Introduction
Indwelling urethral catheters are a mainstay in the
care of hospitalized patients. An estimated 30 million indwelling
urethral (Foley) catheters are used annually in the United States
(1) and ~20% of hospitalized
patients have a urethral catheter at any given time (2,3).
Catheter-associated lower urinary tract symptoms (CALUTS) refer to
a range of symptoms, including frequency, urgency, burning during
micturition, odynuria and suprapubic pain (3). These symptoms may be caused by
involuntary detrusor contractions induced by activation of
muscarinic type III receptors, also known as M3mAChR,
and the increased release of acetylcholine, which are caused by
reactions of the mucosa in the trigone and urethra after insertion
of a catheter (1-8).
An indwelling catheter enables the continuous drainage of urine,
which maintains an empty bladder, enhances the stimulatory effects
of the catheter on the bladder walls and causes an increased
incidence of CALUTS (6). In
addition, server CALUTS may also be associated with higher the
volume of the balloon and the weight of the catheter and/or urine
bag (9). Previous studies have
reported that CALUTS may aggravate post-operative pain, increase
the occurrence of post-operative complications, including burning
during micturition, odynuria and suprapubic pain or even prolong
the length of hospital stay (7,10,11).
Previous studies in CALUTS prevention have focused on the use of
post-operative medications, including anticholinergic drugs, a
receptor blockers (2-4,12-14).
However, the side effects, such as nausea, vomiting, dizziness and
conscious state changes may have adverse effects on patient
recovery (11).
The present study aimed to compare the effects of
various fixed catheter sites on preventing CALUTS in patients who
underwent surgical removal of upper urinary calculi 24 h after
surgery.
Materials and methods
Study design and subjects
A total of 450 patients who underwent surgical
removal of upper urinary calculi at The Affiliated Hospital of
Southwest Medical University (Luzhou, China) between January 2018
and September 2018 were included in this study. A total of 450
patients were selected in the present study, however, later 4
patients were excluded due to breakage of their catheter balloons.
A final of 446 patients were included in the present study, which
were control group (n=148) and groups A and B (n=149/group). A 16
French double-cava Foley urethral catheter (Bardex) was inserted
into the bladders of each patient following surgery (Fig. 1). Patients >18 years of age with
normal cognitive ability and renal function (serum creatinine
≤44.00 µmol/l, urea nitrogen ≤1.70 mmol/l) met the inclusion
criteria for participation in the present study. Patients who were
diagnosed with benign prostate hyperplasia or urethrostenosis, had
a history of bladder dysfunction (overactive bladder, nocturia
>3, or micturition >8 for 24 h before the surgery (7) neurogenic bladder, bladder
inflammation, incontinence, lower urinary tract infection, urinary
tuberculosis or cognitive disorders were excluded. One hundred and
fifty patients were included in each group. The present study was
approved by the Ethics Committee of the Affiliated Hospital of
Southwest University (Luzhou, China; approval no. K2019002-R).
Informed written consent was obtained from all the patients.
All patients were randomly and evenly divided into 3
groups (control, group A and group B), 150 patients in each group.
The present study was not double blinded as the fixed site for the
catheter on patients was visible. Patients with renal calculi who
underwent percutaneous nephrolithotomy were treated with 100 ml of
0.9% normal saline (NS) + 50 mg of flurbiprofen axetil (Beijing
Forte Meditec Co., Ltd.) in an intravenous drip twice on the day of
surgery and the first day after surgery, while patients with
ureteral calculi were not treated with post-operative analgesics.
Ureteral stents (double J tube; C.R. Bard, Inc.) were retained for
one month in all patients post-operatively.
