Introduction
Tuberculosis is an infectious disease caused by
Mycobacterium tuberculosis (MTB), which is a serious threat
to people's health all over the world. According to the WTO's
report, 1/3 of people infected with MTB, and about 1.7 million
people die each year from tuberculosis and related diseases
(1). Therefore, the rapid and
accurate diagnosis of tuberculosis is critical for the treatment of
tuberculosis. The sensitivity and specificity of traditional
methods of detection (anti-acid stains smear, MTB culture,
tuberculin skin test, tuberculosis antibody detection, MTB DNA
detection) in the diagnosis of tuberculosis are limited. MTB
isolation and culture test is the gold standard for the diagnosis
of tuberculosis, but it takes a long time with little significance
for early diagnosis, and it is difficult in sampling
extra-pulmonary tuberculosis. In recent years,
tuberculosis-specific T cell immunity in vitro detection
method γ-interferon in vitro release test interferon-γ
release assay (IGRA), is gradually promoted and applied to clinic
(2–4). This method is not affected by Bacillus
Calmette-Guérin (BCG) vaccination and most non-tuberculosis
mycobacterial infections in China, where BCG vaccination has a very
good application prospects (5). In
the present study, a domestic TB IFN-γ release assay (HGN, Wuhan,
China), was used as it is much cheaper than the imported IGRAs,
QFT-GIT and T-SPOT.TB. It is licensed by the China Food and Drug
Administration (CFDA), and a cheap and high-quality assay that will
be constructive to the clinical application of IGRA and
accumulating more clinical data for indicating its clinical value
in developing countries with high TB burden. This study reviewed
the results of interferon-γ release assays (IGRAs) in 737 suspected
tuberculosis patients in the above hospital from January 2016 to
April 2016, and explored its diagnostic value and significance for
active tuberculosis.
Patients and methods
Participants and samples
In total 740 patients with tuberculosis interferon
release test admitted to The First Affiliated Hospital of Sun
Yat-sen University (Guangzhou, China) in the period of
January-April 2016, were recruited into the study. The age
distribution was 1–96 years, including 737 cases of qualified
specimens, 431 cases of male patients, hemolytic specimens 0 cases,
lipid turbidity specimens 3 cases (Table
I).
 | Table I.Demographic and clinical
characteristics of the 737 patients. |
Table I.
Demographic and clinical
characteristics of the 737 patients.
| Characteristics | Active TB | Non-active TB | P-value |
|---|
| Case number | 87 | 650 |
|
| Age, median (range),
years | 46 (32–62) | 58 (45–67) | 0.001 |
| Sex
(male/female) | 58/29 | 373/277 | 0.062 |
| Evidence of previous
TB (%) | 2 (2.3%) | 18 (2.8%) | 0.353 |
| Blood tests (median,
IQR) |
|
Lymphocytes
(×109/l) | 2.02 (0.78–1.68) | 1.70 (1.06–2.18) | 0.68 |
| ESR
(mm/h) | 42 (9–66) | 30 (15–49) | 0.003 |
| CRP
(mg/l) | 19.00
(1.84–62.00) | 12.00
(4.00–40.00) | 0.032 |
| PCT
(ng/ml) | 8.08
(0.05–74.25) | 0.34 (0.05–0.27) | 0.009 |
This study was reviewed and approved by the
Institutional Review Board of The First Affiliated Hospital of Sun
Yat-sen University according to the guidelines of Helsinki
Declaration. The study was approved by the Ethics Committee of The
First Affiliated Hospital, Sun Yat-Sen University. Patients who
participated in this research had complete clinical data. The
signed informed consents were obtained from the patients or the
guardians.
