Introduction
Tacrolimus, a potent immunosuppressive agent, was
developed in the 1990s and can be isolated from the bacteria
Streptomyces tsukubaensis. FK-506-binding protein 12
(FKBP-12) is an important immunophilin targeted by tacrolimus in T
cells, and tacrolimus can form a complex with FKBP-12, thus
repressing the phosphatase calcineurin, an enzyme necessary to
activate the nuclear factor of T cells (NF-AT) (1-4).
NF-AT serves a key role in the transcription of cytokine-encoding
genes in T cells (5).
Tacrolimus has primarily been used for treating
patients who have received allogeneic organ transplants or patients
with autoimmune diseases (4,6-11).
However, clinical management of tacrolimus therapy can be
challenging due to its narrow treatment range and significant
variabilities within and among individuals (12,13), and these limitations can be caused
by multiple factors that interfere with its metabolism. Therefore,
in clinical settings, therapeutic drug monitoring is used to
optimize the treatment regimen (14).
Tacrolimus has various side effects, and
nephrotoxicity is the most common, occurring in ~50% of patients
treated with tacrolimus (15).
Renal fibrosis is commonly associated with nephrotoxicity (16-20). Fibrosis plays a crucial role in
cadmium-induced nephrotoxicity (16), cyclosporine nephrotoxicity
(17,19), nephrotoxicity induced by oral
sodium nitrite (18) and
aristolochic acid nephrotoxicity (20). In addition, renal fibrosis is an
important process underlying tacrolimus nephrotoxicity (21,22). Therefore, it is important to
identify the factors that lead to renal fibrosis following
tacrolimus nephrotoxicity and control its development (21,22). The present study aimed to
investigate the mechanism underlying renal fibrosis induced by
tacrolimus and to identify novel potential targets.
Materials and methods
Animal experiments
In total, 16 specific pathogen free male Wistar rats
(age, 3 weeks; weight, 64±3 g) were purchased from Shanghai SLAC
Laboratory Animal Co., Ltd. The animals were housed in standard
cages and maintained under standard conditions at a constant room
temperature of 20-25°C, a humidity of 40-70% and a 12/12 h
light/dark cycle. All rats had free access to regular chow and
water. The rats were randomly divided into a normal control (NC)
group (n=8) and a tacrolimus nephrotoxicity (NE) group (n=8). The
NE group was intraperito neally injected with tacrolimus (Astellas
Ireland Co., Ltd.) at 2 mg/kg per day (23,24). The NC group received daily
intraperito neal administrations of equal volumes of tacrolimus
solvent, which consisted of polyoxyethylene hydrogenated castor oil
and absolute ethyl alcohol, for 2 weeks. Animal protocols and
procedures were approved by The Animal Care and Use Committee of
Children's Hospital of Fudan University (Shanghai, China) and
complied with the appropriate institutional regulations.
Sample collection
After 2 weeks of intervention, Wistar rats were
anesthetized with 10% chloral hydrate (300 mg/kg) by
intraperitoneal injection. Animals did not present obvious signs of
peritonitis in the present study. Blood samples were collected from
the abdominal aorta. The rats were euthanized by cervical
dislocation under deep anesthesia with 10% chloral hydrate. The
death of rats was verified by the heartbeat, breathing and neural
reflex. After Wistar rats were sacrificed, the kidneys were removed
and weighed. The kidney index was calculated using the following
formula: Kidney index = (average kidney weight/body weight)
(25). Paraformaldehyde (4%) was
used to fix the fresh kidneys, and liquid nitrogen was used to
rapidly freeze the residual kidney tissues, which were stored at
-80°C until further analysis.
Observation of kidney histological
Kidney tissues were fixed in 4% paraformaldehyde at
4°C for 24 h, embedded in paraffin and cut into 4-µm-thick
sections (26). The sections were
then stained by Masson staining, Sirius red staining and periodic
acid-silver methenamine (PASM) staining (all from Wuhan Servicebio
Technology Co., Ltd.). Masson staining was performed at room
temperature (25°C), with iron hematoxylin for 3 min, Ponceau S
solution for 5 min, phosphomolybdic acid for 1 min and aniline blue
for 3 min. Masson staining was used to dye the collagen fibers
blue. Sirius red staining was performed at room temperature (25°C)
for 1 h. Following Sirius red staining, the collagen fibers were
stained red. For PASM staining, the sections were stained with
periodic acid for 15 min at room temperature (25°C) and hexamine
silver working solution for 40 min at 58°C. Following PASM
staining, elastic and mesh fibers were stained in black. The
aforementioned staining was observed using a light microscope
(Nikon Eclipse E100) at a magnification of ×400. The sum of
integral optical density (IOD) was used to quantify the results and
calculated using Image-Pro Plus 6.0 software (Media Cybernetics,
Inc.).
Immunohistochemistry assays
The 4-µm-thick sections were baked at 60°C
for 2 h and then deparaffinized in xylene, rehydrated in 100, 85
and 75% alcohol, and then washed in water. Subsequently, antigen
retrieval was performed. The samples were treated with 3% hydrogen
peroxide to block endogenous peroxidase activity and then blocked
with BSA for 30 min at room temperature (25°C). Sections were
incubated with vimentin antibody (1:500; Wuhan Servicebio
Technology Co., Ltd.; cat. no. GB11192) at 4°C overnight.
Subsequently, the appropriate secondary antibodies (1:200; HRP-goat
anti-rabbit IgG; Wuhan Servicebio Technology Co., Ltd.; cat. no.