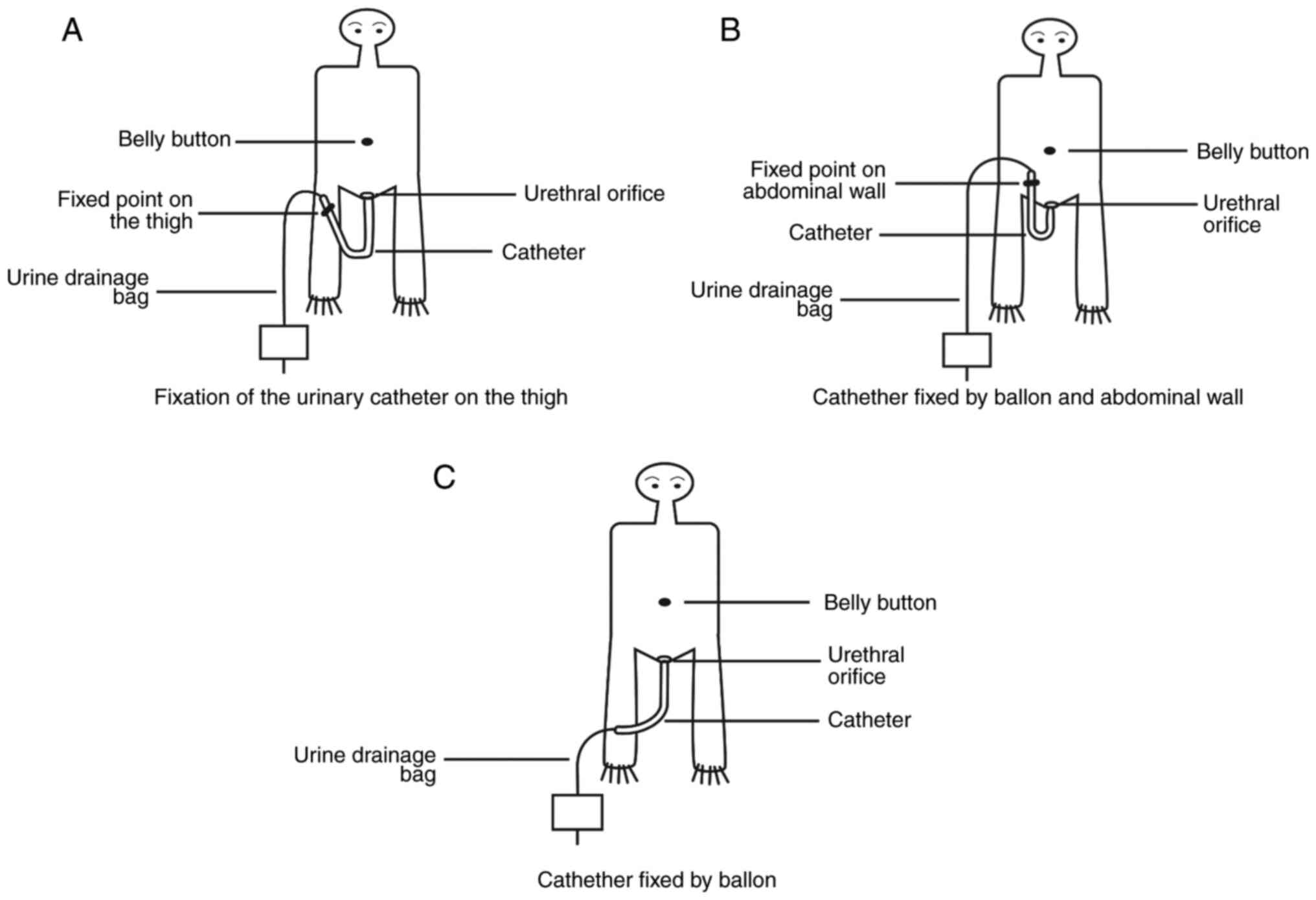
A highly trained nurse was responsible for catheter
fixation and all patients were followed-up for 24 h after catheter
insertion. Catheters were inserted into the bladders of all
patients and the balloons were filled. The catheter was pulled back
after filling the balloon and stopped when the balloon was in
contact with the bladder neck. In group A, the catheters were fixed
on the top one-third of the thigh at the same level as the external
urethral orifice. In doing so the extra-urethral part of the
catheter was U-shaped (Fig. 2A). In
group B, the catheters were fixed to the lower abdominal wall
adjacent to the groin (Fig. 2B).
