Introduction
Primary biliary cirrhosis (PBC) is a chronic
liver-specific autoimmune disorder with an unidentified etiology.
It mainly affects middle-aged women (male-to-female rario, 1:9) and
is categorized by the infiltration of lymphocytes in portal tracts,
the destruction of small- and medium-sized intrahepatic bile ducts,
and the progressive scarring that initially leads to fibrosis and,
eventually, to cirrhosis and end-stage hepatic failure over a
period of 10–20 years without treatment (1,2).
Previous data have indicated that PBC, particularly asymptomatic
PBC, is no longer considered a rare disease due to diagnostic
improvements that include biochemical tests, histological analyses
and the detection of autoantibodies in serum (3,4).
Although histopathological changes serve as the ‘gold standard’ for
the diagnosis of PBC, a liver biopsy is an invasive, painful and
costly procedure that is associated with the possibility of
sampling error and variability in interpretation. To date,
biomarkers for the diagnosis of PBC, such as anti-mitochondrial
antibody (AMA) have been evaluated. AMA, which reacts with the
pyruvate dehydrogenase E2 subunit, is commonly accepted as a
serological hallmark for the diagnosis of PBC, since AMA appears in
approximately 90% of patients with PBC (5). However, depending on the assay used,
up to 15% of patients with PBC have been found to be AMA-negative
(5). Furthermore, although some
AMA-negative patients are positive for antinuclear antibody (ANA)
components in PBC, unlike AMA, which is used for diagnosis,
PBC-associated ANA correlates with the disease severity and may
thus serve as a marker for poor prognosis instead of diagnosis
(5). Besides, although the
nuclear components, including Sp100, promyelocytic leukemia
proteins and two components of the nuclear pore complex protein
(gp210 and nucleoporin 62), react with ANA, as has been previously
demonstrated, anti-sp100 antibody is not a better prognostic marker
for Chinese patients with PBC compared to anti-gp210 antibody,
which was only detected in 34.3% of Chinese patients with PBC
(6).
Therefore, it is still necessary to discover other
novel biomarkers for PBC. Metabolomics is the study of a large
number of low molecular weight metabolites, including amino acids,
hormones and sugars, and has arisen as a potent tool for
discovering novel biomarkers for Parkinson’s disease (7), prostate cancer (8), type 2 diabetes (9), acute myocardial infarction (10) and preeclampsia (11). Metabolomics has also provided some
important insight into the pathogenesis of human non-alcoholic
fatty liver disease, non-alcoholic steatohepatitis and PBC
(12–16). In this study, we utilized a
metabonomics technique based on ultraperformance liquid
chromatography coupled with quadrupole-time-of-flight mass
spectrometry (UPLC/Q-TOF MS) in an aim to discover novel markers
for PBC and elucidate their pathological roles in the progression
of PBC.
Subjects and methods
Patients
A total of 32 patients with a clinical and/or
histological diagnosis of PBC at the Second Affiliated Hospital of
Kunming Medical University, Kunming, China between May 2010 and
November 2011 were enrolled in this study. The experimental
protocol was established, according to the ethical guidelines of
the Helsinki Declaration and was approved by the Human Ethics
Committee of the Affiliated Hospital of Kunming Medical University.
Written informed consent was obtained from each participant prior
to enrollment. The diagnosis of PBC was based on the following
criteria, as previously described (17): i) increased levels of biochemical
markers reflecting intrahepatic cholestasis for >6 months; ii)
an normal biliary system, as shown by ultrasound or
cholangiography; iii) patients were serum AMA- or AMA-M2 positive;
iv) patients were serum AMA/AMA-M2-negative, but a liver biopsy
revealed moderate or severe periportal or periseptal inflammation.
The appropriate exclusion criteria included other liver diseases,
such as alcoholic liver disease, viral hepatitis, drug-induced
liver diseases, genetic diseases, cancer, pregnancy, lactating
subjects, as well as subjects whose blood or urine specimen samples
were kept at room temperature for >30 min. All 32 healthy
control subjects (HCs) were confirmed to have normal liver function
and fit the same exclusion criteria as the patients with PBC.
Informed consent was obtained from all subjects. The study protocol
conformed to the ethical guidelines of the 2008 Declaration of
Helsinki and was approved by the research ethics committee of our
institution.
Sample collection and metabolomics
analysis
In all subjects, blood (3 ml) was drawn after a 12-h
fast, serum was obtained by centrifugation of the blood samples at
3,000 rpm at 4°C for 10 min, and urina sanguinis samples (2 ml)
were collected on the same day as the blood samples. All the
samples were stored at −80°C until subsequent analyses. The urine
samples were thawed at room temperature and centrifuged at 10,000 ×
g at 4°C for 20 min. Subsequently, 150 µl of the supernatant
were diluted with purified water to 1 ml and filtered through a
0.22-µl filter. A total of 10 µl of sample was then
taken. The blood samples were thawed at room temperature, and 180
µl of the sample were then added to acetonitrile (720 µl)
followed by vigorous shaking for 30 sec and centrifugation at
15,000 × g at 4°C for 10 min. The supernatant was stored at 4°C for
analysis within 48 h.
Chromatography
Chromatographic separation was performed on a 15
cmx2.1 mm Acquity™ 1.8 µm C18 column (Agilent Technologies,
Santa Clara, CA, USA) using an Acquity™ ultra performance liquid
chromatography system (Ultimate 3000-Bruker mXis; Dionex,
Sunnyvale, CA, USA). A 10-µl aliquot of each sample was
injected into the column. The column was maintained at 4°C and
eluted with 0.1% formic acid (A) and acetonitrile (B) in a linear
gradient (0–60 min, 5–100% of B). The follow rate was at 0.3
ml/min.