GB23303) were incubated with the sections in the dark at room
temperature (25°C) for 50 min. Subsequently, 3,3'-diami-nobenzidine
dye solution (Dako; Agilent Technologies, Inc.) was incubated with
the sections at room temperature in the dark. Sections were
observed and images were acquired using a light microscope
(magnification, ×400). The sum of IOD was used to quantify the
results and calculated using Image-Pro Plus 6.0 software (Media
Cybernetics, Inc.). The color of vimentin staining was
claybank.
Immunofluorescence method
The 4-µm-thick sections were baked at 60°C
for 2 h and then deparaffinized in xylene, rehydrated in 100, 85
and 75% alcohol, and then washed in water. Subsequently, antigen
retrieval was performed. Then, to reduce the spontaneous
auto-fluorescence, tissue auto-fluorescence quencher (Wuhan
Servicebio Technology Co., Ltd.; cat. no. G1221) was added for 5
min and samples were rinsed in water for 10 min. Sections were
blocked using BSA for 30 min at room temperature (25°C). Samples
were incubated with anti-E-cadherin (1:5,000; Wuhan Servicebio
Technology Co., Ltd.; cat. no. GB12082) and anti-α-smooth muscle
actin (α-SMA) antibodies (1:10,000; Wuhan Servicebio Technology
Co., Ltd.; cat. no. GB13044) at 4°C overnight. Following incubation
with the primary antibodies, the sections were washed and incubated
with the corresponding secondary antibodies (1:500; HRP-goat
anti-mouse IgG; Wuhan Servicebio Technology Co., Ltd.; cat. no.
GB23301) in the dark at room temperature (25°C) for 50 min. DAPI
solution (Wuhan Servicebio Technology Co., Ltd.) was then added and
the samples were incubated in the dark at room temperature for 10
min. An anti-fluorescence quenching solution was used to seal the
samples. Samples were observed and images were acquired using a
confocal microscope (Nikon Corporation; magnification, ×400). The
sum of IOD was used to quantify the results and calculated using
Image-Pro Plus 6.0 software (Media Cybernetics, Inc.). E-cadherin
was stained in red and α-SMA was stained in green.
RNA library construction and
sequencing
Suzhou Basepair Biotechnology Company (http://www.basepair.cn/) performed the RNA library
