stage |
|
|
|
|
I+II | 13 (28.9) | 32 (71.1) | 0.010 |
|
III+IV | 30 (54.5) | 25 (45.5) |
|
| Patient status |
|
|
|
|
Alive | 5 (13.5) | 32 (86.5) | P<0.001 |
|
Succumbed | 38 (60.3) | 25 (39.7) |
|
|
| B, Testing group
(n=100) |
|
|
|
CD103+ cell count |
|
|
|
|
Parameter | Low, n
(%) | High, n
(%) | P-value |
| Age, years |
|
|
|
|
<62 | 28 (43.7) | 36 (56.3) | 0.148 |
|
≥62 | 12 (33.3) | 24 (66.7) |
|
| Sex |
|
|
|
|
Male | 19 (41.3) | 27 (58.7) | 0.307 |
|
Female | 21 (39.6) | 32 (60.4) |
|
| Grade |
|
|
|
|
I+II | 15 (33.3) | 30 (66.7) | 0.218 |
|
III+IV | 25 (45.5) | 30 (54.5) |
|
| T stage |
|
|
|
|
T1+T2 | 22 (47.8) | 24 (52.2) | 0.140 |
|
T3+T4 | 18 (33.3) | 36 (66.7) |
|
| Lymph node |
|
|
|
|
N0-N2 | 20 (37.7) | 33 (62.3) | 0.624 |
|
N3-N4 | 20 (42.6) | 27 (57.4) |
|
| Metastasis |
|
|
|
|
Negative | 32 (38.6) | 51 (61.4) | 0.514 |
|
Positive | 8 (47.1) | 7 (52.9) |
|
| TNM stage |
|
|
|
|
I+II | 15 (30.0) | 35 (70.0) | 0.041 |
|
III+IV | 25 (50.0) | 25 (50.0) |
|
| Patient status |
|
|
|
|
Alive | 13 (25.0) | 39 (75.0) | 0.001 |
|
Succumbed | 27 (56.2) | 21 (43.8) |
|
Follow-up data for all patients was collected by
reviewing archive information, or by making visits or phone calls.
Survival time was defined as the interval between the date of
surgery and date of RCC-associated mortality. Patients who
succumbed due to reasons other than RCC were excluded from the
present study. The present study was approved by the Ethics
Committee of Tianjin Nankai Hospital.
RCC cell culture
A murine RCC cell line, Renca, was obtained from the
Cell Bank of Type Culture Collection of Chinese Academy of Sciences
(Shanghai, China). Cells were cultured in complete RPMI-1640
supplemented with 10% fetal bovine serum, 100 U/ml penicillin and
100 µg/ml streptomycin. Cells were maintained in a humidified
incubator with 5% CO2 at 37°C.
Mouse model of RCC
A total of 30 female BALB/c mice (age, 5 weeks old;
weight, 17–19 g) were purchased from Shanghai Laboratory Animal
Center (Shanghai, China). An RCC xenograft mouse model was
established by injecting Renca cells (1×106) into the
flank of the mice subcutaneously. A total of 1 week later, the mice
were treated with anti-PD-L1 (200 µg/mouse; cat. no. ab213480) and
anti-CTLA4 antibodies (200 µg/mouse, cat. no. ab134090) in
combination with PBS (n=10), anti-CD103 antibody (n=10; 200
µg/mouse; cat. no. ab25198; all Abcam, Cambridge, UK) or the
CD103+ cell growth factor Fms-related tyrosine kinase 3
ligand (FLT3L; n=10; 25 mg/kg; cat. no. bs5905; BIOSS, Beijing,
China) via tail vein injection. The treatment was performed once a
week for 4 weeks. The tumor volume and mice survival status were
checked and recorded once a day. Mice were sacrificed once tumor
volume exceeded 3,000 mm3. All mice were housed at a
temperature of 22–24°C in a specific pathogen-free room with a 12 h
light/dark cycle and free access to clean water and standard
food.
Immunostaining
Following standard procedures, the expression of
CD103 and CD8 in RCC FFPE samples was evaluated using
immunohistochemistry (IHC) and immunofluorescent staining. Briefly,
the 4-µm thick sample sections were deparaffinized with xylene and
rehydrated with ethanol, followed by microwave antigen retrieval at
95°C for 10 min. Following cooling, they were washed with distilled
water and blocked in normal 10% goat serum (Invitrogen; Thermo
Fisher Scientific, Inc., Waltham, MA, USA) at room temperature for
30 min. Subsequently, primary antibodies were added and the
sections were incubated at 4°C overnight. The primary antibodies
used were as follows: Anti-CD103 (1:100; cat. no. 14-1031-85) and
anti-CD8 (1:100; cat. no. RB-9009-P1; both Thermo Fisher
Scientific, Inc). The goat anti-mouse secondary antibody (1:500;
cat. no. ab6785; Abcam) was added and incubated at 37°C for 10 min,
followed by washing with PBS three times for 5 min. All slides were
observed under a fluorescent microscope (BZ-9000; Keyence
Corporation, Osaka, Japan) by two people independently. Five fields
of view from each section were selected randomly to calculate the
average percentage of CD8+ and CD103+ cells.
Then, the groups were given a score for CD8+ and
CD103+ expression depending on the percentage of
CD8+ and CD103+ cells, which was calculated
following cell counts and gave the following values: 1, <35%
positive; 2, 35–70% positive; and 3, >70% positive.