Mass spectrometry
Mass spectrometry was performed on a Waters Q-TOF
micro Mass Spectrometer (Waters MS Technologies, Manchester, UK) in
both the ESI+ and ESI− ion modes. The
following parameters were used: nebulization gas, 6 l/min at 200°C;
cone, 50 l/h; source gas temperature, 100°C; capillary voltage,
4,500 V; cone voltage, 35 V; Q-TOF micro MS acquisition rate, 0.5
sec with a 0.1 sec interscan delay. The scan range was from 50 to
1,000 m/z. Data were collected in centroid mode. All analyses were
acquired using the lock spray to ensure accuracy and
reproducibility; sodium formate was used as the lock mass at a
concentration of 1 mmol/l and a flow rate of 10 µl/min,
deriving an [M + H]+ ion at 4,500 V in ESI+
mode, and an [M - H]− ion at 3,200 V in ESI−
mode. The lock spray frequency was set at 20 sec. Sodium formate
was used as an internal control in this assay.
Data analysis
The raw data were analyzed using ProfileAnalysis
software (Ultimate 3000-Bruker mXis; Dionex) the retention time
(tr) and m/z data pair for each peak were detected using
software from Umetrics AB (Umeå, Sweden). The ion intensities for
each peak detected were then normalized within each sample to the
sum of the peak intensities in that sample, as previously described
(18). The resulting normalized
peak intensities were then multiplied by 10,000. The data were then
exported and analyzed by principal components analysis (PCA) and
partial least squares-discriminate analysis (PLS-DA) using SIMCA-P
software (Umetrics AB). The statistical analysis was performed
using SPSS version 10.0 software (SPSS, Inc., Chicago, IL, USA). A
P-value <0.05 was considered to indicate a statistically
significant difference.
Results
Characteristics of the patients
The characteristics of 32 PBC patients and the 32
HCs were analyzed. Due to hemolysis, one blood sample from each
group was excluded for further assessment. The mean ages of the