construction and sequencing in biological triplicates using an
Illumina HiSeq X Ten Sequencing system (Illumina, Inc.). The main
sequencing processes included sequencing data quality
preprocessing, reference genome alignment, gene expression analysis
and differential expression analysis (25,27).
Kyoto Encyclopedia of Genes and Genomes
(KEGG) pathway enrichment
Sequencing data were analyzed as raw reads, and were
saved in a FASTQ format document. To obtain clean reads,
adaptor-contaminated and low-quality sequences were removed using
filtering methods, as previously described (28). FastQC (version 0.11.4; http://www.bioinformatics.babraham.ac.uk/projects/fastqc/)
was used to examine the quality of the clean reads (25). Subsequently, the reads were
aligned to the reference genome Ensemble-Rnor6.0 using Hisat2
(version 2.1.0). Gene coverage was analyzed using the percentage of
genes covered by the reads. Functional annotation was performed
using ANNOVAR (29).
Differentially expressed genes (DEGs) were identified using the
DEGseq panormalage method (30),
according to negative binomial distributions. The gene expression
levels were analyzed according to the number of fragments per
kilobase of transcript per million reads and counts values. Genes
with an adjusted |log2(fold change)| >1 and P<0.05
were considered as DEGs. KEGG pathway analysis was performed for
the DEGs using the KEGG Orthology-Based Annotation System (31). The significantly enriched KEGG
pathways exhibited a P<0.05 (25,27,28,32).
Statistical analysis
Data are presented as the mean ± standard error of
the mean. The statistical analysis was performed using SPSS
(version 13.0; SPSS, Inc. and GraphPad Prism (version 5.0; GraphPad
Software Inc.). Each experiment was performed three times. An
unpaired Student's t-test was used to compare the protein
expression level between the two groups. P<0.05 was considered
to indicate a statistically significant difference.
Results
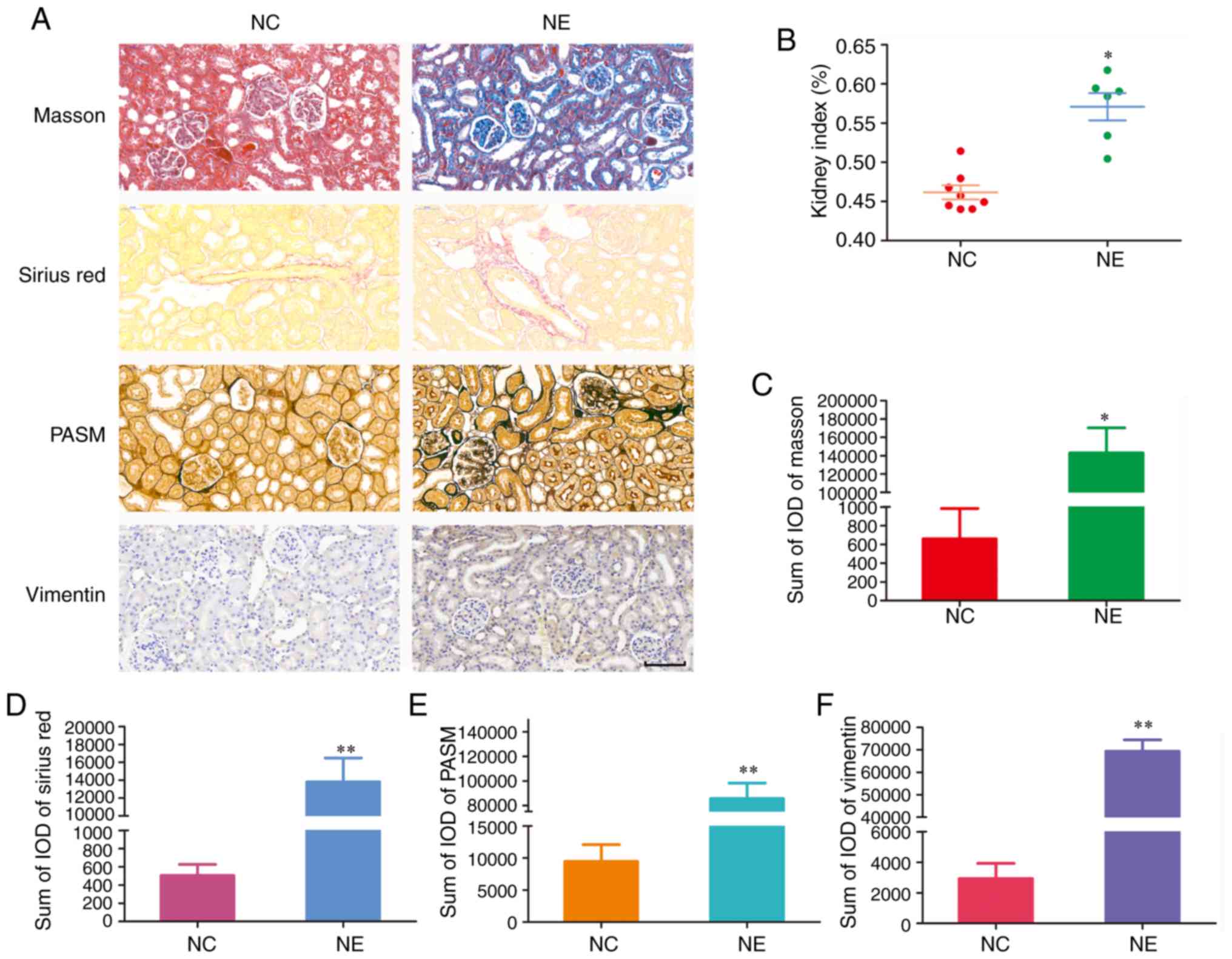
Pathological changes in kidneys induced
by tacrolimus
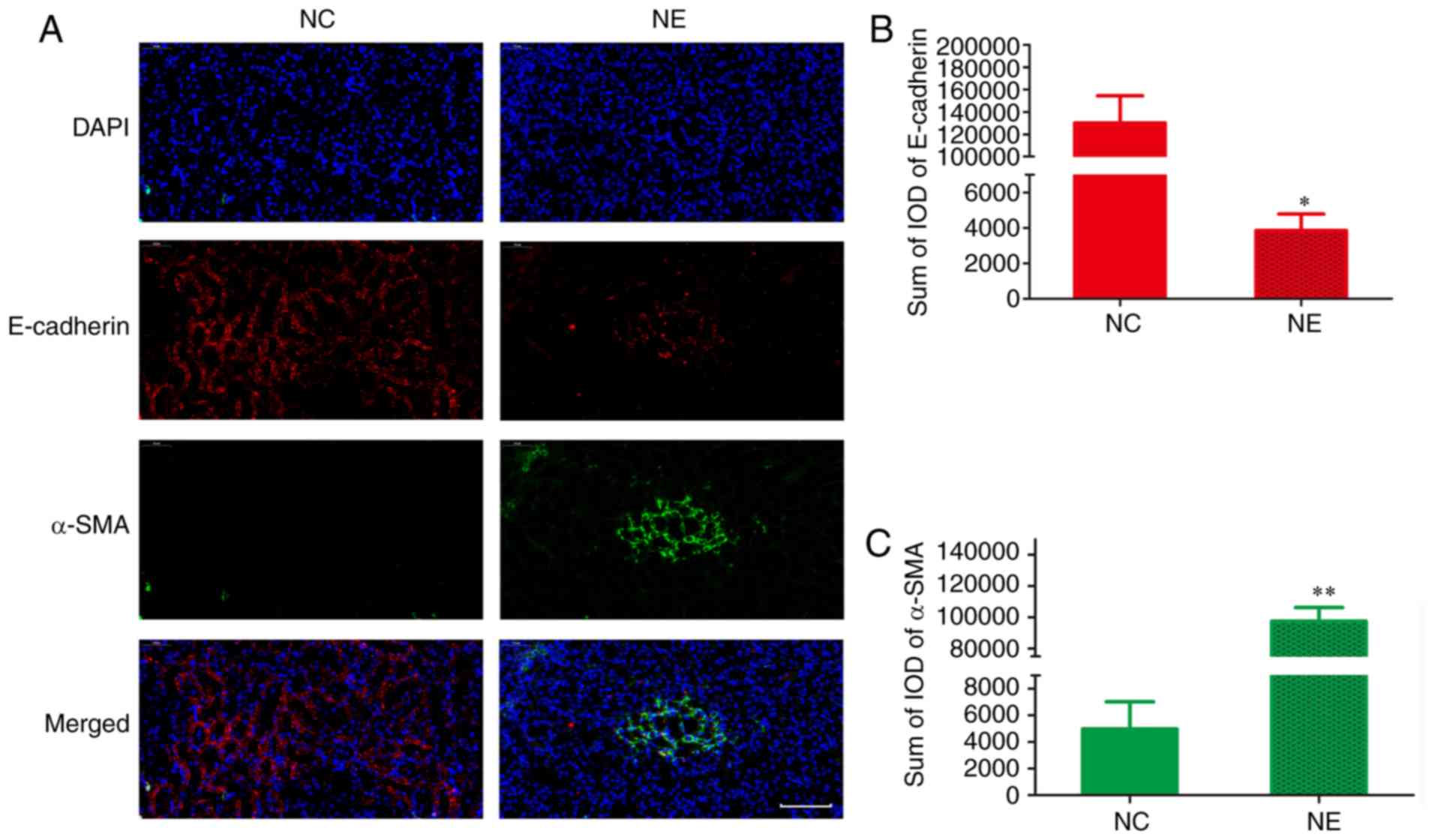
Kidneys were examined using pathological and
immunofluorescent staining (Figs.