Diagnostic criteria
Combined with clinical manifestations, clinical
imaging, etiology and pathology data, the patients were divided
into three categories: i) Confirmed active tuberculosis group:
Smear positive for acid-fast bacilli, or MTB culture positive,
pathological results suggesting granulomatous inflammation with
coagulation necrosis; ii) Clinically diagnosed active tuberculosis
group: The patients with suspected tuberculosis were treated with
anti-tuberculosis therapy or follow-up observation, their features
consistent of clinical and imaging findings of typical
tuberculosis, but not confirmed by etiology and pathology, and
clinicians excluded other non-tuberculous diseases; iii) Non-active
tuberculosis group: pathological findings were clear for tumors,
inflammation or other diseases, and excluded MTB infection, or
clinical diagnosis for other diseases, by the corresponding
treatment or follow-up observation (6). Clinicians excluded MTB infection
through past history, clinical manifestations and laboratory
examinations of the patients.
Detection method
IGRAs
For IGRAs, whole blood was collected from each
patient and inoculated in three heparinized tubes of 1 ml: each one
containing TB antigens (ESAT-6 and CFP-10), a positive control tube
containing phytohemagglutinin, and a null control. Blood samples
were incubated for 20–24 h at 37°C. Plasma samples were then
harvested for IFN-γ quantification by a single-step sandwich-type
ELISA. The test was performed according to manufacturer's
instructions (HyGeianey). Optical densities were interpreted by
using specific software provided by the manufacturer. The result
was considered to be positive if the IFN-γ level after stimulation
with TB antigens minus negative control was ≥0.35 IU/ml and ≥25% of
the negative control. The test was considered negative if the IFN-γ
level was <0.35 IU/ml (after subtraction of the negative
control). The test result was considered to be indeterminate if the
negative control was ≥8.0 IU/ml or the positive control minus
negative control was <0.5 IU/ml (Table II).
| Table II.The result judgement of IGRAs. |
Table II.
The result judgement of IGRAs.
| N (IU/ml) | P-N (IU/ml) | T-N (IU/ml) | Result judgement |
|---|
| ≤8 | Any value | ≥0.35 and ≥N/4 | Positive |
|
| ≥0.5 | <0.35 | Negative |
|
| ≥0.5 | ≥0.35 but
<N/4 |
|
|
| <0.5 | <0.35 | Indeterminate |
|
| <0.5 | ≥0.35 but
<N/4 |
|
| >8 | Any value | Any value |
|
Detection of MTB IgG antibody
Test operation and interpretation of the results
were in strict accordance with the instructions of MTB IgG antibody
detection kit (MP Biomedical Asia Pacific Limited).
TST
Patients were injected with 0.1 ml of tuberculin [2
tuberculin units of pure protein derivatives (PPD)] in accordance
with the American Thoracic Society guidelines. The skin induration
was measured at 48–72 h after the inoculation. The size of the
induration equal or higher than 5 mm was considered positive. A
previous BCG vaccination did not change the size limits for the
tuberculin reaction. The result was considered to be invalid or not
read, if the patient did not come to be measured or could not be
contacted. All patients with a positive tuberculin test who had not
been previously treated, received chemoprophylaxis with isoniazid
for 6–9 months.
Statistical analysis. The statistical software
package SPSS 22.0 (IBM Corp., Armonk, NY, USA) was used for data
analysis to draw the ROC curve for the diagnosis value of IGRAs.
Statistical comparisons were made by using the t-test to assess the
difference between two proportions. Tests of statistical
significance included the 95% confidence intervals of unadjusted
relative risks. Values <0.05 were considered statistically
significant. Sensitivity, specificity, positive predictive value,
negative predictive value, positive likelihood ratio and negative
likelihood ratio, and the 95% confidence interval of the
corresponding indicators, were calculated to evaluate diagnostic
performance of IGRAs by Medical software. The data were reviewed by
laboratory quality-control staff, and data entry was performed by
two independent persons. Most important, confirmed indeterminate
samples were not enrolled into calculation in any equation.