patients with PBC and the HCs were 52.6±11.95 years (range, 30–76
years) and 52.1±14.6 years (range, 27–76 years), and the
female-male ratios were 27/5 and 25/7, respectively. There were no
significant differences between the patients with PBC and the HCs
in terms of age, parity and gender (P>0.05). Sixteen cases from
the PBC group were newly diagnosed with PBC, and the mean time
course of the disease was 25.4±45.3 months (range, 4 days to 17
years). The liver function Child-Pugh score was grade A in 23
cases, grade B in 8 cases and grade C in 1 case. The globulin and
transaminase levels are presented Table I. The detection levels of
autoantibodies in the sera from patients with PBC are shown in
Fig. 1. In total, 15 patients
were AMA-M2-positive, 8 were anti-gp210-positive, 7 were
anti-sp100-positive, 10 were AMA-M2-, anti-gp210- and
anti-sp100-negative, 1 was AMA-M2-, anti-gp210- and
anti-sp100-positive, 7 were AMA-M2- and anti-gp210-positive, 1 was
anti-gp210- and anti-sp100-positive, and 2 were AMA-M2- and
anti-sp100-positive.
 | Table IClinical data of globulin and
transaminase levels in the patients with PBC. |
Table I
Clinical data of globulin and
transaminase levels in the patients with PBC.
| Liver function | No. | Min. value | Max. value | Mean ± SD |
|---|
| ALT (U/l) | 32 | 15 | 1176 | 156±225.4 |
| AST (U/l) | 32 | 30 | 710 | 145.2±148.46 |
| ALP (U/l) | 32 | 61 | 893 | 299±203.2 |
| GGT (U/l) | 32 | 29 | 1359 | 346.8±280.67 |
| GLO (g/l) | 32 | 23.6 | 53.5 | 34.9±6.56 |
Urine and serum profiles in patients with
PBC
Following UPLC/Q-TOF analysis, the retention time
and m/z data pair for each peak were detected. Although PCA is an
excellent tool for data reduction and hence graphical display, it
does not lend itself to the development of a diagnostic model to
predict the presence or absence of disease. To address this issue,
PLS-DA and the coefficient of correlation analysis were used for