1A and 2A, respectively). The
NE group exhibited a significantly higher of kidney index compared
with the NC group (Fig. 1B;
P<0.05). Compared with the NC group, the NE group exhibited
severe renal fibrosis. This was indicated by a significantly higher
sum of IOD in the NE group following Masson staining (Fig. 1C; P<0.05), Sirius red staining
(Fig. 1D; P<0.01) and PASM
staining (Fig. 1E; P<0.01). In
addition, the NE group exhibited significantly upregulated vimentin
(Fig. 1F; P<0.01),
significantly down-regulated E-cadherin (Fig. 2B; P<0.05) and significantly
upregulated α-SMA (Fig. 2C;
P<0.01).
Transcriptomic and bioinformatics
analyses reveal the nephrotoxicity mechanism underlying
tacrolimus
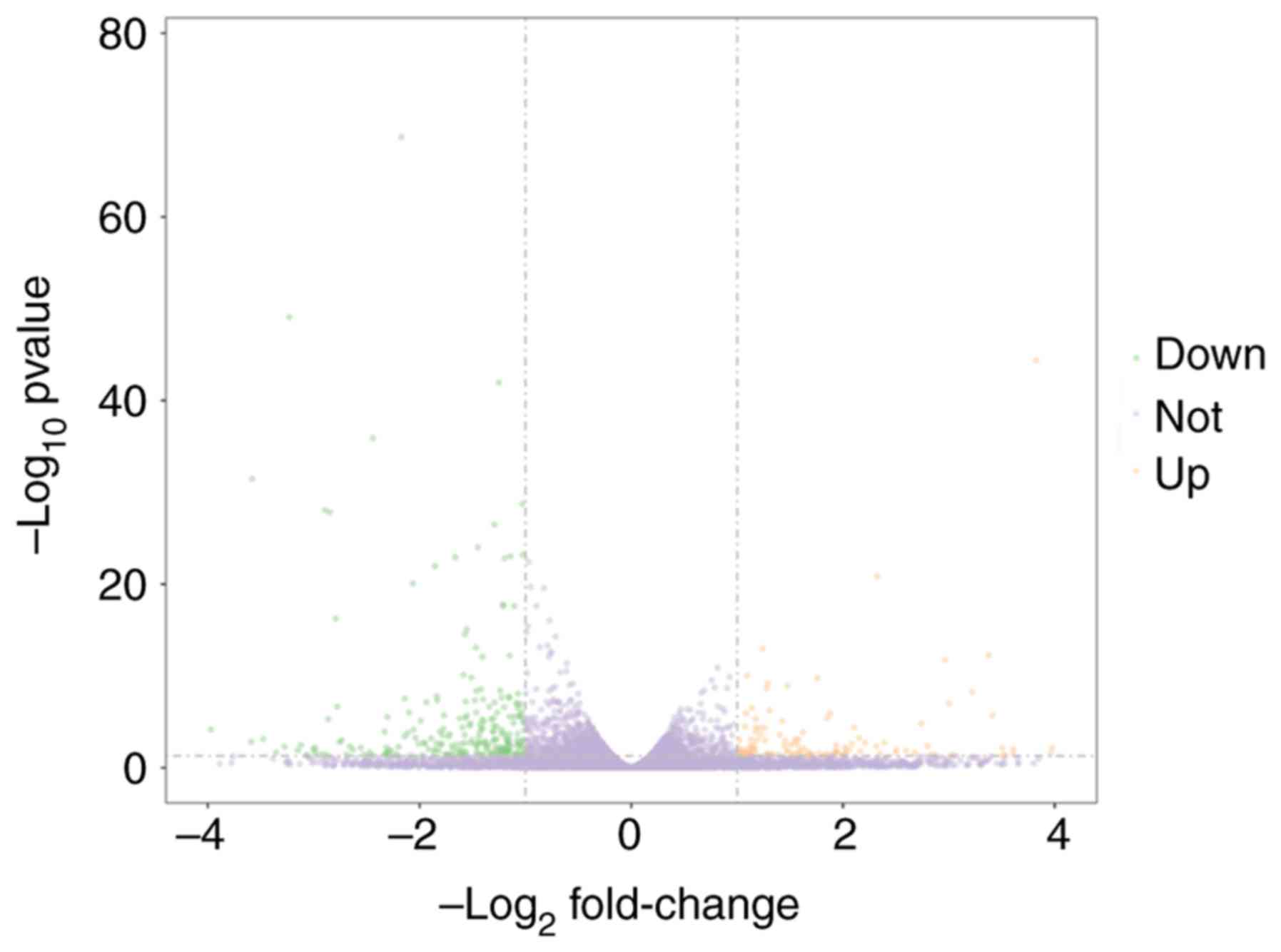
A total of six next-generation sequencing libraries,
including three from the NC group and three from the NE group, were
analyzed. As presented in Fig. 3,
the transcriptomic analysis identified 453 DEGs, including 173
upregulated and 280 downregulated genes. The pathway demonstrating
the highest enrichment following KEGG analysis was
'cytokine-cytokine receptor interaction' (Fig. 4A; P<0.05). Further analysis of
this signaling pathway using KEGG identified that tacrolimus
increased the expression levels of CXCL1, CXCL2, CXCL3 and the
chemokine receptor CXCR2 (Fig.