ELISA
ELISA was performed to evaluate the level of
interferon (IFN)-γ (cat. no. ab100690), granzyme B (cat. no.
ab46142), and PD-L1 (cat. no. ab214565) in RCC tumor tissue from
the xenograft mouse model following treatment. All ELISA kits were
purchased from Abcam. Tumor tissues harvested from the mice were
immediately lysed using radioimmunoprecipitation assay buffer
supplemented with protease inhibitor (cat. no. ab156034, Abcam).
Standard ELISA procedures were conducted according to the
manufacturer's protocol. Data were normalized to the control
group.
Fluorescence-activated cell sorting
(FACS)
FACS analysis was performed to identify the number
of CD103+ cells in the tumor tissue of the RCC mouse
model following treatment. Standard procedures were followed.
Briefly, tumor tissue harvested from the mice were cut into small
pieces and dissociated into single cells by enzymatic digestion.
Cells were carefully suspended in the residual volume (200 µl) of
staining buffer and then 200 µl freshly prepared cold fixation
buffer (Shanghai Haoran Biotechnology Co., Ltd., Shanghai, China)
was added. Cells were fixed with 70% ethyl alcohol (Shanghai Haoran
Biological Technology Co., Ltd.) for 30 min at 4°C in the dark.
Then, the sample was centrifuged at 1,000 × g for 5 min at room
temperature and the fixative was removed. To permeabilize the
cells, the cell pellet was suspended in 200 µl of freshly prepared,
pre-warmed (37°C) 0.1% Triton X-100 (Shanghai Haoran Biological
Technology Co., Ltd.) and cells were then incubated for 30 min at
37°C in the dark. Cells were subsequently centrifuged at 1,000 × g
for 5 min at room temperature and the buffer was removed. Then,
cells were incubated with anti-CD103 antibodies for 1 h on ice and
washed with PBS. Subsequently, the cells were incubated with
fluorophore-labeled goat anti-mouse secondary antibody (1:300, cat.
no. ab150117; Abcam) for 15 min at room temperature. The stained
cells were analyzed using the FACSCanto II (BD Biosciences, San
Jose, CA, USA). FlowJo software 8.0 (FlowJo, LLC, Ashland, OR, USA)
was used to analyze the data.
Statistical analysis
Data are presented as the mean ± standard deviation
of ≤3 independent experiments. All data analysis was performed
using SPSS software (version 17.0; SPSS, Inc., Chicago, IL, USA)
and GraphPad Prism 5.0 (GraphPad Software, Inc., La Jolla, CA,
USA). One-way analysis of variance followed by a Dunnett's test,
and a Student's t-test or the Chi-squared test was used to analyze
the statistical significance of differences between groups. The