Results
Of the 737 patients who did receive IGRA, 87 cases
were diagnosed with active tuberculosis (30 cases with confirmed
active tuberculosis, 58 cases with clinically diagnosed active
tuberculosis) and 650 cases non-active tuberculosis. The total
sensitivity of IGRAs of active tuberculosis was 90.80% (79/87, 95%
CI, 82.68–95.95), with specificity of 76.62% (498/650, 95% CI,
73.17–79.82), positive predictive value of 34.18% (95% CI3.33–4.53)
and the negative predictive value was 98.7% (498/506, 95% CI,
97.44–99.40), the positive likelihood ratio was 3.88, the negative
likelihood compared to 0.12. Table
III shows the results of IGRAS, TST, TB-IgG test results, the
sensitivity and specificity of the differences were statistically
significant (P<0.05).
| Table III.Diagnostic efficacy of results of
IGRAs, TST and TB-IgG. |
Table III.
Diagnostic efficacy of results of
IGRAs, TST and TB-IgG.
| Test | Sensitivity, % (95%
CI) | Specificity, % (95%
CI) | PPV, % (95% CI) | NPV, % (95% CI) |
|---|
| IGRAs | 90.80
(82.68–95.95) | 76.62
(73.17–79.82) | 34.18
(33.33–34.53) | 98.66
(97.44–99.40) |
| TST | 75.45
(68.38–88.02) | 72.27
(57.11–85.53) | 50.95
(44.48–66.54) | 88.52
(84.48–89.84) |