The patients in whom the catheters were neither fixed on the thigh
nor the abdominal wall were designated as controls (Fig. 2C).
Observation indices were recorded 24 h following
catheter insertion, including the incidence of various CALUTS, such
as frequency, urgency, odynuria, pain in the urethra or bladder, an
increase in urethral discharge, a red and swollen external urethral
orifice and other discomfort associated with the indwelling
catheter or catheter obstruction.
Pain in the urethra and bladder were evaluated
according to a previous study as follows: 0, no pain; 1-3, mild
pain; 4-6, moderate pain; and 7-10, severe pain (15). The catheter-associated level of
discomfort was quantified as follows: 0, no discomfort; 1, mild
discomfort; 2, moderate discomfort, but able to tolerate the
indwelling catheter; and 3, severe discomfort requiring removal of
the catheter (6).
Statistical analysis
The data were analyzed using the SPSS 18.0 (SPSS,
Inc.). The normality of data distribution of the continuous
variables was assessed using the Shapiro-Wilk test. Continuous
variables with normal distribution are presented as the mean ±
standard deviation (SD). The means of normally distributed
continuous variables were compared using Tukey's test and one-way
ANOVA (Respectively, if the results of ANOVA was significant,
Tukey's test was used to compare the differences between the two
means.). Tukey's test was used to compare between groups. P<0.05
was considered to indicate a statistically significant
difference.
Results
Basic characteristics
No significant differences were observed in indices,
such as age, sex, education level, types of surgery, including
percutaneous nephroscopy (PCNL) and ureteroscopy (URL) and the
length of the operation between the control group and groups A and
B (P>0.05; Table I).
 | Table IParameters of patients (n=446) with
different catheter fixation sites who underwent surgical removal of
upper urinary calculi. |
Table I
Parameters of patients (n=446) with
different catheter fixation sites who underwent surgical removal of
upper urinary calculi.
| | Sex, n (%) | Education level, n
(%) | Type of surgery, n
(%) |
|---|
| Patients | Age, years X±S | Length of the
operation, min X±S | Male | Female | Illiterate | Primary | Junior | High | University | PCNL | URL |
|---|
| Control (n=148) | 54.14±18.97 | 45.53±17.89 | 91 (61.49) | 57 (38.51) | 20 (13.51) | 53 (35.81) | 45 (30.41) | 20 (13.51) | 10 (6.76) | 64 (43.24) | 84 (56.76) |
| Group A (n=149) | 54.27±18.54 | 45.79±17.58 | 95 (63.76) | 54 (36.24) | 21 (14.09) | 50 (33.56) | 47 (31.54) | 22 (14.77) | 9 (6.04) | 67 (44.97) | 82 (55.03) |
| Group B (n=149) | 53.99±19.12 | 46.01±17.64 | 93 (62.42) | 56 (37.58) | 20 (13.42) | 51 (34.23) | 48 (32.21) | 23 (15.44) | 7 (4.70) | 65 (43.62) | 84 (56.38) |
| χ2
valuea | 0.06 | 0.13 | 0.164 | | 0.3 | | | | | 0.085 | |
| P-valuea | >0.05 | >0.05 | 0.686 | | 0.99d | | | | | 0.765e | |
| χ2
valueb | t=0.07 | 0.23 | 0.027 | | 0.871 | | | | | 0.004 | |
| P-valueb | >0.05 | >0.05 | 0.869 | | 0.929d | | | | | 0.947e | |
| χ2
valuec | t=0.13 | 0.11 | 0.058 | | 0.317 | | | | | 0.054 | |
| P-valuec | >0.05 | >0.05 | 0.810 | | 0.989d | | | | | 0.816e | |
Comparison of urinary catheter related
LUTS
Patients in group A had significantly lower
incidences of frequency, urgency and odynuria compared with
patients in the control group (P<0.05). The proportion of
patients who complained of bladder pain in groups A or B was
significantly lower compared with patients in the control group
(P<0.05) (Table II), while the
number of patients with mild bladder pain in group A was
significantly higher compared with group B (P<0.05) (Table II). The incidence of dysuria and
total urethral pain scores of group A was significantly lower than
group B (P<0.05). In addition, patients in group B had a
significantly lower incidence of urgency when compared with the
control group (P<0.05) (Table
II). Significantly lower incidences of urethral discharge and
catheter traction were observed in patients in group A compared
with patients in the group B (P<0.05; Table III). In group B, a significantly
higher incidence of urethral discharge was observed compared with
group A and the control group, and a significantly higher incidence
of red and swollen external urethral orifices in group B compared
with group A was observed (P<0.05; Table III). The incidence of urethrorrhea
in the control group was significantly higher than group A and B
(10 vs. 1 and 4, respectively), while there were only two cases
with catheter blockage in group A.