Kaplan-Meier estimator method was used for survival analysis and
the log-rank test was used to compare survival curves between
different groups. The proportional hazards (Cox) regression method
was used to determine the independent prognostic impact of factors
on the survival of patients with RCC. A receiver operating
characteristic (ROC) curve was used to determine the point at which
CD103+ cell numbers were no longer positive indicators
at a high sensitivity and specificity in RCC patients and areas
under the curves (AUCs) and confidence interval (CI) were also
reported. Two-tailed P<0.05 was considered to indicate a
statistically significant difference.
Results
A higher number of CD103+
cells is associated with a later TNM stage and poorer survival in
RCC
In order to explore the role of CD103+
cells in RCC development, RCC tissue samples were collected from
patients and the number of CD103+ cells was evaluated by
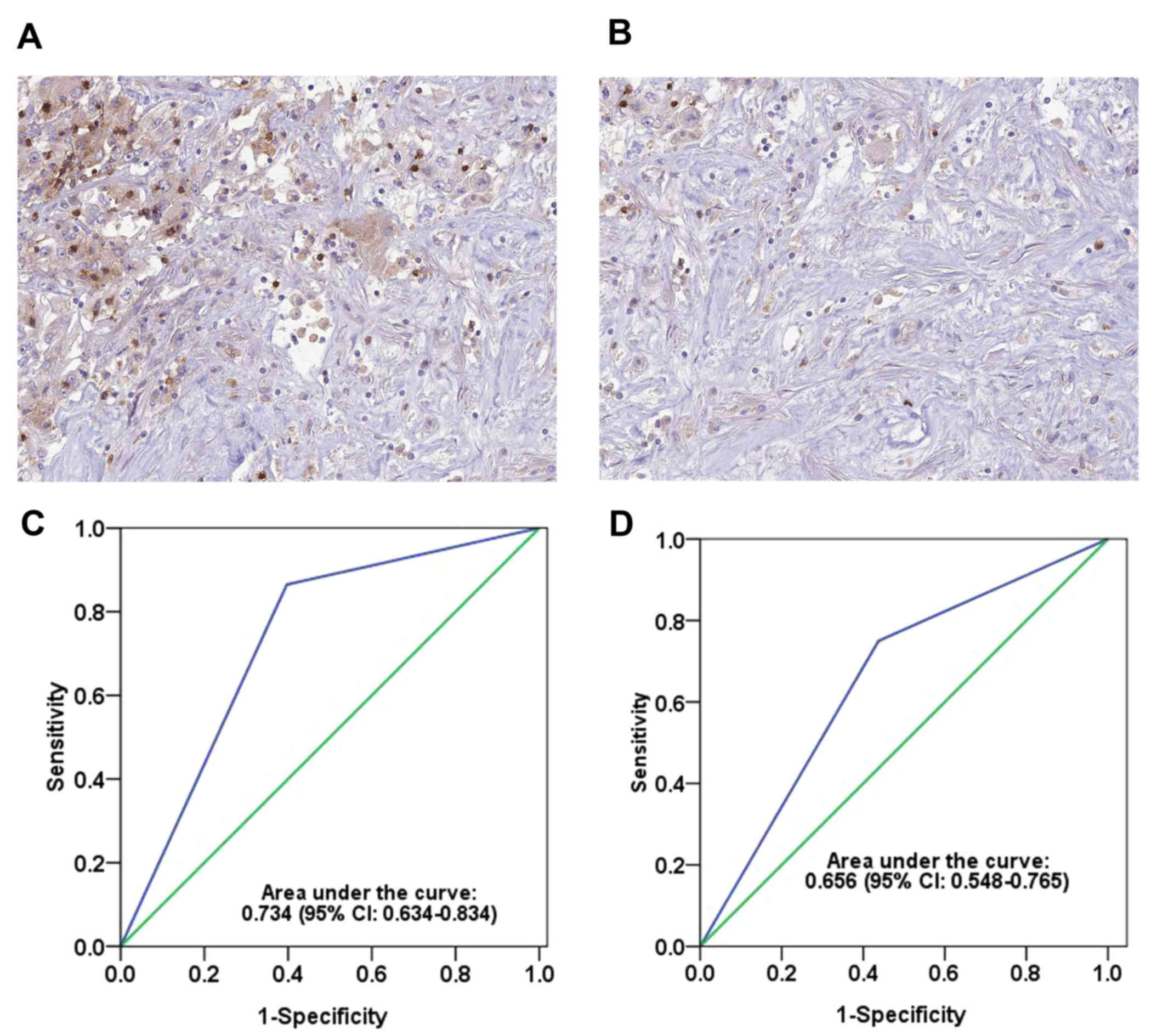
IHC. As demonstrated in Fig. 1A and
B, different levels of CD103+ cells were observed
among these patients. In order to further measure the difference
between a high and low number of CD103+ cells, patients
with RCC were randomly distributed into two groups, a training
group (n=100; average age, 61 years old) and a testing group
(n=100; average age, 62 years old) in order to eliminate any other
factors that may have effected the immune system. The proportion of
patients with advanced-stage RCC was 55% in the training cohort and
50% in the testing cohort.
According to the ROC curve analysis, a score of 2
was chosen as the cutoff point for a ‘high’ or ‘low’ number of
CD103+ cells (≥2 was determined as ‘high’; <2 was
determined as ‘low’). This cutoff point had high sensitivity and
specificity in the training [area under the curve (AUC), 0.734; 95%
CI, 0.634–0.834; Fig. 1C] and
testing (AUC, 0.656; 95% CI, 0.548–0.765; Fig. 1D) groups. Furthermore, the
association between the number of CD103+ cells and other
clinicopathological parameters was analyzed using the Chi-squared
test (Table I). The number of
CD103+ cells was similar in the training group compared
with the testing group. In the testing and training groups, an
early TNM stage was associated with a significantly higher number
of CD103+ cells compared with a later TNM stage (P=0.041
and P=0.010, respectively). Notably, the number of
CD103+ cells was also associated with the survival of
RCC patients: Patients who succumbed to RCC had a significantly
lower number of CD103+ cells compared with patients who
survived at the end of our research (P<0.001 in the training