4B; P<0.05). The potential mechanism underlying
tacrolimus-induced nephrotoxicity is presented in Fig. 5.
Discussion
Tacrolimus is one of the most used and effective
clinical immunosuppressive agents currently available in the
clinic, and it has been widely used for treating patients receiving
renal (33-38), liver (39-44) and lung transplants (45), and for patients with idiopathic
membranous nephropathy (46),
nephritic syndrome (4) and
systemic-onset juvenile idiopathic arthritis (7). However, although tacrolimus has been
demonstrated to exhibit evident benefits, immunosuppressive agents
are associated with the occurrence of acute or chronic renal
toxicity, limiting their clinical use (15).
In addition, it has previously been reported that
the epithetlial-mesenchymal transition (EMT) is significantly
correlated with renal fibrosis, which is associated with
calcineurin inhibitor-mediated nephrotoxicity (21). EMT is one of the basic mechanisms
of renal fibrosis and involves various processes in which
epithelial cells stop exhibiting epithelial characteristics,
including the expression of E-cadherin, and obtain traits specific
of mesenchymal cells, including the upregulation of α-SMA (25,47-48). In addition, it has previously been
reported that vimentin is a potential novel biomarker in renal
fibrosis (25,49).
In the present study, Masson staining, Sirius red
staining and PASM staining were used to examine the pathological
alterations occurring in kidneys. Compared with the NC group, the
tacrolimus nephrotoxicity group exhibited severe renal fibrosis.
Further analysis confirmed that vimentin was upregulated,
E-cadherin was downregulated and α-SMA was upregulated in the
tacrolimus-induced nephrotoxicity group. Subsequently, the exact
mechanism underlying tacrolimus-induced nephrotoxicity was
examined.
Transcriptome analysis can identify both coding and
non-coding RNA, quantifying gene expression heterogeneity in cells,
tissues, organs and even in the whole organism (50). Transcriptome analysis is important
to investigate various processes (51) and it has been widely used to
identify key factors in the progression of multiple diseases
(27,52-53). Kim et al (52), using transcriptome analysis,
identified Tensin 4 as a key effector of cetuximab and a regulator
of the oncogenic activity of KRAS-mutant colorectal cancer cell
lines. Yang et al (27)
reported the transcriptome profiling of brain myeloid cells, and
identified an upregulation of integrin subunit α L, triggering
receptor expressed on myeloid cells 1 and secreted phosphoprotein 1
in Western diet-induced obesity. Siena et al (53) performed a whole transcriptome
analysis in melanoma and identified a correlation between the
expression level of the long non-coding RNA ZEB1-AS1 with invasive
ability of melanoma cells. These previous studies suggested that
the transcriptome has become a reliable tool to identify key
factors in the development and progression of various diseases
(27,52,53). The present study aimed to
investigate the mechanism underlying tacrolimus nephrotoxicity and
to identify novel potential targets via transcriptomic and
bioinformatics analyses.
The KEGG enrichment analysis identified
'cytokine-cytokine receptor interaction' as the pathway most
significantly enriched following tacrolimus-mediated nephrotoxicity
induction. By analyzing components of the 'cytokine-cytokine
receptor interaction' signaling pathway, tacrolimus was identified
to increase the expression levels of CXCL1, CXCL2, CXCL3 and the
chemokine receptor CXCR2.
CXCR2 is a seven-transmembrane G-protein-coupled
receptor that medi ates chemotaxis during immune response, and is
expressed in renal parenchymal cells and neutrophils (54-55). Dornelles et al (56) firstly reported the association
between the increase in CXCR2 expression and nephrotoxicity
following cyclophosphamide treatment. In addition, upregulation of
CXCR2 has been reported in inflammatory diseases, including
psoriasis, atherosclerosis and rheumatoid arthritis (57,58). CXCR2-knockout mice were identified
to be protected against dextran sodium sulfate-mediated colitis and
acute kidney injury. In addition, the expression of cytokines and
chemokines and the level of neutrophil infiltration were reduced in
the colon and kidney of CXCR2-knockout mice (59). Collectively, these previous
studies suggest that CXCR2 may be a promoter of kidney damage.
In conclusion, the mechanism underlying
tacrolimus-induced nephrotoxicity may involve the increase of the
chemokine receptor CXCR2 to promote the upregulation of vimentin
and α-SMA, and the downregulation of E-cadherin, thus accelerating
the renal fibrosis progression. However, the present analysis was
performed in animal models, and validation of the present results
is required in the future by analyzing blood and kidney biopsies
from patients with nephrotoxicity caused by tacrolimus.
Acknowledgments
Not applicable.
Funding
This study was supported by Clinical Pharmacy Key
Specialty Construction Project of Shanghai (grant no. YZ2017/5),
Important Weak Subject Construction Project of Shanghai (grant no.