marker selection and identification, as previously described
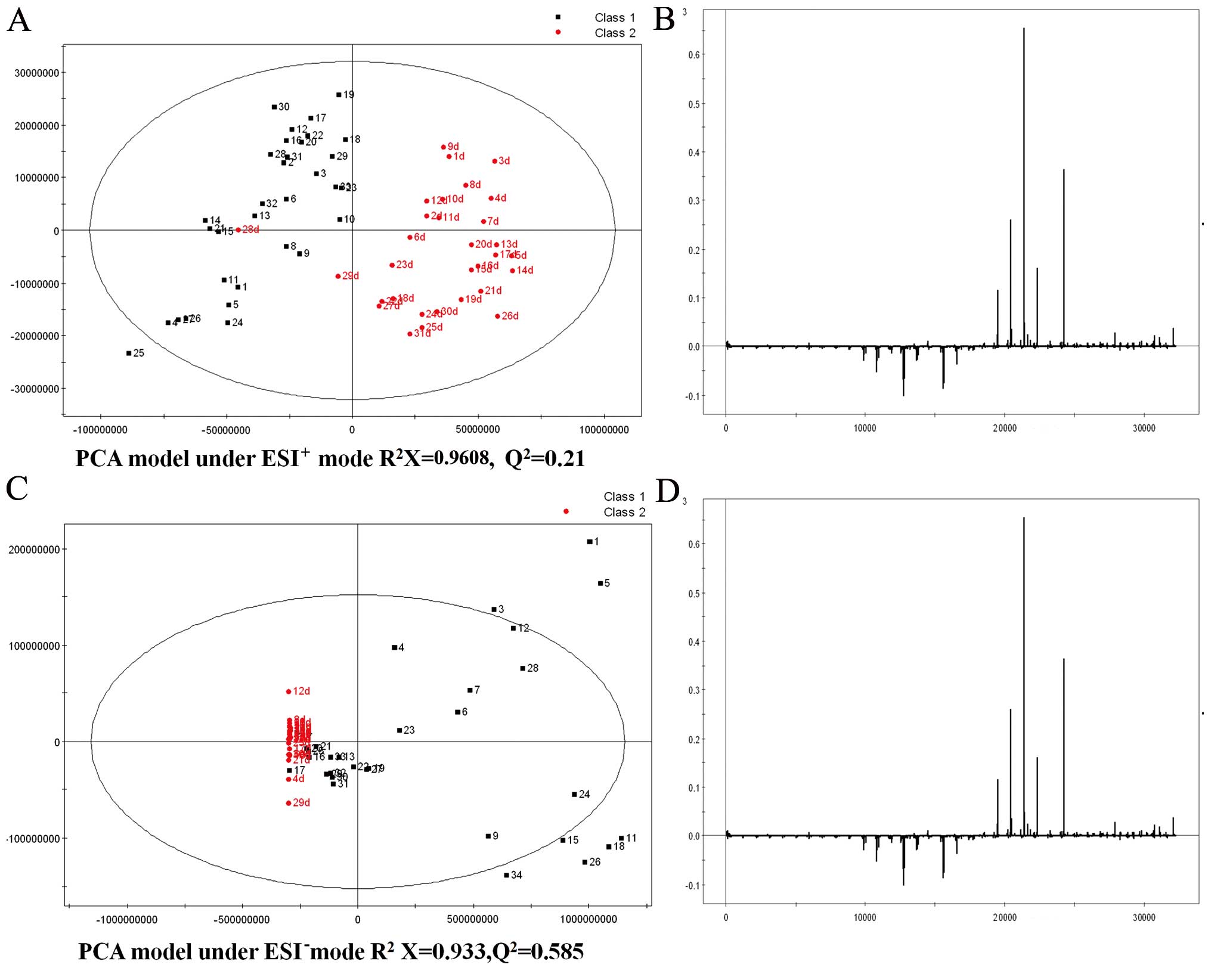
(19). Figs. 2Figure 3–4 show the score plots of PCA and PLS-DA
of the urine metabolome from the patients with PBC and the HCs
scanned by ESI+ and ESI−. The prediction rate
and resolution are very good under the urine ESI mode to
distinguish the PBC group from the control group using the PLS-DA
model. Since patients with PBC were shown to be distributed in
different regions, we divided them into 2 subgroups.
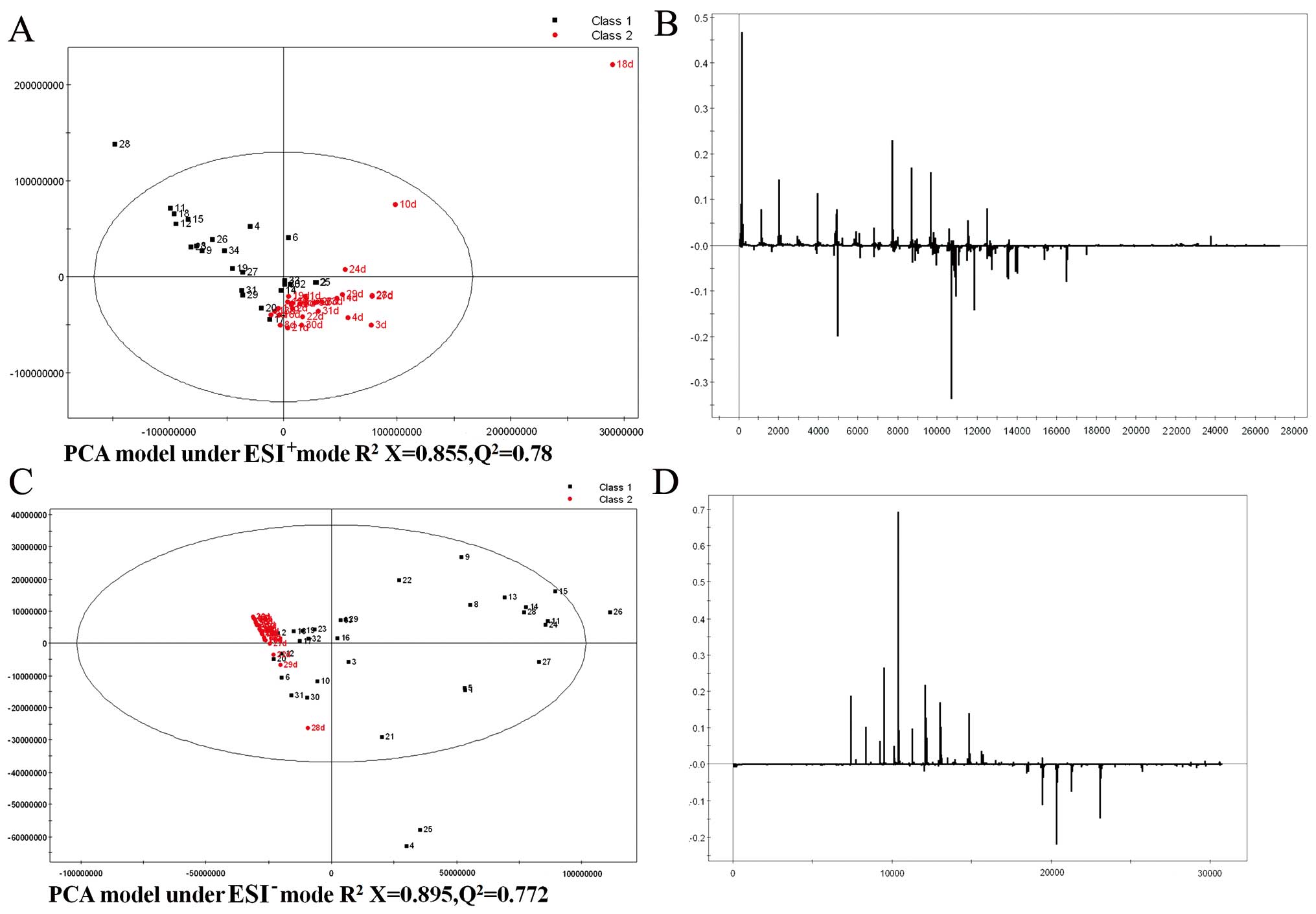
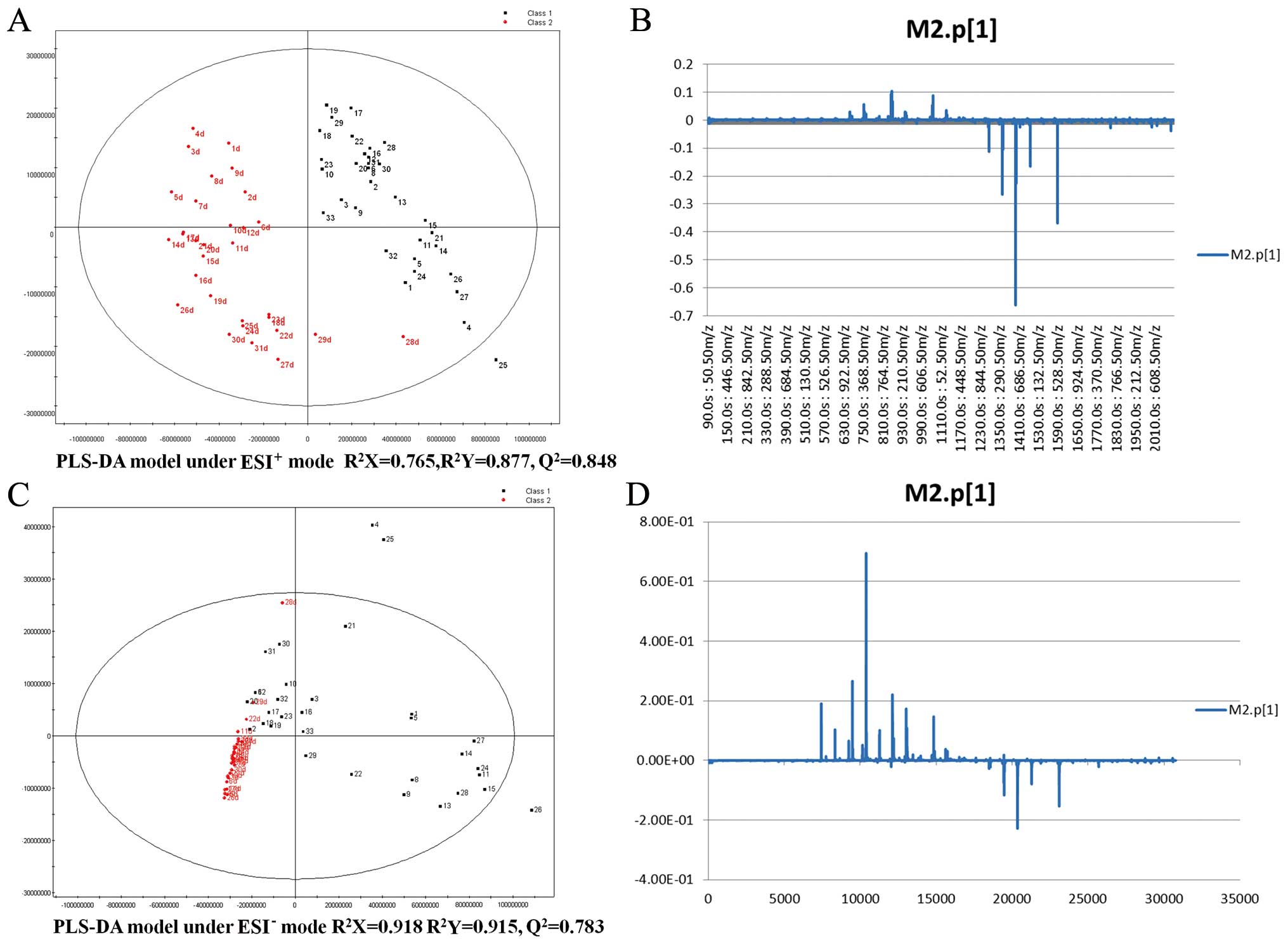
Figs. 5 and
6 show the score plots of PCA and
PLS-DA of the serum metabolome from patients with PBC and the HCs
scanned by ESI+ and ESI−. In both ion
scanning modes, the modeling parameters listed in Table II indicate that the models of PBC
had been successfully established and the patients with PBC could
be easily distinguished through these models. Potential biomarkers
were identified in the urine (Table
III) and serum (Table IV)
from PBC patients. The levels of 11 of the 18 potential biomarkers
identified were increased in the urine of the patients with PBC,
while the levels of 7 of these 18 potential biomarkers were
decreased in the urine of the patients with PBC compared to the
HCs. Similarly, the levels of 9 of the 20 potential biomarkers
identified in the serum of the patients with PBC were increased,
while the levels of 11 of these 20 potential biomarkers were
decreased in the serum of the patients with PBC compared to the
HCs. Among these biomarkers, the levels of bile acids increased
with the progression of PBC, while the levels of carnitines, such
as propionyl carnitine and butyryl carnitine, decreased with the
progression of PBC.
| Table IISummary of the modeling information
for PCA and PLS-DA analysis. |
Table II
Summary of the modeling information
for PCA and PLS-DA analysis.