group; P=0.001 in the testing group).
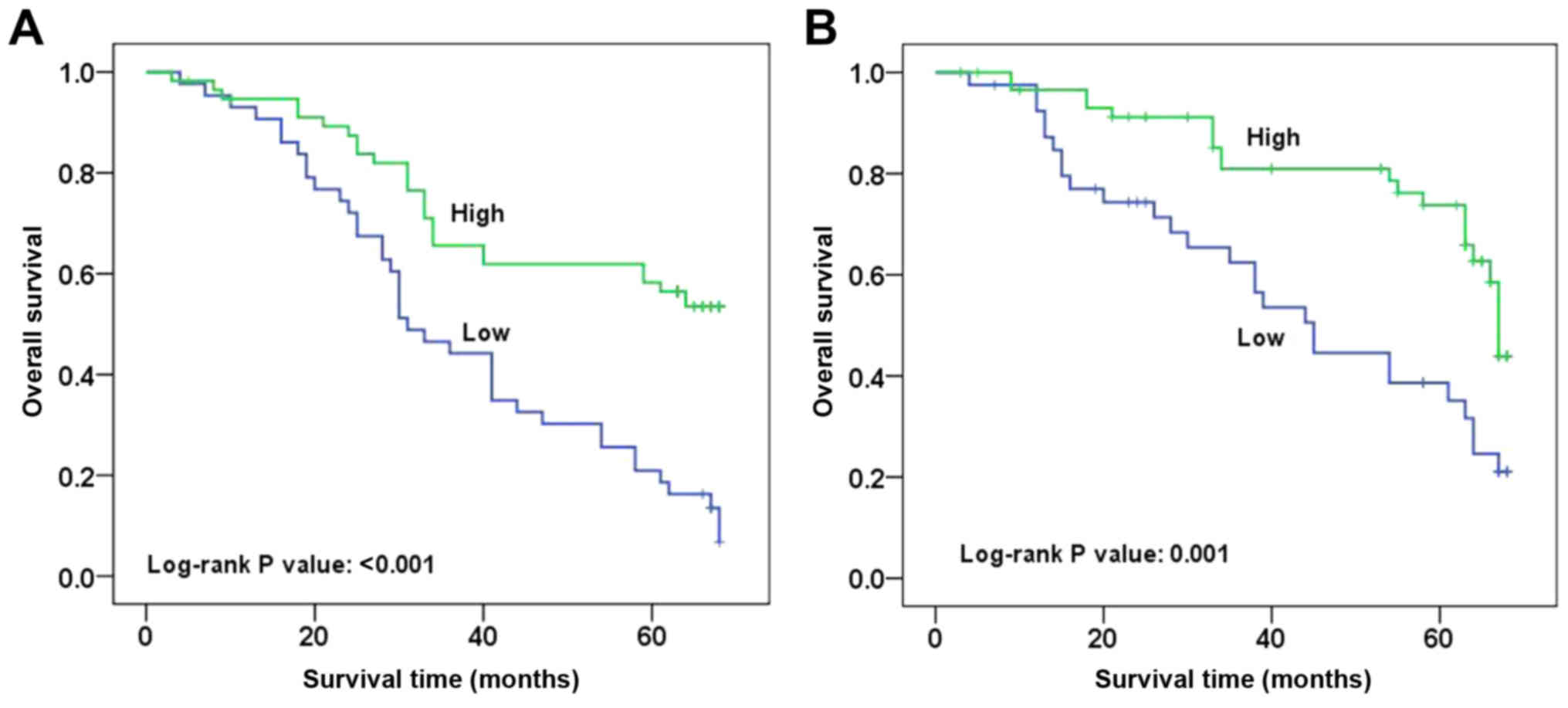
A high number of CD103+
cells is a favorable prognosticator for patients with RCC
The difference in the number of CD103+
cells among patients with RCC and its association with outcome
suggested that CD103+ cells could serve a key role in
the progression of RCC. Thus, follow-up data was obtained for these
patients and survival analysis was performed. As shown in Fig. 2, typical survival curves were
observed for patients with RCC with high or low numbers of
CD103+ cells. Patients with a high number of
CD103+ cells had a significantly longer survival rate
compared with those with a low number of CD103+ cells in
the training and testing groups (P<0.001 and P=0.001,
respectively). Furthermore, Cox regression analysis indicated that
a high number of CD103+ cells was an independent
predictor of good survival in patients with RCC when other
clinicopathological features were not predictors of survival
(P=0.001 in the training group, P=0.003 in the testing group;
Table II). Consistent results for
CD103+ expression were observed in the training [hazard
ratio (HR), 0.365; 95% CI, 0.205–0.648] and testing (HR, 0.391; 95%
CI, 0.210–0.728) groups (Table
II).
| Table II.Multivariate Cox regression analysis
of the overall survival of patients with renal cell carcinoma. |
Table II.
Multivariate Cox regression analysis
of the overall survival of patients with renal cell carcinoma.
| A, Training group
(n=100) |
|---|
|
|---|
| Clinicopathological
feature | P-value | HR (95% CI) |
|---|
| Age (≥60 vs. <60
years) | 0.120 | 1.532
(0.895–2.621) |
| Gender (male vs.
female) | 0.267 | 0.734
(0.425–1.267) |
| T stage (T3-T4 vs.
T1-T2) | 0.097 | 1.664
(0.911–3.040) |
| Lymph node (N3-N4
vs. N0-N2) | 0.092 | 1.601
(0.926–2.767) |
| Metastasis
(positive vs. negative) | 0.368 | 1.399
(0.673–2.906) |
| TNM stage (III–IV
vs. I–II) | 0.619 | 1.163
(0.641–2.112) |
| Grade (III+IV vs.
I+II) | 0.064 | 1.6681
(0.970–2.913) |
| CD103expression
(high vs. low) | 0.001 | 0.365
(0.205–0.648) |
|
| B, Testing group
(n=100) |
|
|
Clinicopathological feature | P-value | HR (95%
CI) |
|
| Age (≥60 vs. <60
years) | 0.995 | 0.998
(0.535–1.861) |
| Gender (male vs.
female) | 0.555 | 1.211
(0.641–2.288) |
| T stage (T3-T4 vs.
T1-T2) | 0.946 | 1.000
(0.549–1.820) |
| Lymph node (N3-N4
vs. N0-N2) | 0.063 | 1.801
(0.968–3.349) |
| Metastasis
(positive vs. negative) | 0.595 | 0.804
(0.360–1.795) |
| TNM stage (III–IV
vs. I–II) | 0.776 | 0.910
(0.475–1.743) |
| Grade (III+IV vs.