2016ZB0305), Scientific Research Project of Science and Technology
Commission of Shanghai Municipality (grant no. 18DZ1910604) and the
China Scholarship Council (grant no. 201906100164).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
ZL and HX conceived and designed the study. DW, XC
and MF performed the experiments. DW and XC wrote, reviewed and
edited the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Animal protocols and procedures were approved by The
Animal Care and Use Committee of Children's Hospital of Fudan
University (Shanghai, China) and complied with the appropriate
institutional regulations.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Yoshida T, Nakanishi K, Yoshioka T,
Tsutsui Y, Maeda A, Kondo H and Sako K: Oral tacrolimus oil
formulations for enhanced lymphatic delivery and efficient
inhibition of T-cell's interleukin-2 production. Eur J Pharm
Biopharm. 100:58–65. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Maguire O, Tornatore KM, O'Loughlin KL,
Venuto RC and Minderman H: Nuclear translocation of nuclear factor
of activated T cells (NFAT) as a quantitative pharmacodynamic
parameter for tacrolimus. Cytometry A. 83:1096–1104. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dong QE, Fu R, Liu CY, Ruan EB, Wang XM,
Wang GJ, Qu W, Liu H, Wu YH, Song J, et al: Inhibitory effects of
tacrolimus on effector T cells from patients with severe aplastic
anemia. Zhonghua Yi Xue Za Zhi. 93:1541–1545. 2013.In Chinese.
PubMed/NCBI
|
|
4
|
Wang DD, Chen X and Li ZP: Efficacy and
safety of tacrolimus in treating pediatric refractory nephrotic
syndrome: A meta-analysis. Int J Clin Exp Med. 11:6436–6444.
2018.
|
|
5
|
Ho S, Clipstone N, Timmermann L, Northrop
J, Graef I, Fiorentino D, Nourse J and Crabtree GR: The mechanism
of action of cyclosporin A and FK506. Clin Immunol Immunopathol.
80:S40–S45. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Masuda S and Inui K: An up-date review on
individualized dosage adjustment of calcineurin inhibitors in organ
transplant patients. Pharmacol Ther. 112:184–198. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang D, Chen X and Li Z: Treatment of
patients with systemic-onset juvenile idiopathic arthritis with
tacrolimus. Exp Ther Med. 17:2305–2309. 2019.PubMed/NCBI
|
|
8
|
Wang D, Chen X, Xu H and Li Z: Population
pharmacokinetics and dosing regimen optimisation of tacrolimus in
Chinese pediatric hematopoietic stem cell transplantation patients.
Xenobiotica. 2:1–8. Apr 2–2019.Epub ahead of print.
|
|
9
|
Wang DD, Chen X and Li ZP: Wuzhi capsule
and haemoglobin influence tacrolimus elimination in paediatric
kidney transplantation patients in a population pharmacokinetics
analysis: A retrospective study. J Clin Pharm Ther. 44:611–617.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wang DD, Chen X and Li ZP: Population
pharmacokinetics of sirolimus in pediatric patients with kaposiform
hemangioen-dothelioma: A retrospective study. Oncol Lett.
18:2412–2419. 2019.PubMed/NCBI
|
|
11
|
Wang DD, Chen X and Li ZP: Efficacy and
safety of tacrolimus in Chinese lupus nephritis patients: A
meta-analysis. Int J Clin Exp Med. 12:3056–3064. 2019.
|
|
12
|
Jusko WJ, Thomson AW, Fung J, McMaster P,
Wong SH, Zylber-Katz E, Christians U, Winkler M, Fitzsimmons WE and
Lieberman R: Consensus document: Therapeutic monitoring of
tacrolimus (FK-506). Ther Drug Monit. 17:606–614. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Venkataramanan R, Swaminathan A, Prasad T,
Jain A, Zuckerman S, Warty V, McMichael J, Lever J, Burckart G and
Starzl T: Clinical pharmacokinetics of tacrolimus. Clin
Pharmacokinet. 29:404–430. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Schutte-Nutgen K, Tholking G, Suwelack B
and Reuter S: Tacrolimus-pharmacokinetic considerations for
clinicians. Curr Drug Metab. 19:342–350. 2018. View Article : Google Scholar
|
|
15
|
Staatz CE and Tett SE: Clinical
pharmacokinetics and pharmacodynamics of tacrolimus in solid organ
transplantation. Clin Pharmacokinet. 43:623–653. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Joardar S, Dewanjee S, Bhowmick S, Dua TK,
Das S, Saha A and De Feo V: Rosmarinic acid attenuates
cadmium-induced nephrotoxicity via inhibition of oxidative stress,
apoptosis, inflammation and fibrosis. Int J Mol Sci. 20:E20272019.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gonzalez-Guerrero C, Cannata-Ortiz P,
Guerri C, Egido J, Ortiz A and Ramos AM: TLR4-mediated inflammation
is a key pathogenic event leading to kidney damage and fibrosis in
cyclosporine nephrotoxicity. Arch Toxicol. 91:1925–1939. 2017.
View Article : Google Scholar
|
|
18
|
Al-Gayyar MM, Hassan HM, Alyoussef A,
Abbas A, Darweish MM and El-Hawwary AA: Nigella sativa oil
attenuates chronic nephrotoxicity induced by oral sodium nitrite:
Effects on tissue fibrosis and apoptosis. Redox Rep. 21:50–60.
2016.
|
|
19
|
Nielsen FT, Jensen BL, Hansen PB,
Marcussen N and Bie P: The mineralocorticoid receptor antagonist
eplerenone reduces renal interstitial fibrosis after long-term
cyclosporine treatment in rat: Antagonizing cyclosporine
nephrotoxicity. BMC Nephrol. 14:422013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Okada H, Watanabe Y, Inoue T, Kobayashi T,
Kanno Y, Shiota G, Nakamura T, Sugaya T, Fukamizu A and Suzuki H:
Transgene-derived hepatocyte growth factor attenuates reactive
renal fibrosis in aristolochic acid nephrotoxicity. Nephrol Dial
Transplant. 18:2515–2523. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bennett J, Cassidy H, Slattery C, Ryan MP
and McMorrow T: Tacrolimus modulates TGF-β signaling to induce
epithelial-mesenchymal transition in human renal proximal tubule
epithelial cells. J Clin Med. 5:E502016. View Article : Google Scholar
|
|
22
|
Shihab FS, Bennett WM, Tanner AM and Andoh
TF: Mechanism of fibrosis in experimental tacrolimus
nephrotoxicity. Transplantation. 64:1829–1837. 1997. View Article : Google Scholar
|
|
23
|
Mitamura T, Yamada A, Ishida H, Fujihira
S, Ohara K, Noguchi H and Mine Y: Tacrolimus (FK506)-induced
nephrotoxicity in spontaneous hypertensive rats. J Toxicol Sci.