| Sample mode | Analysis mode | R2X | R2Y | Q2 |
|---|
| Urine
ESI+ | PCA-X | 0.608 | | 0.21 |
| Urine
ESI+ | PLS-DA | 0.328 | 0.755 | 0.679 |
| Urine
ESI− | PCA-X | 0.933 | | 0.585 |
| Urine
ESI−a | PLS-DA | 0.944 | 0.9 | 0.682 |
| Urine ESI-subgroup
1 | PLS-DA | 0.648 | 0.865 | 0.711 |
| Urine ESI-subgroup
2 | PLS-DA | 0.953 | 0.985 | 0.964 |
| Serum
ESI+ | PCA-X | 0.855 | | 0.78 |
| Serum
ESI+ | PLS-DA | 0.765 | 0.877 | 0.848 |
| Serum
ESI− | PCA-X | 0.895 | | 0.772 |
| Serum
ESI− | PLS-DA | 0.918 | 0.915 | 0.783 |
| Table IIISelected markers indicating a
difference between ESI+ and ESI− scans of the
urine samples from patients with PBC and HCs. |
Table III
Selected markers indicating a
difference between ESI+ and ESI− scans of the
urine samples from patients with PBC and HCs.
| No | Tr±30 (sec) | Patients with PBC
vs. HCs | m/z | Potential
markers |
|---|
|
ESI+ | | | | |
| 1 | 390 | ↑ | 321.1362 | Three oxygen
radicals on cinnamic acid |
| 2 | 750 | ↑ | 414.2997 | Glycolic amide |
| 3 | 810 | ↑ | 626.3537 | aSugar goes to oxygen cholic acid
3-glucoside, bile acid, glucuronic acid |
| 4 | 930 | ↑ | 432.3118 |
7a-hydroxy-3-ursodeoxycholic acid
oxo-5b |
| 5 | 930 | ↑ | 823.4127 | UK |
| 6 | 1110 | ↑ | 593.3328 | Urobilinogen |
| 7 | 90 | ↓ | 204.9095 | Potassium chlorate,
cyano sulfate anion |
| 8 | 150 | ↓ | 218.1390 | Propionyl
carnitine |
| 9 | 210 | ↓ | 232.1548 | Butyryl
L-carnitine, butyryl carnitine |
| 10 | 330 | ↓ | 268.1060 | Deoxyguanosine,
adenosine |
| 11 | 390 | ↓ | 189.0657 | Hippuric acid,
3-succinyl pyridine, adrenaline, hydroxybenzoic acid,
hydroxybenzoic acid |
| 12 | 570 | ↓ | 286.2012 | UK |
| 13 | 630/690 | ↓ | 310.2013 | L-group of ammonia
and alcohol, L-carnitine zinn |
|
ESI− | | | | |
| 14 | 630 | ↑ | 288.6198 | aCow bile acid sodium sulfonated goes
to oxygen-7-sulfuric acid |
| 15 | 810 | ↑ | 624.3392 | aGlycine goes to deoxycholic acid
3-glucoside acid |
| 16 | 870 | ↑ | 471.2423 | aUrsodesoxycholic acid,
chenodeoxycholic acid 3-sulfuric acid, bile acid sulfate goes to
oxygen |
| 17 | 930 | ↑ | 448.3072 | aAmmonia bearing bile acid goes to
oxygen, chenodeoxycholic acid glycine conjugated, DNA single
glycine conjugate |
| 18 | 750 | ↑ | 528.2645 | aGlycine goes to deoxycholic
acid-3-sulfuric acid, aGlycine
lithocholic acid 3-sulfuric acid disodium salt |
| Table IVSelected markers indicating a
difference between the ESI+ and ESI− scans of
the serum samples from patients with PBC and the HCs. |
Table IV
Selected markers indicating a
difference between the ESI+ and ESI− scans of
the serum samples from patients with PBC and the HCs.
| No. | Tr±30 (sec) | Patients with PBC
vs. HCs | m/z | Potential
markers |
|---|
|
ESI+ | | | | |
| 1 | 670/750 | ↑ | 414.3005 | UK |
| 2 |
870/930/1110/1050 | ↑ | 450.3213 | aCDCA, glycine conjugated, deoxycholic
acid f glycine conjugated |
| 3 | 1050 | ↑ | 466.316 | aGCA |
| 4 | 1290/1350 | ↓ | 520.394 | Salbutamol |
| 5 | 1350/1410 | ↓ | 496.3394 | 3-β,α-hydroxy-5–7
bile acid ethyl ester, carnitine 3.24 X-hydroxy-3-alcohol |
| 6 | 1470 | ↓ | 522.3556 | UK |
| 7 | 1590 | ↓ | 524.2707 | UK |
| 8 | 2070 | ↓ | 758.5705 | UK |
|
ESI− | | | | |
| 9 | 570/630/690 | ↑ | 288.62 | aCattle sulfonated goes to oxygen
cholic acid-7-sulfuric acid |
| 10 | 690/750 | ↑ | 528.2632 | aGlycine goes to deoxych olic
acid-3-sulfuric acid, aGlycine
lithocholic acid 3-sulfuric acid disodium salt |
| 11 | 810 | ↑ | 498.2891 | aCDCA, tauroursodeoxycholic acid,
tauroursodesoxycholic acid |
| 12 | 810 | ↑ | 514.2843 | aTaurocholic acid |
| 13 | 1050 | ↑ | 437.206 | aCDCA deoxycholic acid |
| 14 | 1110 | ↑ | 448.3074 | aChenodeoxycholic acid glycine
conjugated, glycine conjugated deoxycholic acid |
| 15 | 1290 | ↓ | 476.2773 | UK |
| 16 | 1350/1410 | ↓ | 540.3302 | UK |
| 17 | 1350 | ↓ | 564.3304 | UK |
| 18 | 1470 | ↓ | 566.3485 | UK |
| 19 | 1590 | ↓ | 568.3623 | UK |
| 20 | 1770 | ↓ | 433.236 |
5,6-Dihydroxy-prostaglandin F1A |
Small molecule metabolites may be distinguished
effectively using PCA and PLS-DA in the ESI+ and
ESI− mode. This method is a good prediction method,
apart from PCA-X of the urine ESI+ mode
(R2X=0.608, Q2=0.21). All the identified
metabolites of the potential biomarkers are listed in Tables III and IV.