I+II) | 0.233 | 1.460
(0.784–2.718) |
| CD103 expression
(high vs. low) | 0.003 | 0.391
(0.210–0.728) |
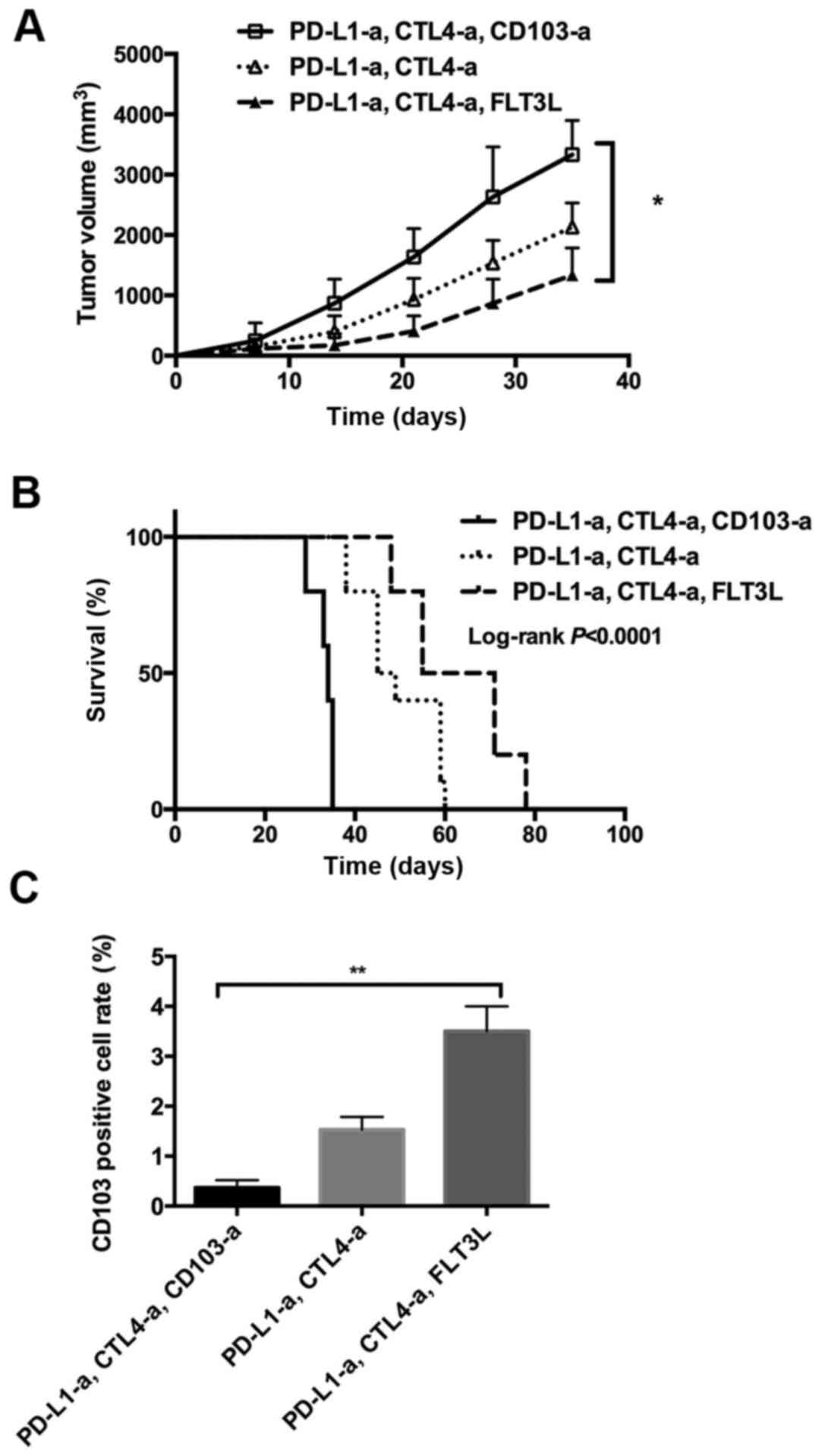
CD103 depletion inhibits the effects
of ICBT in an RCC animal model
In order to further explore the role of
CD103+ cells in RCC development, a RCC xenograft mouse
model was established using a murine RCC cell line, Renca. In this
animal model, the tumors of the mice administered with ICBT
(anti-PD-L1 and anti-CTL40a antibodies) and anti-CD103 antibodies
grew faster compared with the mice administered with ICBT and PBS
(Fig. 3A). Notably, following
administration with ICBT and FLT3L, tumor growth was significantly
inhibited compared with the group that received ICBT and anti-CD103
antibodies (P<0.05; Fig. 3A).
Furthermore, mice that received ICBT and anti-CD103 antibodies had
a significantly shorter survival time compared with the mice
administered ICBT treatment with PBS or those administered ICBT and
FLT3L (both P<0.01; Fig. 3B). In
addition, a decreased number of CD103+ cells were
observed within the tumor tissue of mice that received ICBT and
anti-CD103 antibodies, and a significantly increased number of
CD103+ cells were observed in the mice administered ICBT
and FLT3L treatment, compared with mice administered with ICBT
treatment with PBS (both P<0.01; Fig.
3C). These data suggest that CD103+ cells serve a
key role in suppressing the development of RCC in an immune
response-dependent manner.