| TB-IgG | 40.00
(26.41–54.2) | 74.47
(59.65–86.06) | 11.16
(6.25–19.85) | 96.75
(85.25–99.85) |
| TST combined
TB-IgG | 85.27
(74.61–92.72) | 53.81
(43.77–63.84) | 16.06
(13.01–19.21) | 97.24
(93.01–99.26) |
Among the 79 cases of active tuberculosis (including
confirmed active tuberculosis and clinical diagnosed active
tuberculosis), 8 were confirmed by pathogenicity as tuberculosis
and the remaining 71 were smear-negative tuberculosis. The
sensitivity of IGRAs to detect smear positive tuberculosis was 100%
(8/8), and 88.73% (63/71) in the detection of smear-negative
tuberculosis, and there was no significant difference
(P>0.05).
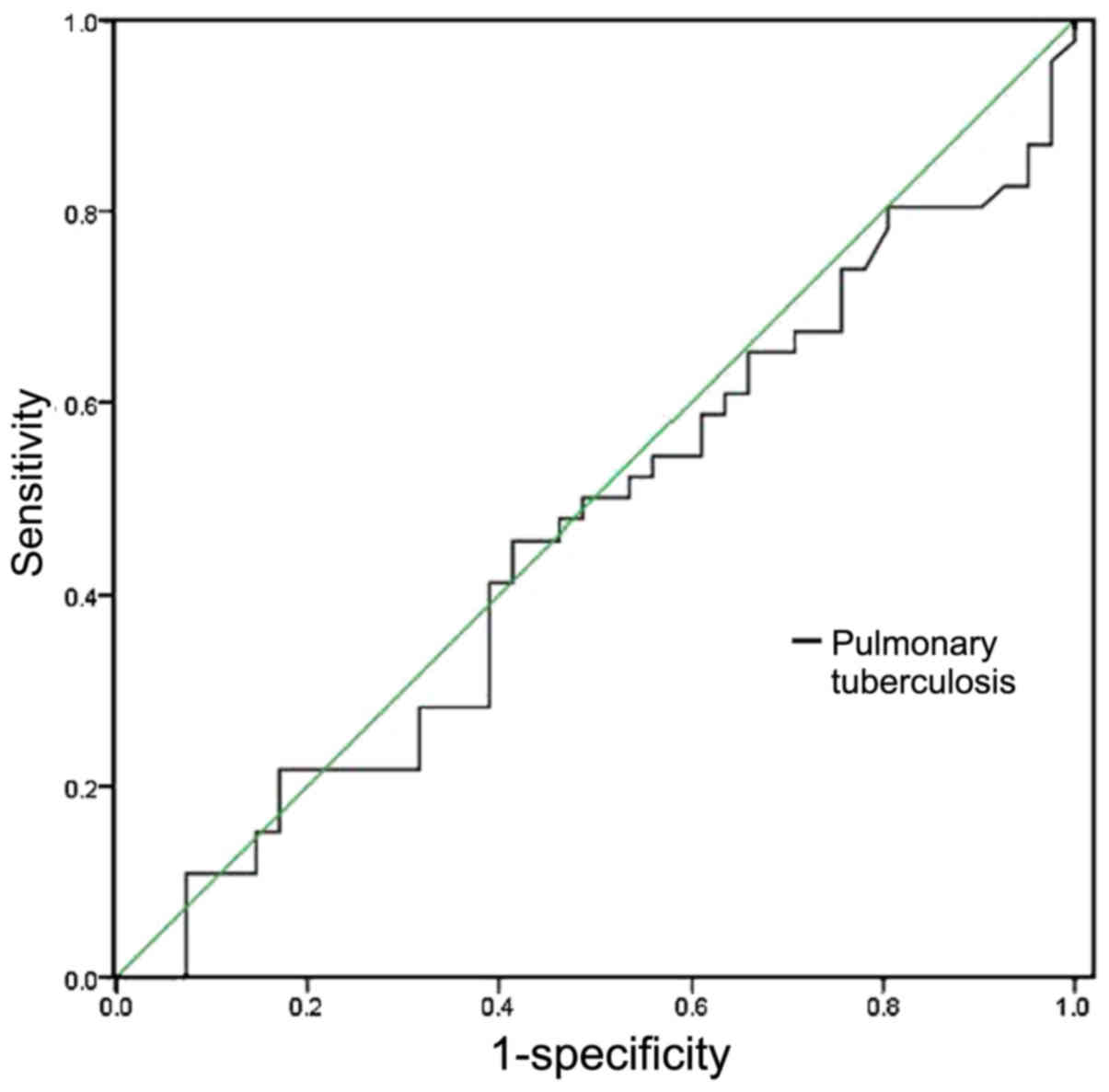
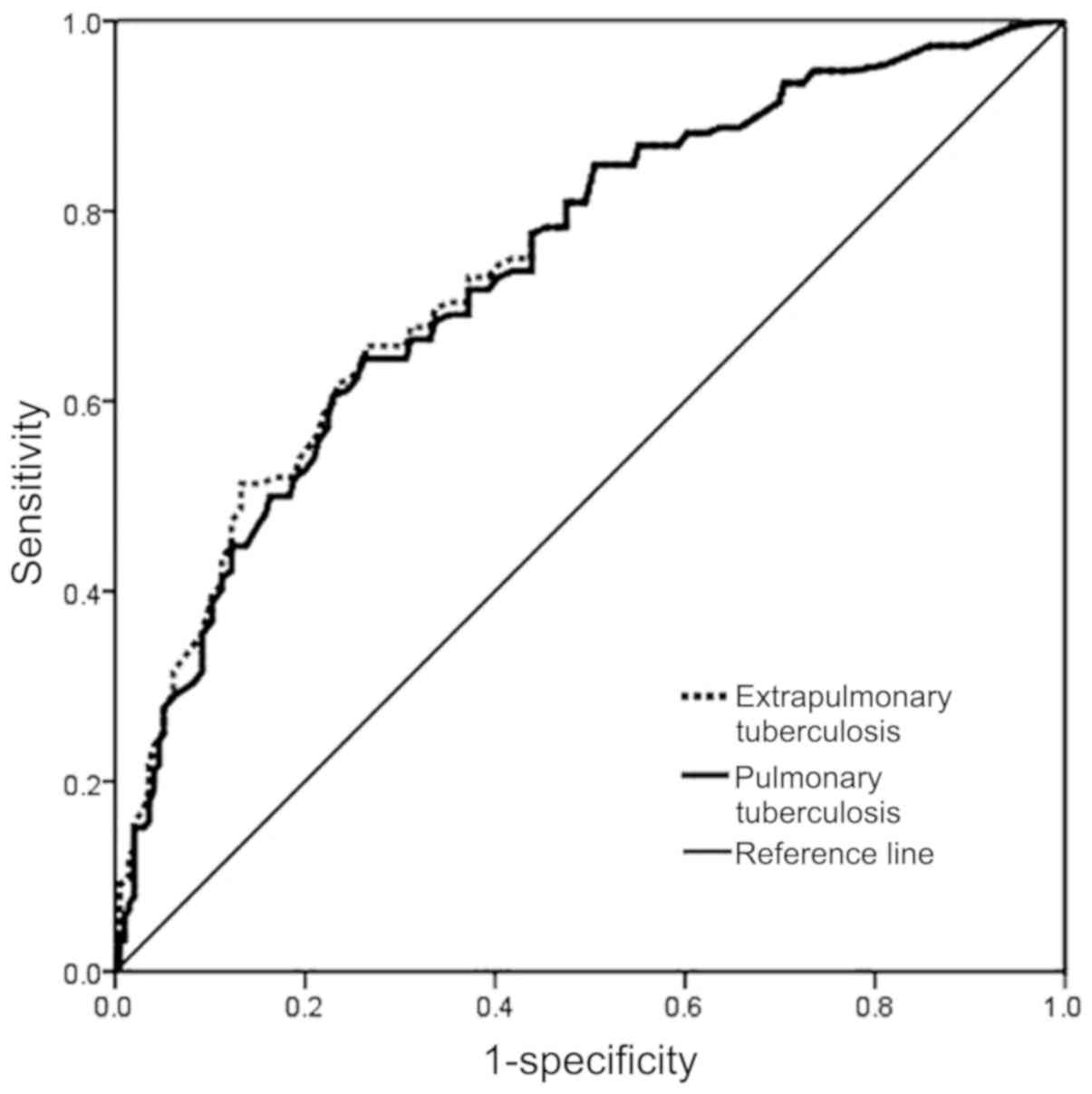
The sensitivity of IGRAs to detect active pulmonary
tuberculosis was 85.7% (36/42), and the sensitivity of
extra-pulmonary tuberculosis (including tuberculous pleurisy,
intestinal tuberculosis, lumbar tuberculosis, bone and joint
tuberculosis and tuberculous meningitis) was 94.4% (34/36), the
sensitivity of pulmonary tuberculosis with extrapulmonary
tuberculosis was 100% (9/9). It was not statistically significant
(P>0.05) (Table IV).
| Table IV.Comparison of sensitivity of IGRA test