Discussion
Significant hurdles to the early diagnosis of PBC
still exist. Due to the shortcomings of liver biopsies and the
limitations of AMA and ANA antibody assays, a cost-effective early
detection method will require a very accurate screening method.
Therefore, clinically helpful biomarkers for the early detection of
PBC should be measurable in an easily accessible bodily fluid, such
as blood or urine. Furthermore, these biomarkers should provide
predictive value with high specificity and sensitivity. In the
present study, we compared the metabolomics profiles of urine and
serum from patients with PBC with those of age- and gender-matched
HCs using both unsupervised PCA and supervised PLS-DA with
UPLC/Q-TOF.
In this study, the analysis of the urine and serum
metabolomics profiles identified important differences between the
patients with PBC and the HCs. One of the most significant
observations was that the levels of bile acids were significantly
increased in the patients with PBC compared to the HCs. In line
with our results, in a previous study, the concentrations of total
bile acids, taurine and glycine conjugates of primary bile acids
were increased in patients with PBC, compared to non-cholestatic
donors (16). Indeed, bile acids
are the main product of endogenous cholesterol metabolism and are
related to lipid absorption and biliary excretion. Bile acids
endure a strong enterohepatic recirculation, through which they can
be converted into secondary deoxycholic and lithocholic acids in
the intestines. Bile acids reabsorbed in the intestines may be
further absorbed back into the liver, as only a small fraction of
bile acids is found in the peripheral circulating blood and urine
in healthy individuals. However, liver injury caused by liver
diseases, such as cirrhosis and gallbladder disease, results in a
decrease in the hepatic clearance of bile acids and, eventually, in
an increase in the levels of bile acids in the serum. Therefore,
bile acids are considered to be a hallmark of liver injury. During
the early stages of liver cirrhosis, bile acids may induce the
upregulation of hepatocyte-derived monocyte chemotaxis protein-1
(MCP-1), a hepatic stellate cell-responsive chemokine, leading to
hepatic stellate cell recruitment. In turn, MCP-1 mediates hepatic
stellate cell recruitment, causing a further decrease in the
hepatic clearance of bile acids and further promoting liver
cirrhosis (20). Furthermore,
bile acids directly activate the proinflammatory signaling network
in hepatocytes and induce the upregulation of multiple
proinflammatory mediators, such as cytokines, chemokines, adhesion
molecules and other proteins that influence immune cell functions
(21). Moreover, bile acid
receptor GP-BAR1 (TGR5) expression has been shown to be increased
in rodent models of colitis and Crohn’s disease (22); and the treatment of a murine model
of non-alcoholic fatty liver disease with a dual bile acid FXR/TGR5
receptor agonist was shown to decrease intrahepatic inflammation
and altered the immune phenotype of monocytes (23).
The bile acid sensor farnesoid X receptor (FXR) is
required for the immunoregulatory activities of Toll-like
receptor-9 in intestinal inflammation (24). Another intriguing difference
between patients with PBC and HCs is the relatively higher level of
carnitines, such as propionyl carnitine and butyryl carnitine in
HCs. Carnitine is a substance necessary for long-chain fatty acids
to pass the mitochondrial intramembrane to induce β-oxidation
(25). However, the results of
studies assessing carnitine metabolism in patients with PBC have
been controversial thus far. Some studies have demonstrated that
the lack of carnitine decreases the rate of hepatic fatty acid
oxidation and may be associated with hepatic steatosis, which
causes pathological consequences in the liver (26), whereas elevated carnitine
concentrations are present in patients with cirrhosis of different
causes (27). In addition, an
increased urinary excretion of total carnitine has been found due
to an increase in the fractional excretion of both free carnitine
and short-chain acylcarnitine (28). Furthermore, severe carnitine
deficiency leads to the increased apoptosis of enterocytes, villous
atrophy, inflammation and gut injury (29); and L-carnitine supplementation has
been shown to have a positive effect in improving immune responses
in aged animals (30).
The third potential biomarker for PBC is the
relatively higher level of prostaglandin (PG), which is an
important player in inflammatory processes. In fact,
phytohemagglutinin (PHA)-stimulated-enriched monocytes of patients
with PBC produce approximately 3-fold more PGE2 than
that of normal control monocytes (31); and the PGE2 produced in
monocytes may play a primary role in the hyporesponsiveness to PHA
observed in patients with PBC (32). Moreover, epithelial cells from
patients with PBC have been shown to have moderate levels of
cyclooxygenase-2 expression, which in turn participates in the
conversion of arachidonic acid into PG (33). PGs also function in the transition
and maintenance of chronic inflammation. One role that PGs play in
such processes is the amplification of cytokine signaling, which in
turn facilitates acquired immunity and induces long-lasting immune
inflammation (34). PGs also play
a part in chronic inflammation by generating a positive feedback
loop and/or inducing chemokines and recruiting inflammatory cells
to alternate active cell populations in affected tissues (35). In addition, PGs contribute to
tissue remodeling in fibrosis in a transforming growth factor
β-independent manner (36). Thus,
PGs are commonly known as mediators of inflammation (37–39).