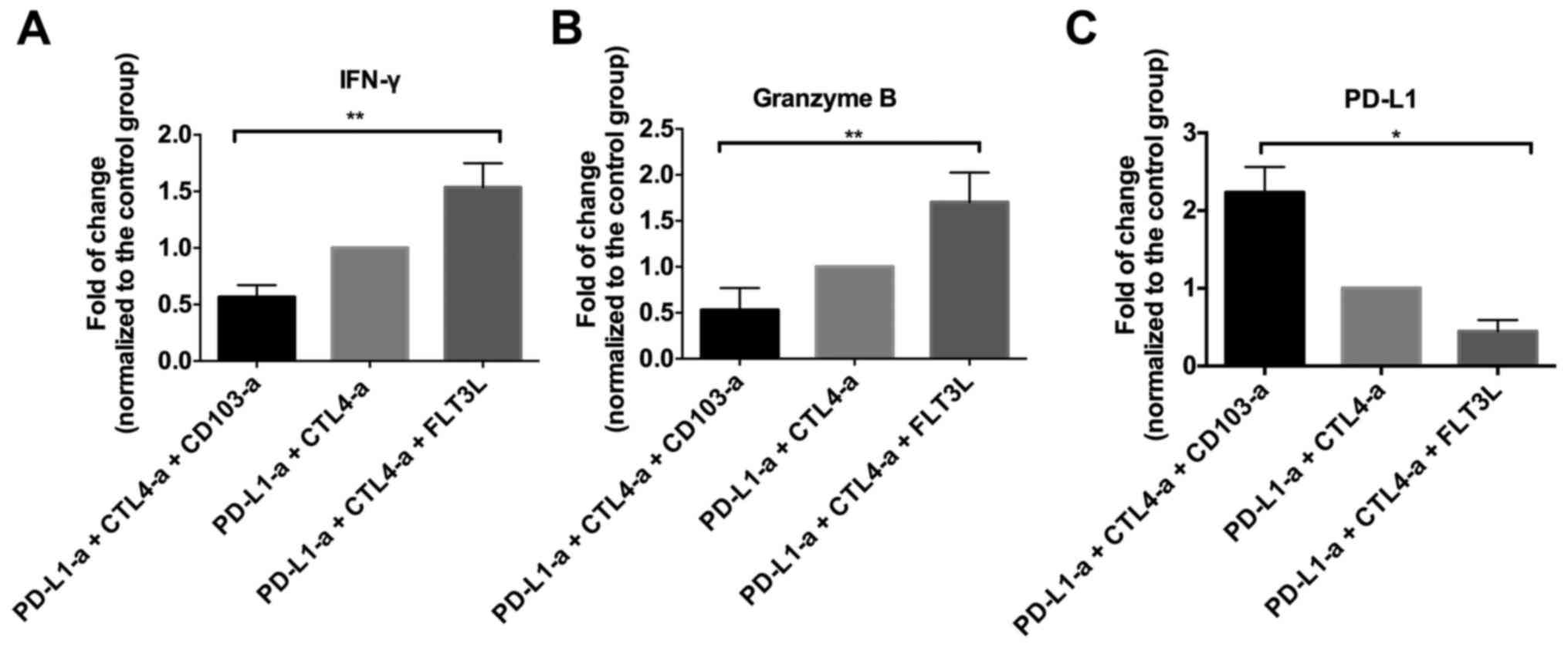
CD103+ cells promote the
function of CD8+ T cells
Based on the proposal that CD103+ cells
may work synergistically with tumor immunity to suppress the
development of RCC in an animal model, T cell functions were
investigated further in these mice. As demonstrated in Fig. 4, varying levels of CD8+ T
cell infiltration were identified in different groups of mice. The
quantitative analysis indicated that the mice that received ICBT
and CD103 depletion had a significantly decreased number of
CD8+ T-cells, while the mice administered FLT3L and ICBT
treatment had a significantly increased number of CD8+
T-cells, compared with the group administered with ICBT treatment
and PBS (both P<0.0001; Fig. 4D).
Similar trends were observed in the level of IFN-γ and granzyme B
in tumor tissue (Fig. 5A and B). In
addition, a significantly increased PD-L1 level was observed in the
tumor tissue of mice administered ICBT and anti-CD103 treatment,
but a significantly decreased level of PD-L1 was observed in mice
administered with ICBT and FLT3L treatment, compared with the group
administered with ICBT treatment and PBS (P<0.05; Fig. 5C).
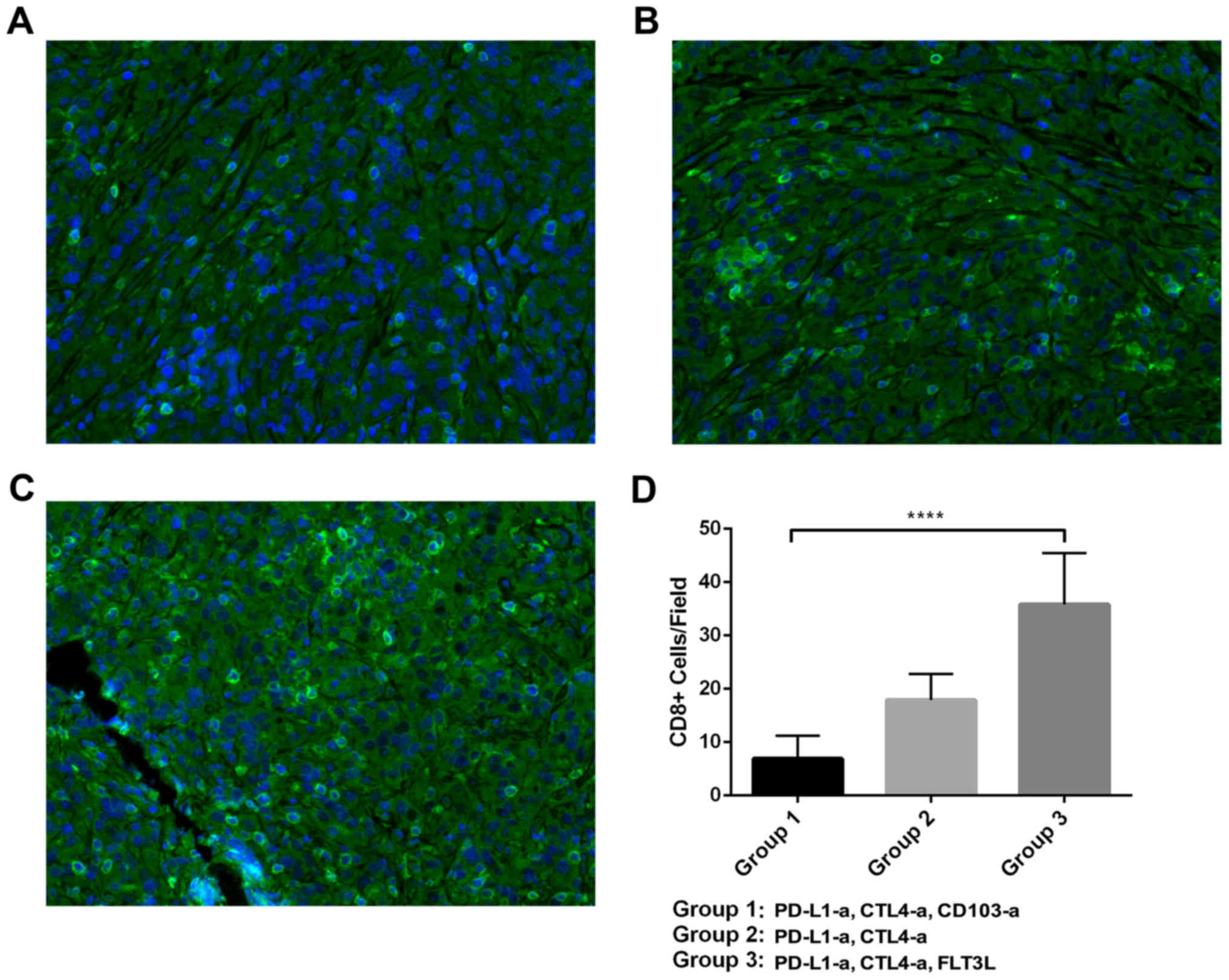 | Figure 4.Tumor infiltrating CD8+ T
cells in a RCC xenograft mouse model. (A-C) Representative images
of CD8+ T cells in the tumor tissue of RCC mice treated
with ICBT and anti-CD103 antibodies, ICBT alone, or ICBT and FLT3L.