| Table IIComparison of catheter-associated
lower urinary tract symptoms between the 3 groups of patients. |
Table II
Comparison of catheter-associated
lower urinary tract symptoms between the 3 groups of patients.
| | Urethral pain scores
(15) n (%) | Bladder pain scores n
(%) |
|---|
| Patients | Frequency n (%) | Urgency | Odynuria | 1-3 | 4-6 | 7-10 | Total | 1-3 | 4-6 | 7-10 | Total |
|---|
| Control (n=148) | 86 (58.11) | 36 (24.32) | 18 (12.16) | 54 (36.49) | 3 (2.03) | 2 (1.35) | 59 (39.87) | 23 (15.54) | 7 (4.73) | 7 (4.73) | 37 (25.00) |
| Group A
(n=149) | 68 (45.64) | 16 (10.74) | 13 (8.72) | 33 (22.15) | 0 | 2 (1.34) | 35 (23.49) | 23 (15.44) | 1 (0.67) | 0 (0.00) | 24 (16.11) |
| Group B
(n=149) | 73 (48.99) | 18 (12.08) | 26 (17.45) | 55 (36.91) | 2 (1.34) | 2 (1.34) | 59 (39.59) | 20 (13.42) | 0 (0.00) | 5 (3.36) | 5 (3.36) |
| χ2
valuea | 4.635 | 9.489 | 0.938 | 3.082 | | | 9.203 | 11.974 | | | 3.598 |
|
P-valuea | 0.032 | 0.002 | 0.333 | 0.214e | | | 0.002 | 0.003d | | | 0.058 |
| χ2
valueb | 2.480 | 7.482 | 1.645 | 0.211 | | | 0.002 | 7.911 | | | 3.038 |
|
P-valueb | 0.115 | 0.006 | 0.200 | 0.900e | | | 0.962 | 0.019d | | | 0.081 |
| χ2
valuec | 0.337 | 0.133 | 4.986 | 2.135 | | | 8.951 | 4.073 | | | 0.024 |
|
P-valuec | 0.562 | 0.716 | 0.026 | 0.344e | | | 0.003 | 0.044d | | | 0.876 |
| Table IIIComparison of other
catheter-associated lower urinary tract symptoms between the 3
groups of patients. |
Table III
Comparison of other
catheter-associated lower urinary tract symptoms between the 3
groups of patients.
| Patients | Urethral discharge
n (%) | Urethrorrhea n
(%) | Catheter traction,
n (%) | Red and swollen
urethra, n (%) | Catheter blockage n
(%) |
|---|
| Control
(n=148) | 77 (52.03) | 10 (6.76) | 71 (47.97) | 12 (8.11) | 0 (0.00) |
| Group A
(n=149) | 94 (63.09) | 1 (0.67) | 14 (9.40) | 7 (4.70) | 2 (1.34) |
| Group B
(n=149) | 111 (74.50) | 4 (2.68) | 13 (8.72) | 20 (13.42) | 0 (0.00) |
| χ
valuea | 3.718 | 7.710 | 54.089 | 1.442 | 0.497 |
|
P-valuea | 0.054 | 0.005 | 0.000 | 0.230 | 0.481 |
| χ2
valueb | 16.137 | 2.741 | 56.388 | 2.182 | - |
|
P-valueb | 0.000 | 0.098 | 0.000 | 0.140 | - |
| χ2
valuec | 4.517 | 0.814 | 0.041 | 6.883 | 0.503 |
|
P-valuec | 0.034 | 0.367 | 0.840 | 0.009 | 0.478 |
Comparison of catheter associated
discomfort
There were 51 cases with mild of catheter-associated
discomfort in control group, while it was 40 and 41 cases in group
A and group B, respectively. The total cases with catheter
associated discomfort was 63 in control group, while it was 42 and
46 in group A and group B, respectively. Patients in groups A and B
had a lower incidence of mild discomfort when compared with the
control group (Table IV).