The fourth difference between the patients with PBC
and the HCs was the elevated level of urine deoxyguanosine, which
is known as an oxidatively damaged nucleobase of DNA excreted into
the urine. Indeed, the possible association of oxidative stress has
been suggested to be involved in the pathogenesis of cellular
senescence in PBC (40). For
example, oxidative stress and proinflammatory cytokines, such as
interferon-β and tumor necrosis factor-α, induce reactive oxygen
species generation and activate the ATM/p53/p21WAF1/Cip1 pathway,
followed by biliary epithelial senescence in the case of PBC
(41).
In conclusion, the findings of the present study
suggest that the circulating levels of bile acids and carnitine are
differentially altered in patients with PBC. However, due to the
limitations of the present pilot study, such as a small patient
population and the absence of a stratification metabolomics profile
amongst the disease stages of PBC, further studies to confirm the
differential variations are warranted.
Acknowledgments
This study was supported by the National Natural
Science Foundation of China (grant no. 81360072), the Natural
Science Foundation of Yunnan Province (grant go. 2013FB050) and the
Health Science and Technology Project of Yunnan Province (grant
nos. 2012WS0102, 2012WS0103 and 2014NS109). The authors would like
to thank Ms. Wen Na Guan (Qingdao Institute of Biological Energy
and Process Research Institute of the Chinese Academy of Sciences)
for assisting in the detection and data analysis of
UPLC-Q-TOF-MS.
References
|
1
|
Kaplan MM and Gershwin ME: Primary biliary
cirrhosis. N Engl J Med. 353:1261–1273. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Prince M, Chetwynd A, Newman W, Metcalf JV
and James OF: Survival and symptom progression in a geographically
based cohort of patients with primary biliary cirrhosis: Follow-up
for up to 28 years. Gastroenterology. 123:1044–1051. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kim WR, Lindor KD, Locke GR III, Therneau
TM, Homburger HA, Batts KP, Yawn BP, Petz JL, Melton LJ III and
Dickson ER: Epidemiology and natural history of primary biliary
cirrhosis in a US community. Gastroenterology. 119:1631–1636. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Selmi C, Invernizzi P, Zuin M, Podda M and
Gershwin ME: Genetics and geoepidemiology of primary biliary
cirrhosis: Following the footprints to disease etiology. Semin
Liver Dis. 25:265–280. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
He XS, Ansari AA, Ridgway WM, Coppel RL
and Gershwin ME: New insights to the immunopathology and autoimmune
responses in primary biliary cirrhosis. Cell Immunol. 239:1–13.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hu C, Deng C, Song G, Zhang W, Zhang S, Li
X, Li P, Zhang F and Li Y: Prevalence of autoimmune liver disease
related autoantibodies in Chinese patients with primary biliary
cirrhosis. Dig Dis Sci. 56:3357–3363. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bogdanov M, Matson WR, Wang L, Matson T,
Saunders-Pullman R, Bressman SS and Flint Beal M: Metabolomic
profiling to develop blood biomarkers for Parkinson’s disease.
Brain. 131:389–396. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sreekumar A, Poisson LM, Rajendiran TM, et
al: Metabolomic profiles delineate potential role for sarcosine in
prostate cancer progression. Nature. 457:910–914. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wang C, Kong H, Guan Y, Yang J, Gu J, Yang
S and Xu G: Plasma phospholipid metabolic profiling and biomarkers
of type 2 diabetes mellitus based on high-performance liquid
chromatography/electrospray mass spectrometry and multivariate
statistical analysis. Anal Chem. 77:4108–4116. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sabatine MS, Liu E, Morrow DA, Heller E,
McCarroll R, Wiegand R, Berriz GF, Roth FP and Gerszten RE:
Metabolomic identification of novel biomarkers of myocardial
ischemia. Circulation. 112:3868–3875. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Heazell AE, Brown M, Worton SA and Dunn
WB: Review: The effects of oxygen on normal and preeclamptic
placental tissue -insights from metabolomics. Placenta. 32(Suppl
2): S119–S124. 2011. View Article : Google Scholar
|
|
12
|
Barr J, Caballería J, Martínez-Arranz I,
et al: Obesity-dependent metabolic signatures associated with
nonalcoholic fatty liver disease progression. J Proteome Res.
11:2521–2532. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kalhan SC, Guo L, Edmison J, Dasarathy S,
McCullough AJ, Hanson RW and Milburn M: Plasma metabolomic profile
in nonalcoholic fatty liver disease. Metabolism. 60:404–413. 2011.
View Article : Google Scholar
|
|
14
|
Puri P, Wiest MM, Cheung O, et al: The
plasma lipidomic signature of nonalcoholic steatohepatitis.
Hepatology. 50:1827–1838. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tokushige K, Hashimoto E, Kodama K, et al:
Serum metabolomic profile and potential biomarkers for severity of
fibrosis in nonalcoholic fatty liver disease. J Gastroenterol.
48:1392–1400. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Trottier J, Białek A, Caron P, Straka RJ,
Heathcote J, Milkiewicz P and Barbier O: Metabolomic profiling of
17 bile acids in serum from patients with primary biliary cirrhosis
and primary sclerosing cholangitis: A pilot study. Dig Liver Dis.
44:303–310. 2012. View Article : Google Scholar
|
|
17
|
Heathcote EJ: Management of primary
biliary cirrhosis. The American Association for the Study of Liver
Diseases practice guidelines. Hepatology. 31:1005–1013. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yin P, Zhao X, Li Q, Wang J, Li J and Xu
G: Metabonomics study of intestinal fistulas based on
ultraperformance liquid chromatography coupled with Q-TOF mass
spectrometry (UPLC/Q-TOF MS). J Proteome Res. 5:2135–2143. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
User’s Guide to SIMCA-P, SIMCA-P version
11.0. Umetrics AB; Umeå, Sweden: pp. 3972005
|
|
20
|
Ramm GA, Shepherd RW, Hoskins AC, et al:
Fibrogenesis in pediatric cholestatic liver disease: Role of
taurocholate and hepatocyte-derived monocyte chemotaxis protein-1
in hepatic stellate cell recruitment. Hepatology. 49:533–544. 2009.