19:219–226. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Al-Harbi NO, Imam F, Al-Harbi MM, Iqbal M,
Nadeem A, Al-Shahrah OA, Korashy HM, Al-Hosaini KA, Ahmed M and
Bahashwar S: Treatment with aliskiren ameliorates
tacrolimus-induced nephrotoxicity in rats. J Renin Angiotensin
Aldosterone Syst. 16:1329–1336. 2015. View Article : Google Scholar
|
|
25
|
Wang D, Chen X, Fu M and Li Z:
Transcriptomics analysis of sirolimus treatment in lupus nephritis.
Mol Med Rep. 20:245–251. 2019.PubMed/NCBI
|
|
26
|
Wang D, Zhang G, Chen X, Wei T, Liu C,
Chen C, Gong Y and Wei Q: Sitagliptin ameliorates diabetic
nephropathy by blocking TGF-β1/Smad signaling pathway. Int J Mol
Med. 41:2784–2792. 2018.PubMed/NCBI
|
|
27
|
Yang H, Graham LC, Reagan AM, Grabowska
WA, Schott WH and Howell GR: Transcriptome profiling of brain
myeloid cells revealed activation of Itgal, Trem1, and Spp1 in
western diet-induced obesity. J Neuroinflammation. 16:1692019.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Liu J, Yang L, Hou Y, Soteyome T, Zeng B,
Su J, Li L, Li B, Chen D, Li Y, et al: Transcriptomics study on
staphylococcus aureus biofilm under low concentration of
ampicillin. Front Microbiol. 9:24132018. View Article : Google Scholar :
|
|
29
|
Wang K, Li M and Hakonarson H: ANNOVAR:
Functional annotation of genetic variants from high-throughput
sequencing data. Nucleic Acids Res. 38:e1642010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Burden CJ, Qureshi SE and Wilson SR: Error
estimates for the analysis of differential expression from RNA-seq
count data. Peer J. 2:e5762014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kanehisa M and Goto S: KEGG: Kyoto
encyclopedia of genes and genomes. Nucleic Acids Res. 28:27–30.
2000. View Article : Google Scholar
|
|
32
|
Zhang Q, Sun S, Zhu C, Zheng Y, Cai Q,
Liang X, Xie H and Zhou J: Prediction and analysis of weighted
genes in hepato-cellular carcinoma using bioinformatics analysis.
Mol Med Rep. 19:2479–2488. 2019.PubMed/NCBI
|
|
33
|
Andreu F, Colom H, Grinyo JM, Torras J,
Cruzado JM and Lloberas N: Development of a population PK model of
tacrolimus for adaptive dosage control in stable kidney transplant
patients. Ther Drug Monit. 37:246–255. 2015. View Article : Google Scholar
|
|
34
|
Benkali K, Rostaing L, Premaud A, Woillard
JB, Saint-Marcoux F, Urien S, Kamar N, Marquet P and Rousseau A:
Population pharmacokinetics and bayesian estimation of tacrolimus
exposure in renal transplant recipients on a new once-daily
formulation. Clin Pharmacokinet. 49:683–692. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Bergmann TK, Hennig S, Barraclough KA,
Isbel NM and Staatz CE: Population pharmacokinetics of tacrolimus
in adult kidney transplant patients: Impact of CYP3A5 genotype on
starting dose. Ther Drug Monit. 36:62–70. 2014.
|
|
36
|
Han N, Ha S, Yun HY, Kim MG, Min SI, Ha J,
Lee JI, Oh JM and Kim IW: Population
pharmacokinetic-pharmacogenetic model of tacrolimus in the early
period after kidney transplantation. Basic Clin Pharmacol Toxicol.
114:400–406. 2014. View Article : Google Scholar
|
|
37
|
Zhao W, Elie V, Roussey G, Brochard K,
Niaudet P, Leroy V, Loirat C, Cochat P, Cloarec S, Andre JL, et al:
Population pharmacokinetics and pharmacogenetics of tacrolimus in
de novo pediatric kidney transplant recipients. Clin Pharmacol
Ther. 86:609–618. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Zuo XC, Ng CM, Barrett JS, Luo AJ, Zhang
BK, Deng CH, Xi LY, Cheng K, Ming YZ, Yang GP, et al: Effects of
CYP3A4 and CYP3A5 polymorphisms on tacrolimus pharmacokinetics in
Chinese adult renal transplant recipients: A population
pharmacokinetic analysis. Pharmacogenet Genomics. 23:251–261. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Lu YX, Su QH, Wu KH, Ren YP, Li L, Zhou TY
and Lu W: A population pharmacokinetic study of tacrolimus in
healthy Chinese volunteers and liver transplant patients. Acta
Pharmacol Sin. 36:281–288. 2015. View Article : Google Scholar :
|
|
40
|
Musuamba FT, Guy-Viterbo V, Reding R,
Verbeeck RK and Wallemacq P: Population pharmacokinetic analysis of
tacrolimus early after pediatric liver transplantation. Ther Drug
Monit. 36:54–61. 2014.
|
|
41
|
Wallin JE, Bergstrand M, Wilczek HE,
Nydert PS, Karlsson MO and Staatz CE: Population pharmacokinetics
of tacrolimus in pediatric liver transplantation: Early
posttransplantation clearance. Ther Drug Monit. 33:663–672. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Yang JW, Liao SS, Zhu LQ, Zhao Y, Zhang Y,
Sun XY, Rao W, Qu W, Li WZ and Sun LY: Population pharmacokinetic
analysis of tacrolimus early after Chinese pediatric liver
transplantation. Int J Clin Pharmacol Ther. 53:75–83. 2015.