| Table IVComparison of catheter associated
discomfort between the 3 groups of patients (6). |
Table IV
Comparison of catheter associated
discomfort between the 3 groups of patients (6).
| Patients | Level 1 (mild) n
(%) | Level 2 (moderate)
n (%) | Level 3 (severe) n
(%) | Total n (%) |
|---|
| Control
(n=148) | 51 (34.46) | 8 (5.41) | 4 (2.70) | 63 (42.57) |
| Group A
(n=149) | 40 (26.85) | 0 (0.00) | 2 (1.34) | 42 (28.19) |
| Group B
(n=149) | 41 (27.52) | 0 (0.00) | 5 (3.36) | 46 (30.88) |
Discussion
In the present study the effects of various fixed
sites of catheters on preventing CALUTS in patients who underwent
surgical removal of upper urinary calculi were assessed, and it was
demonstrated that catheters fixed by filling the balloon then
fixing the catheter to the top one-third of the thigh were most
beneficial for patients.
In the present study, patients in group A complained
of significantly less frequency and urgency, odynuria and bladder
pain compared with the control group, which may be due to the
additional fixed site of the catheter. The additional fixed site on
the thigh changed the pressure of the catheter and urine bag weight
on the additional fixed position. Hence, this fixation site could
decrease the pull force of the catheter and urine bag on the neck
of the bladder and urethra. In the control group, the pull force of
the catheter and urine bag may directly press on the neck of the
bladder and urethra, especially when the patients were in bed. The
aforementioned reason may explain the complaints of majority of the
patients in the control group who reported more serious CALUTS when
in bed, and may also be responsible for the significantly higher
incidence of frequency, urgency and odynuria in the control group
compared with group A and B.
In the present study, patients in group B also had
an additional fixed site of the catheter on the abdominal wall;
however, they had a significantly lower incidence of frequency and
a significantly decreased composition ratio of bladder pain when
compared with the control group (P<0.05). Patients in group B
had a significantly increased incidence of odynuria, urethral pain
and proportion of severe bladder pain compared with group A
(P<0.05). The findings of the present study were consistent with
those of Zhang and Zhang (16) who
reported that the additional fixation of the catheter on the inside
of the thigh may lower the incidence of external urethral orifice
pain, ulcers and necrosis in patients with neurosurgical crises.
The present study hypothesized that the difference of CALUTS
between groups A and B in the present study may be due to the
different fixed position of urethral catheter resulting in
different changes in normal physiological structure of the urethra.
Although, in the present study the additional fixation of the
catheter on the abdominal wall decreased the pull forces from the
catheter and urine bag on the urethra, the additional fixation site
was still at a higher level compared with the external urethral
orifice, which caused a reverse angle to be formed between the
extra-urethral part of the catheter and the urethra (the size of
the angle depends on the fat thickness beneath the abdominal wall).
This reverse angle causes the catheter to pull and press on the
urethra and therefore increases the incidence rate of odynuria. In
addition, the additional fixation on the abdominal wall affects the
physio anatomy of the urethra and causes the disappearance of the
urethral ante curvature (6,17). The urethral ante curvature was
therefore passive straightened in the present study which increased
the urethral pain. In group A, the additional fixation of the
catheter on the thigh enabled the catheter and external urethral
orifice to be at the same level which thereby maintaining the
physiological curve of the urethra, decreased the press force of
the catheter on the urethra and decreased the incidence of
odynuria.