Magnification, ×400. (D) Quantitative analysis of CD8+ T
cells in the RCC xenograft mouse model. RCC, renal cell carcinoma;
ICBT, immune checkpoint blockade therapy; -a, antibody; PD-L1,
programmed cell death ligand 1; CTLA4, cytotoxic
T-lymphocyte-associated protein 4; FLT3L, Fms-related tyrosine
kinase 3 ligand; CD, cluster of differentiation.
****P<0.0001. |
Discussion
The tumor microenvironment influences tumor
initiation and progression (17).
Among the large spectrum of tumor stromal cells, immune cells are
critical in restricting cancer development (11). However, tumors have been indicated to
suppress the antitumor immune response via stimulating inhibitory
immune checkpoints (6). Thus,
targeting these inhibitory immune checkpoints to release inhibition
of tumor immunity may benefit patients with cancer. An example of a
strategy that uses immune checkpoints is ICBT, which has achieved
significant clinical benefits. However, the majority of patients
with cancer such as glioma do not respond to ICBT (5–6).
Previous studies have demonstrated that CD103+ dendritic
cells are the only antigen-presenting cells that transport intact
antigens to the lymph nodes and prime tumor-specific
CD8+ T cells in melanoma (18–20).
Furthermore, previous studies have revealed that a high
CD103+ cell count is a favorable marker for patients
with various types of cancer, including lung (11), ovarian (21) and bladder (21) cancer. However, the role of
CD103+ cells in RCC remains unknown.
The current study identified that CD103+
cell count was associated with the outcome of patients with RCC.
Patients with RCC with adverse outcomes tended to have a low
CD103+ cell count in the tumor stroma. Survival analysis
based on the follow-up data of a large number of patients with RCC
was consistent with this, indicating that patients with high CD103
expression had longer survival times. In addition, multivariate
analysis identified that high CD103 expression was an independent
favorable prognostic factor for patients with RCC. To the best of
our knowledge, this is the first report to reveal the prognostic
value of CD103+ cells in RCC. These findings are
consistent with previous studies that reported that
CD103+ cells are protective in various cancer types
(11,20,21).
These results suggest a potential therapeutic benefit of expanding
CD103+ cells in an RCC animal model.
In order to further explore the role of
CD103+ cells in tumor immunity in RCC, CD103+
cells were expanded or depleted in an RCC mouse model. The results
demonstrated that the expansion of CD103+ cells could
enhance the response to ICBT, which is consistent with the results
of previous studies in other tumor types, including melanoma and
breast cancer (19,20,22).
Notably, the number of tumor infiltrating CD8+ T cells
was increased after treatment with a growth factor of
CD103+ cells. Furthermore, activation of these
CD8+ T cells was observed, indicated by significantly
increased levels of IFN-γ and granzyme B. As CD8+ T
cells are the major effector cells of tumor immunity, these results
suggest that CD103+ cells are required for the
activation of tumor-specific cytotoxic T cells in RCC. This is
consistent with previous reports that demonstrated that
CD103+ cells have unique antigen processing and
presentation capabilities, and act as superior stimulators of naïve
and activated CD8+ T cells (10,23). In
addition, in the present study, anti-CD103 treatment inhibited the
effects of ICBT, decreased the number of tumor infiltrating
CD8+ T cells, and decreased IFN-γ and granzyme B levels.
These results indicate that CD103+ cells may act as a
key ‘switch’ for regulating tumor immunity.
Advances in cancer immunology make this an exciting
time to research and treat cancer. However, the insensitivity of
certain tumors, including RCC, to immune responses restricts the
use of immunotherapies. The results of the present study indicate
that a high CD103+ cell count is an independent
favorable prognostic factor in patients with RCC. Thus, the
expansion of CD103+ cells may increase the efficacy of
ICBT in patients with RCC.
Acknowledgements
The present study was supported by Tianjin Nankai
Hospital (Tianjin, China).
References
|
1
|
Quail DF and Joyce JA: Microenvironmental
regulation of tumor progression and metastasis. Nat Med.