to different tuberculosis. |
Table IV.
Comparison of sensitivity of IGRA test
to different tuberculosis.
| Groups | IGRAs positive | IGRAs negative |
|---|
| Pulmonary
tuberculosis | 36 | 6 |
| Extra pulmonary
tuberculosis | 34 | 2 |
| Tuberculous
pleurisy | 14 | 1 |
| Lumbar
tuberculosis | 4 | 1 |
| Intestinal
tuberculosis | 8 | 0 |
| Tuberculosis of bone
and joint | 2 | 0 |
| Other extra pulmonary
tuberculosis | 6 | 0 |
| Pulmonary
tuberculosis with extrapulmonary tuberculosis | 9 | 0 |
According to the value of T-N detected by IGRAs, we
performed ROC curve analysis (Fig.
1), and the area under the curve was 0.878 (95% CI,
0.839–0.917), suggesting that IGRAs has a good application value in
the diagnosis of active tuberculosis infection. N refers to a null
control of interferon concentration in each patient, and T refers
to the interferon concentration stimulated by tuberculosis antigen
in the curve. Fig. 2 shows the ROC
curve for the diagnosis of active pulmonary tuberculosis and
extrapulmonary tuberculosis, with the area under the curve being
0.839 and 0.841, respectively.
Discussion
Early diagnosis and treatment of tuberculosis has
become a key factor in tuberculosis control (7–9).