In the present study, patients in groups A and B
were observed to have a significantly lower incidence of catheter
traction compared with the control group (P<0.05); however, no
significant difference in the incidence of catheter traction or
blockage was observed between groups A and B (P>0.05). The
findings of the present study were not consistent with those of
Zheng and Li (18), which
considered that catheter traction was more likely to occur in the
thigh fixation than in the abdominal wall fixation. The present
study hypothesized that the different additional fixation sites and
methodology utilized may be responsible for this inconsistency. In
the present study, in patients from group A the pull force of the
catheter and urine bag on the urethra and bladder neck could be
released when the patients abducted their thigh, bend their knees
and rolled over in bed. Patients in groups A or B demonstrated no
significant difference in incidence of a red and swollen external
urethral orifice compared with the control group (P>0.05), while
a significantly lower incidence was found in group A when compared
with group B (P<0.05). The aforementioned findings were
consistent with the results obtained by Zhang and Zhang (16). The present study hypothesized that
the additional fixation on the abdominal wall may increase the pull
force of the catheter on the urethra, form the reverse angle and
cause the passive straight urethral antecurvature. In addition, the
significant increase in urethral discharge in group B compared with
group A and the control group may also be responsible for the
difference observed between the groups (P<0.05).
In the present study, the incidence of
catheter-associated discomfort and the proportion of severe
catheter-associated discomfort in groups A and B was significantly
lower compared with the control group. In groups A and B, the
majority of patients complained of mild catheter-associated
discomfort, while in the control group, the majority of patients
complained of moderate and severe discomfort. The different
incidence rates of pull force by the catheter may be responsible
for this finding. The pull force from the catheter may have a
crucial effect on CALUTS; however, in the present study the
incidence of odynuria, urethral and bladder pain in group A was
significantly lower compared with group B, while no significant
difference was observed in the incidence of catheter-associated
discomfort and the proportion of severe catheter-associated
discomfort between groups A and B. The present study hypothesized
that catheter-associated discomfort may involve the incidence of
CALUTS and the pull force of the catheter, and might also depend on
the tolerance of the patient. This may explain inconsistent results
between the present study and those of Sun and Wang (19) who compared the different comfort
levels between various catheter fixation sites and concluded that
there was no significant difference of the comfort of female
patients between the abdominal wall fixation and thigh
fixation.
The present study had some limitations. First,
whether fixation of the catheter could be applied to urological
surgery of the lower urinary tract was not evaluated. Further
studies with clinical efficacy were needed. Secondly, the
observation time was only 24 h. With the extension of catheter
indwelling time, whether different fixation methods have different
effects on the occurrence of CALUTS and other accompanying symptoms
needs further observation and confirmation.
The present study demonstrated that additional
fixation of the catheter for bedridden patients was necessary and
decreased the incidence of CALUTS and other concomitant symptoms,
such as catheter traction and urethral discharge. An additional
fixation site on the thigh is recommended based on the results of
the present study.
Acknowledgements
Not applicable.
Funding
The present study was funded by a grant from the
Health Department of Sichuan Province for the Research of
Continuing Nursing Health Promoting Education Model for Patients
with Urinary Stones (grant no. 16158).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
The authors declare that all the listed authors have
participated actively in the study and all met the requirements of
the authorship. LZ and RJ conducted study design and experimental
supervision. LZ wrote the first draft of the manuscript, RJ edited
the manuscript and reviewed it, XW conducted secondary fixation and
data collection of urinary catheters in all patients, LP and QD
were responsible for intraoperative catheter indwelling and airbag
fixation, XK and XL were responsible for statistical analysis of
data. All authors read and approved the publication of the
manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
The Affiliated Hospital of Southwest University (Luzhou, China;
approval no. K2019002-R). Informed written consent was obtained
from each patient.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Binhas M, Motamed C, Hawajri N, Yiou R and
Marty J: Predictors of catheter-related bladder discomfort in the
post-anaesthesia care unit. Ann Fr Anesth Reanim. 30:122–125.
2011.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Agarwal A, Dhiraaj S, Singhal V, Kapoor R
and Tandon M: Comparison of efficacy of oxybutynin and tolterodine
for prevention of catheter related bladder discomfort: A
prospective, randomized, placebo-controlled, double-blind study.