View Article : Google Scholar
|
|
21
|
Allen K, Jaeschke H and Copple BL: Bile
acids induce inflammatory genes in hepatocytes: A novel mechanism
of inflammation during obstructive cholestasis. Am J Pathol.
178:175–186. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Cipriani S, Mencarelli A, Chini MG,
Distrutti E, Renga B, Bifulco G, Baldelli F, Donini A and Fiorucci
S: The bile acid receptor GPBAR-1 (TGR5) modulates integrity of
intestinal barrier and immune response to experimental colitis.
PLoS One. 6:e256372011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
McMahan RH, Wang XX, Cheng LL, et al: Bile
acid receptor activation modulates hepatic monocyte activity and
improves nonalcoholic fatty liver disease. J Biol Chem.
288:11761–11770. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Renga B, Mencarelli A, Cipriani S, D’Amore
C, Carino A, Bruno A, Francisci D, Zampella A, Distrutti E and
Fiorucci S: The bile acid sensor FXR is required for
immune-regulatory activities of TLR-9 in intestinal inflammation.
PLoS One. 8:e544722013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bremer J: Carnitine - metabolism and
functions. Physiol Rev. 63:1420–1480. 1983.PubMed/NCBI
|
|
26
|
Bowyer BA, Miles JM, Haymond MW and
Fleming CR: L-carnitine therapy in home parenteral nutrition
patients with abnormal liver tests and low plasma carnitine
concentrations. Gastroenterology. 94:434–438. 1988.PubMed/NCBI
|
|
27
|
Amodio P, Angeli P, Merkel C, Menon F and
Gatta A: Plasma carnitine levels in liver cirrhosis: Relationship
with nutritional status and liver damage. J Clin Chem Clin Biochem.
28:619–626. 1990.PubMed/NCBI
|
|
28
|
Krähenbühl S and Reichen J: Carnitine
metabolism in patients with chronic liver disease. Hepatology.
25:148–153. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sonne S, Shekhawat PS, Matern D, Ganapathy
V and Ignatowicz L: Carnitine deficiency in OCTN2−/−
newborn mice leads to a severe gut and immune phenotype with
widespread atrophy, apoptosis and a proinflammatory response. PLoS
One. 7:e477292012. View Article : Google Scholar
|
|
30
|
Thangasamy T, Subathra M, Sittadjody S,
Jeyakumar P, Joyee AG, Mendoza E and Chinnakkanu P: Role of
L-carnitine in the modulation of immune response in aged rats. Clin
Chim Acta. 389:19–24. 2008. View Article : Google Scholar
|
|
31
|
Chiricolo M, Lenzi M, Bianchi F,
Franceschi C, Bartolini G, Orlandi M, Tomasi V and Licastro F:
Immune dysfunction in primary biliary cirrhosis. II. Increased
production of prostaglandin E. Scand J Immunol. 30:363–367. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Licastro F, Lenzi M, Chiricolo M, Davis
LJ, Cassani F, Bianchi F and Franceschi C: Immune dysfunction in
primary biliary cirrhosis (PBC): I. Increased sensitivity of PHA
stimulated lymphocyte cultures to indomethacin. J Clin Lab Immunol.
23:19–23. 1987.PubMed/NCBI
|
|
33
|
Hayashi N, Yamamoto H, Hiraoka N, et al:
Differential expression of cyclooxygenase-2 (COX-2) in human bile
duct epithelial cells and bile duct neoplasm. Hepatology.
34:638–650. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Yao C, Sakata D, Esaki Y, Li Y, Matsuoka
T, Kuroiwa K, Sugimoto Y and Narumiya S: Prostaglandin E2-EP4
signaling promotes immune inflammation through Th1 cell
differentiation and Th17 cell expansion. Nat Med. 15:633–640. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Aoki T, Nishimura M, Matsuoka T, et al:
PGE(2)-EP(2) signalling in endothelium is activated by haemodynamic
stress and induces cerebral aneurysm through an amplifying loop via
NF-κB. Br J Pharmacol. 163:1237–1249. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Oga T, Matsuoka T, Yao C, et al:
Prostaglandin F(2alpha) receptor signaling facilitates
bleomycin-induced pulmonary fibrosis independently of transforming
growth factor-beta. Nat Med. 15:1426–1430. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ricciotti E and FitzGerald GA:
Prostaglandins and inflammation. Arterioscler Thromb Vasc Biol.
31:986–1000. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Fattahi MJ and Mirshafiey A:
Prostaglandins and rheumatoid arthritis. Arthritis (Egypt).
2012:2393102012.
|
|
39
|
Lima IV, Bastos LF, Limborço-Filho M,
Fiebich BL and de Oliveira AC: Role of prostaglandins in
neuroinflammatory and neurodegenerative diseases. Mediators
Inflamm. 2012:9468132012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Bell LN, Wulff J, Comerford M, Vuppalanchi
R and Chalasani N: Serum metabolic signatures of primary biliary
cirrhosis and primary sclerosing cholangitis. Liver Int.
35:263–274. 2015. View Article : Google Scholar
|
|
41
|
Sasaki M, Ikeda H, Sato Y and Nakanuma Y:
Proinflammatory cytokine-induced cellular senescence of biliary
epithelial cells is mediated via oxidative stress and activation of
ATM pathway: A culture study. Free Radic Res. 42:625–632. 2008.
View Article : Google Scholar : PubMed/NCBI
|