However, the positive rate of smear detection of acid-fast bacilli
is very low, and the culture cycle of MTB is long, so they are not
suitable for early diagnosis. The diagnostic value of
microbiological methods is very limited. In this study, only 8
cases were smear positive for detection of acid-fast bacilli of 87
cases of active tuberculosis. TST can be used to diagnose
tuberculosis quickly, but at the same time some antigenic
components of the BCG pure protein derivative used in the TST are
the same as those of BCG and most of the non-tuberculosis
mycobacteria, and they are prone to cross-reactivity, making for
high false-positive rate and low diagnostic specificity; while the
response degree of the organism to PPD is affected by the state of
the immune system, thus lacking sufficient sensitivity (10,11). The
detection of TB-IgG was influenced by the antigen processing,
immunoassay method, and the immune response of the body, which have
a great impact on the sensitivity and specificity of the test
results (12).
IGRAs, developed in recent years based on the T cell
immune response, have been shown to be more sensitive and specific
in tuberculosis diagnosis. Meta-analysis of relevant literature and
data from 1966 to 2006 by Menzies et al (13) showed that IGRA were more sensitive
than TST in the diagnosis of tuberculosis. Domestic IGRAS research
data show that the difference of the sensitivity and specificity is
large, with the sensitivity of 53–98% floating, specificity of
60–90% (or above), but most of the literature reported sensitivity
and specificity greater than 70%, showing that the specificity of
IGRAs is better than PPD test (14).
The results of this study show that the total sensitivity of IGRAs
to detect active tuberculosis is similar to that reported in the
literature, and the specificity is slightly lower.
At present, IGRA test is mainly used to assist
diagnosis of MTB infection, and it cannot identify latent MTB
infection and active tuberculosis. As the natural infection rate of
tuberculosis is high in China, nearly 1/3 of people have a history
of MTB infection. In this study, non-active tuberculosis did not
exclude latent MTB infection and old tuberculosis patients.
When the body is in a state of severe
immunosuppression, such as immunodeficiency virus infection,
decompensated liver cirrhosis, severe tuberculosis and non-fully
developed childhood immune system whose T cell response is low,
IGRAs may be false-negative, and the elderly, body mass index
<16.0 kg/m2 may also result in false-negatives
(15). The positive reaction of
interferon-γ release test can also be changed in anti-tuberculosis
treatment. In this study, there were 8 cases of false-negative: 1
case was followed up for more than 2 years after renal
transplantation, with long-term use of anti-rejection drugs; 1 case
of systemic lupus erythematosus active patient, who accepted
repeated hormone shock treatment; 1 case of lumbar spinal
tuberculosis patient who was treated with anti-tuberculosis before
IGRA test; but there are still five false-negative results which
cannot be explained. In the literature, the IGRAs trial has a high
negative predictive value, but negative results are not yet
possible to exclude the possibility of active tuberculosis,
especially in immunosuppressed population (16). Now researchers use pleural effusion,
cerebrospinal fluid as IGRA test specimens, but whether the
negative results are more valuable, is worth exploring.
In summary, IGRA have high sensitivity and good
specificity in the diagnosis of active tuberculosis, but cannot
identify latent MTB infection and old tuberculosis, which is
approved by the US Food and Drug Administration for the diagnosis
of MTB infection rather than active tuberculosis. The results of
this study confirm that IGRAs can be widely used in the diagnosis
of MTB infection in China which has a high natural infection rate
of MTB, and its higher negative predictive value can provide an
important reference for the diagnosis and treatment of clinical
tuberculosis. Moreover, due to the low cost and high quality of the
domestic TB-IGRA, it can be a useful tool in MTB infection
detection in low-income countries with TB endemics.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
LA and PF drafted the manuscript. LA, PF and DC were
mainly devoted to collecting and interpreting the data. LA, SC and
HX revised it critically for important intellectual content. PF, DC
and HX were responsible for the conception and design of the study.
All the authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
The First Affiliated Hospital, Sun Yat-Sen University (Guangzhou,
China). Patients who participated in this research had complete
clinical data. The signed informed consents were obtained from the
patients or the guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
World Health Organization (WHO), . Global
tuberculosis control: Surveillance, financing WHO report 2005.