Brit J Anaesth. 96:377–380. 2006.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ryu JH, Hwang JW, Lee JW, Seo JH, Park HP,
Oh AY, Jeon YT and Do SH: Efficacy of butylscopolamine for the
treatment of catheter-related bladder discomfort: A prospective,
randomized, placebo-controlled, double-blind study. Brit J Anaesth.
111:932–937. 2013.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Shi H, Zhang H, Pan W, Lu Y, Zhang Y, Chen
L, Wei C and Cui Y: Pooled analysis of the efficacy and safety of
intraoperative dexmedetomidine on postoperative catheter-related
bladder discomfort. Low Urin Tract Symptoms: Jun 4, 2020 (Epub
ahead of print). doi: 10.1111/luts.12322.
|
|
5
|
Kim HC, Lee YH, Jeon YT, Hwang JW, Lim YJ,
Park JE and Park HP: The effect of intraoperative dexmedetomidine
on postoperative catheter-related bladder discomfort in patients
undergoing transurethral bladder tumor resection: A double-blind
randomised study. Eur J Anaesthesiol. 32:596–601. 2015.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Wilson M: Causes and management of
dwelling urinary catheter-related pain. Br J Nurs. 17:232–239.
2008.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Anderson KE and Wein AJ: Pharmacology of
the lower urinary tract:basis for current and future treatments of
urinary incontinence. Pharmacol Rev. 56:581–631. 2004.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Li JY and Ren Liao R: Prevention of
catheter-related bladder discomfort-pudendal nerve block with
ropivacaine versus intrsvenous tramadol: Study protoccl for a
randomized controlled trial. Trials. 17(448)2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Hanchett M: Techniques for stabilizing
urinary catheters. Am J Nurs. 102:44–48. 2002.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Bai Y, Wang X, Li X, Pu C, Yuan H, Tang Y,
Li J, Wei Q and Han P: Management of catheter-related bladder
discomfort in patients who underwent elective surgery. J Endourol.
29:640–649. 2015.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Lepousé C, Lautner CA, Liu L, Gomis P and
Leon A: Emergence delirium in adults in the post-anaesthesia care
unit. Br J Anaesth. 96:747–753. 2006.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Srivastava VK, Agrawal S, Kadiyala VN,
Ahmed M, Sharma S and Kumar R: The efficacy of pregabalin for
prevention of catheter-related bladder discomfort: A prospective,
randomiazed, placebo-controlled double-blind study. J Anesth.
29:212–216. 2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Maro S, Zarattin D, Baron T, Bourez S, de
la Taille A and Salomon L: Catheter-related bladder discomfort
after urologicalsurgery: Importance of the type of surgery and
efficiency of treatment by clonazepam. Prog Urol. 24:628–633.
2014.PubMed/NCBI View Article : Google Scholar : (In French).
|
|
14
|
Shariat Moharari R, Lajevardi M, Khajavi
M, Najafi A, Shariat Moharari G and Etezadi F: Effects of
intra-operative ketamine administration on postoperative
catheter-related bladder discomfort: A double-blind clinical trial.
Pain Pract. 14:146–150. 2014.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Breivik H, Borchgrevink PC, Allen SM,
Rosseland LA, Romundstad L, Hals EK, Kvarstein G and Stubhaug A:
Assessment of pain. Br J Anaesth. 101:17–24. 2008.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Zhang J and Zhang X: Effect of external
urinary catheterization on indwelling catheterization in critically
ill patients with neurosurgery. Nurs Res. 19:1577–1578. 2005.
|
|
17
|
Na YQ and Guo ZH: Practical urology. First
Edition. Beijing: People's Medical Publishing House, 2009.
|
|
18
|
Zheng LI and Li D: Comparison of the
effects of different methods of fixation of indwelling catheters in
elderly patients. Gen Nurs. 10:1570–1571. 2012.
|
|
19
|
Sun Y and Wang X: Improvement and effect
of female indwelling catheter fixation method. Nurs Res.
22(624)2008.
|