View Article : Google Scholar
|
|
43
|
Zhang XQ, Wang ZW, Fan JW, Li YP, Jiao Z,
Gao JW, Peng ZH and Liu GL: The impact of sulfonylureas on
tacrolimus apparent clearance revealed by a population
pharmacokinetics analysis in Chinese adult liver-transplant
patients. Ther Drug Monit. 34:126–133. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Zhu L, Yang J, Zhang Y, Jing Y, Zhang Y
and Li G: Effects of CYP3A5 genotypes, ABCB1 C3435T and G2677T/A
polymorphism on pharmacokinetics of Tacrolimus in Chinese adult
liver transplant patients. Xenobiotica. 45:840–846. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Monchaud C, de Winter BC, Knoop C, Estenne
M, Reynaud-Gaubert M, Pison C, Stern M, Kessler R, Guillemain R,
Marquet P and Rousseau A: Population pharmacokinetic modelling and
design of a bayesian estimator for therapeutic drug monitoring of
tacrolimus in lung transplantation. Clin Pharmacokinet. 51:175–186.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Di J, Qian Q, Yang M, Jiang Y, Zhou H, Li
M and Zou Y: Efficacy and safety of long-course tacrolimus
treatment for idiopathic membranous nephropathy. Exp Ther Med.
16:979–984. 2018.PubMed/NCBI
|
|
47
|
Chen X, Yang Y, Liu C, Chen Z and Wang D:
Astragaloside IV ameliorates high glucoseinduced renal tubular
epithelialmesenchymal transition by blocking mTORC1/p70S6K
signaling in HK2 cells. Int J Mol Med. 43:709–716. 2019.
|
|
48
|
Badid C, Desmouliere A, Babici D,
Hadj-Aissa A, McGregor B, Lefrancois N, Touraine JL and Laville M:
Interstitial expression of alpha-SMA: An early marker of chronic
renal allograft dysfunction. Nephrol Dial Transplant. 17:1993–1998.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Cao YH, Lv LL, Zhang X, Hu H, Ding LH, Yin
D, Zhang YZ, Ni HF, Chen PS and Liu BC: Urinary vimentin mRNA as a
potential novel biomarker of renal fibrosis. Am J Physiol Renal
Physiol. 309:F514–F522. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Granjeaud S, Bertucci F and Jordan BR:
Expression profiling: DNA arrays in many guises. Bioessays.
21:781–790. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Jiang Z, Zhou X, Li R, Michal JJ, Zhang S,
Dodson MV, Zhang Z and Harland RM: Whole transcriptome analysis
with sequencing: Methods, challenges and potential solutions. Cell
Mol Life Sci. 72:3425–3439. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Kim S, Kim N, Kang K, Kim W, Won J and Cho
J: Whole transcriptome analysis identifies TNS4 as a key effector
of cetuximab and a regulator of the oncogenic activity of KRAS
mutant colorectal cancer cell lines. Cells. 8:8782019. View Article : Google Scholar :
|
|
53
|
Siena ÁDD, Plaça JR, Araújo LF, de Barros
II, Peronni K, Molfetta G, de Biagi CAO Jr, Espreafico EM, Sousa JF
and Silva WA Jr: Whole transcriptome analysis reveals correlation
of long noncoding RNA ZEB1-AS1 with invasive profile in melanoma.
Sci Rep. 9:113502019. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Svensson M, Irjala H, Svanborg C and
Godaly G: Effects of epithelial and neutrophil CXCR2 on innate
immunity and resistance to kidney infection. Kidney Int. 74:81–90.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Li L, Huang L, Vergis AL, Ye H, Bajwa A,
Narayan V, Strieter RM, Rosin DL and Okusa MD: IL-17 produced by
neutrophils regulates IFN-gamma-mediated neutrophil migration in
mouse kidney ischemia-reperfusion injury. J Clin Invest.
120:331–342. 2010. View Article : Google Scholar
|
|
56
|
Dornelles FN, Andrade EL, Campos MM and
Calixto JB: Role of CXCR2 and TRPV1 in functional, inflammatory and
behavioural changes in the rat model of cyclophosphamide-induced
haemorrhagic cystitis. Br J Pharmacol. 171:452–467. 2014.
View Article : Google Scholar :
|
|
57
|
Mihara K, Smit MJ, Krajnc-Franken M,
Gossen J, Rooseboom M and Dokter W: Human CXCR2 (hCXCR2) takes over
function-alities of its murine homolog in hCXCR2 knockin mice. Eur
J Immunol. 35:2573–2582. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Liu L, Sun H, Wu S, Tan H, Sun Y, Liu X,
Si S, Xu L, Huang J, Zhou W, et al: IL17A promotes CXCR2dependent
angiogenesis in a mouse model of liver cancer. Mol Med Rep.
20:1065–1074. 2019.PubMed/NCBI
|
|
59
|
Ranganathan P, Jayakumar C, Manicassamy S
and Ramesh G: CXCR2 knockout mice are protected against
DSS-colitis-induced acute kidney injury and inflammation. Am J
Physiol Renal Physiol. 305:F1422–F1427. 2013. View Article : Google Scholar : PubMed/NCBI
|