World Health Organization (WHO/HTM/TB/2005.349) Geneva. https://apps.who.int/iris/bitstream/handle/10665/144569/9241562919_eng.pdf?sequence=1
|
|
2
|
Zhang X, Sun Y, He C, Qiu X, Zhou D, Ye Z,
Long Y, Tang T, Su X and Ma J: The immune characterization of
interferon-β responses in tuberculosis patients. Microbiol Immunol.
62:281–290. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Andersen P, Munk ME, Pollock JM and
Doherty TM: Specific immune-based diagnosis of tuberculosis.
Lancet. 356:1099–1104. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang S, Shao L, Mo L, Chen J, Wang F,
Meng C, Zhong M, Qiu L, Wu M, Weng X, et al: Evaluation of gamma
interferon release assays using Myeobacterium tuberculosis
antigens for diagnosis of latent and active tuberculosis in
Mycobacterium bovis BCG-vaccinated populations. Clin Vaccine
lmmunol. 17:1985–1990. 2010. View Article : Google Scholar
|
|
5
|
Sayyahfar S, Davoodzadeh F, Hoseini R,
Rahimzadeh N and Otukesh H: Comparison of tuberculin skin test and
interferon gamma release assay for diagnosis of latent tuberculosis
infection in pediatric candidates of renal transplantation. Pediatr
Transplant. 22:e131482018. View Article : Google Scholar
|
|
6
|
Ministry of Health of the People's
Republic of China, . Diagnostic criteria for pulmonary
tuberculosis. People's Health Publishing House; Beijing: pp. 1–16.
2008, (In Chinese).
|
|
7
|
Diel R, Loddenkemper R and Nienhaus A:
Evidence-based comparison of commercial interferon-gamma release
assays for detecting active TB: A metaanalysis. Chest. 137:952–968.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Laurenti P, Raponi M, de Waure C, Marino
M, Ricciardi W and Damiani G: Performance of interferon-γ release
assays in the diagnosis of confirmed active tuberculosis in
immunocompetent children: A new systematic review and
meta-analysis. BMC Infect Dis. 16:1312016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Galloway KM and Parker R: Could an
increase in vigilance for spinal tuberculosis at primary health
care level, enable earlier diagnosis at district level in a
tuberculosis endemic country? Afr J Prim Health Care Fam Med.
10:e1–e9. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Thwaites GE: Advances in the diagnosis and
treatment of tuberculous meningitis. Curr Opin Neurol. 26:295–300.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kusum S, Aman S, Pallab R, Kumar SS,
Manish M, Sudesh P, Subhash V and Meera S: Multiplex PCR for rapid
diagnosis of tuberculous meningitis. J Neurol. 258:1781–1787. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Qin L, Zhang L, Zhang Y, Shi X, Zhang Y
and Liu X: Diagnostic value of T-Cell interferon-γ release assays
on cerebrospinal fluid for tuberculous meningitis. PLoS One.
10:01418142015. View Article : Google Scholar
|
|
13
|
Menzies D, Pai M and Comstock G:
Meta-analysis: New tests for the diagnosis of latent tuberculosis
infection: Areas of uncertainty and recommendations for research.
Ann Inter Med. 146:340–354. 2007. View Article : Google Scholar
|
|
14
|
Editorial Board of Chinese Journal of
Tuberculosis and Respiratory Medicine, Chinese Medical Association,
. The application of interferon gamma release test in China. Chin J
Tuberculosis Respir Dis 10. 372014.(In Chinese).
|
|
15
|
Hang NT, Lien LT, Kobayashi N, Shimbo T,
Sakurada S, Thuong PH, Hong LT, Tam DB, Hijikata M, Matsushita I,
et al: Analysis of factors lowering sensitivity of interferon-γ
release assay for tuberculosis. PLoS One. 6:e238062011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Maze M and Beckert L: Active tuberculosis
(TB) with a negative interferon gamma release assay: Failure of
this test to rule out TB. N Z Med J. 126:85–87. 2013.PubMed/NCBI
|