19:1423–1437. 2013. View
Article : Google Scholar : PubMed/NCBI
|
|
2
|
Banerjee S, Modi S, McGinn O, Zhao X,
Dudeja V, Ramakrishnan S and Saluja AK: Impaired synthesis of
stromal components in response to minnelide improves vascular
function, drug delivery and survival in pancreatic cancer. Clin
Cancer Res. 22:415–425. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chen DS and Mellman I: Oncology meets
immunology: The cancer-immunity cycle. Immunity. 39:1–10. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ott PA, Hodi FS and Robert C: CTLA-4 and
PD-1/PD-L1 blockade: New immunotherapeutic modalities with durable
clinical benefit in melanoma patients. Clin Cancer Res.
19:5300–5309. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Brahmer JR, Drake CG, Wollner I, Powderly
JD, Picus J, Sharfman WH, Stankevich E, Pons A, Salay TM, McMiller
TL, et al: Phase I study of single-agent anti-programmed death-1
(MDX-1106) in refractory solid tumors: Safety, clinical activity,
pharmacodynamics and immunologic correlates. J Clin Oncol.
28:3167–3175. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Topalian SL, Hodi FS, Brahmer JR,
Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD,
Sosman JA, Atkins MB, et al: Safety, activity and immune correlates
of anti-PD-1 antibody in cancer. N Engl J Med. 366:2443–2454. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
El-Asady R, Yuan R, Liu K, Wang D, Gress
RE, Lucas PJ, Drachenberg CB and Hadley GA: TGF-{beta}-dependent
CD103 expression by CD8+ T cells promotes selective destruction of
the host intestinal epithelium during graft-versus-host disease. J
Exp Med. 201:1647–1657. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kilshaw PJ and Murant SJ: A new surface
antigen on intraepithelial lymphocytes in the intestine. Eur J
Immunol. 20:2201–2207. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Evers BD, Engel DR, Böhner AM, Tittel AP,
Krause TA, Heuser C, Garbi N, Kastenmuller W, Mack M, Tiegs G, et
al: CD103+ kidney dendritic cells protect against crescentic GN by
maintaining IL-10-producing regulatory t cells. J Am Soc Nephrol.
27:3368–3382. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Floc'h AL, Jalil A, Vergnon I, Le Maux
Chansac B, Lazar V, Bismuth G, Chouaib S and Mami-Chouaib F: Alpha
E beta 7 integrin interaction with E-cadherin promotes antitumor
CTL activity by triggering lytic granule polarization and
exocytosis. J Exp Med. 204:559–570. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Djenidi F, Adam J, Goubar A, Durgeau A,
Meurice G, de Montpréville V, Validire P, Besse B and Mami-Chouaib
F: CD8+CD103+ tumor-infiltrating lymphocytes are tumor-specific
tissue-resident memory T cells and a prognostic factor for survival
in lung cancer patients. J Immunol. 194:3475–3486. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Le Floc'h A, Jalil A, Franciszkiewicz K,
Validire P, Vergnon I and Mami-Chouaib F: Minimal engagement of
CD103 on Cytotoxic T lymphocytes with an E-cadherin-Fc molecule
triggers lytic granule polarization via a phospholipase
Cgamma-dependent pathway. Cancer Res. 71:328–338. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rini BI, Campbell SC and Escudier B: Renal
cell carcinoma. Lancet. 373:1119–1132. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jonasch E, Gao J and Rathmell WK: Renal
cell carcinoma. BMJ. 349:g47972014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sharma P, Wagner K, Wolchok JD and Allison
JP: Novel cancer immunotherapy agents with survival benefit: Recent
successes and next steps. Nat Rev Cancer. 11:805–812. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cohen M: Comparing relaxation training and
cognitive-behavioral group therapy for women with breast cancer.
Res Social Work Pract. 17:313–323. 2007. View Article : Google Scholar
|
|
17
|
Chan AC, Fan ST, Poon RT, Cheung TT, Chok
KS, Chan SC and Lo CM: Evaluation of the seventh edition of the
American Joint Committee on Cancer tumour-node-metastasis (TNM)
staging system for patients undergoing curative resection of
hepatocellular carcinoma: Implications for the development of a
refined staging system. HPB (Oxford). 15:439–448. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zhao X, He Y and Chen H: Autophagic tumor
stroma: Mechanisms and roles in tumor growth and progression. Int J
Cancer. 132:1–8. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Broz ML, Binnewies M, Boldajipour B,
Nelson AE, Pollack JL, Erle DJ, Barczak A, Rosenblum MD, Daud A,
Barber DL, et al: Dissecting the tumor myeloid compartment reveals
rare activating antigen-presenting cells critical for T cell
immunity. Cancer Cell. 26:638–652. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Salmon H, Idoyaga J, Rahman A, Leboeuf M,
Remark R, Jordan S, Casanova-Acebes M, Khudoynazarova M, Agudo J,
Tung N, et al: Expansion and activation of CD103+ dendritic cell
progenitors at the tumor site enhances tumor responses to
therapeutic PD-L1 and BRAF inhibition. Immunity. 44:924–938. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Webb JR, Milne K and Nelson BH: Location,
location, location: CD103 demarcates intraepithelial,
prognostically favorable CD8+ tumor-infiltrating lymphocytes in
ovarian cancer. Oncoimmunology. 3:e276682014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wang B, Wu S, Zeng H, Liu Z, Dong W, He W,
Chen X, Dong X, Zheng L, Lin T and Huang J: CD103+ tumor
infiltrating lymphocytes predict a favorable prognosis in
urothelial cell carcinoma of the bladder. J Urol. 194:556–562.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Liu Y and Cao X: Intratumoral dendritic
cells in the anti-tumor immune response. Cell Mol Immunol.
12:387–390. 2015. View Article : Google Scholar : PubMed/NCBI
|