Introduction
Colorectal cancer (CRC) is the third most frequent
cancer worldwide and a common cause of cancer death primarily due
to metastases that are resistant to conventional therapy (1). Over the last couple of years, a
series of monoclonal antibodies targeting different tumor cell
surface antigens have been tested in both experimental and clinical
studies (2–5). Therapeutical antibodies have been
successfully used for the treatment of metastatic CRC or after the
failure of conventional chemotherapy, including cetuximab and
panitumumab, antibodies to endothelial cell growth factor receptor
(anti-EGFR), and bevacizumab, an antibody to vascular endothelial
growth factor (anti-VEGF). Several drugs are under development with
proven efficacy in phase II and III trials. However, the benefit of
anti-EGFR therapy was limited to patients who had KRAS
wild-type tumors with normal PTEN expression (6–8).
HER2 is a 185-kDa transmembrane tyrosine kinase
receptor, and belongs to the family of epidermal growth factor
receptors (EGFRs), playing critical roles in epithelial cell growth
and differentiation. HER2 overexpression has been found to be
involved in pathogenesis of several human cancers (9–15).
Although a dozen different ligands are known to bind to EGFRs,
there is no ligand to be shown to bind directly to HER2. Instead,
HER2 is thought to function as a co-receptor for other members of
the ErbB/HER family, and frequently activated upon ligand binding
to any of the other ErbB/HER receptors. Therefore, it is not
surprising that HER2 has also been implicated in the development of
carcinomas. In CRC the prevalence of HER-2/neu
overexpression ranges from 0 to 83% (16–18),
a big variation largely due to the lack of standardization of the
detection methods. The success of HER-2/neu directed therapy
in breast cancer suggests its potential role in the treatment of
other tumors expressing HER2, including CRC. Herceptin®
has been shown to inhibit colony formation of the HCA-7 colon
cancer cell line and HCA-7 tumor xenografts (19).
In addition to the development of therapeutics for
new targets, another approach to improve current antibody therapy
was the development of bispecific antibodies. Cancer
immunotherapies involving bispecific antibodies mediated-killing
have been widely explored. Bispecific antibodies were first
developed two decades ago and several molecules targeting different
tumor cell surface antigens have been tested in clinical studies
(20,21). In this study, clinically approved
anti-CD3 antibody was chemically conjugated with Herceptin
antibody. The anti-CD3 x anti-HER2 bispecific antibody (HER2Bi-Ab)
was then used to direct the activated T cells (ATCs) to kill
colorectal carcinoma targets. Armed with HER2Bi-Ab, ATCs exhibited
high levels of specific cytotoxicity and proliferation ability. The
efficacy of HER2Bi-Ab for the inhibition of HER2-positive CRCs in
SCID-Beige mouse model was also demonstrated.
Materials and methods
Cell lines and mice
Colo205-luc, HT-29-luc, BXPC-3-luc, PC-3M-luc,
Hela-luc, and K562-luc cell lines were all from Caliper Life
Sciences. The primary culture and the metastatic culture were
derived from freshly isolated colon carcinoma cells from patients
of primary colon carcinoma or hepatic metastasis of colonic
carcinoma, respectively, in 302 Military Hospital of China. The
consent was obtained from the patients before sample collection.
The study complied with the Declaration of Helsinki and was
approved by the Biomedical Research Ethics Committee of CAS Key
Laboratory of Pathogenic Microbiology and Immunology. The agents
for cell culture were all from Gibco Co. Beige-SCID mice (8–10
weeks) were purchased from Vital River Laboratories.
Isolation of peripheral blood lymphocytes
and preparation and cryopreservation of activated T
lymphocytes
Peripheral mononuclear blood cells (PBMCs) were
isolated using Ficoll density gradient centrifugation from healthy
donors supplied by the Beijing Blood Bank. PBMCs were cultured at
1×106/ml in RPMI-1640 medium supplemented with 10% FBS
and 5 μg/ml anti-CD3 mAb and 100 IU/ml recombinant human IL-2 at
1×106/ml. Half-volume medium exchange was performed
every 3 days with medium containing fresh 100 IU/ml recombinant
human IL-2 as the method previously described (22). On day 14, ATC expansion products of
donors were on average 98.85±1.06% CD3+ cells
(38.4±18.10% CD3+CD4+ cells, and 66.35±9.83%
CD3+CD8+ T cells), the cells were used
immediately or cryopreserved for further use. Based on an informed
consent, this project was approved by the Biomedical Research
Ethics Committee of CAS Key Laboratory of Pathogenic Microbiology
and Immunology.
Synthesis of HER2Bi-Ab and arming of
ATCs
Anti-HER2 (Herceptin®; Roche) was reacted
with sulfo-SMCC and anti-CD3 (OKT3; eBioscience; 85-16-0037-85) was
reacted with Traut’s reagents as previously described (23). Cryopreserved ATCs were thawed, and
armed with HER2Bi at a concentration of 50 ng/106 cells
at room temperature for 30 min followed by washing the cells to
eliminate unbound antibodies. The combination of OKT3 (50
ng/106 cells) and Herceptin® (50
ng/106 cells) pre-incubated ATCs were used as control
unarmed ATCs.
Cytotoxicity assay
Cytotoxicity was measured with a luciferase
quantitative assay (23–25). Target cells were seeded in
duplicates in 96-well U-bottom microplates at 1×104/well
before the addition of HER2Bi-armed, or unarmed ATCs at various
effector-to-target (E/T) ratios. Effector cells and tumor cells
were allowed to interact at 37°C for 18 h. A final concentration of
0.15 mg/ml D-luciferin (Synchem Chemie; Bc219-05) was added to each
well.
IFN-γ ELISA
Target cells were plated in 96-well U-bottom
microplates at a concentration of 1×104/well at 37°C
overnight. HER2Bi-armed, or unarmed ATCs were then added at an E/T
ratio of 5:1 to target cells and incubated for 18 h. The cell free
supernatants were collected, and the IFN-γ production was measured
by using a human IFN-γ ELISA kit (Thermo Scientific) according to
the manufacturer’s instructions.
Flow cytomet ric analysis
The ant i-CD69-PE, anti-CD3-FITC, anti-mouse
IgG-FITC secondary antibodies were from eBioscience, and anti-human
IgG-FITC secondary antibody was from Beijing Zhongshan Golden
Bridge Biotechnology, Co., Ltd. The cells were assayed with a Guava
EasyCyte flow cytometer (Guava Technologies, Inc.) and the data
analysis was carried out with FlowJo software version 7.6.1 (Tree
Star, Inc.).
In vitro cell proliferation assay
For evaluating Herceptin® on colorectal
tumor cell proliferation in vitro, colon carcinoma cells
were seeded into 96-well plates in triplicates and incubated with
the fresh medium or Herceptin® at the indicated
concentration for 72 h. For evaluating HER2Bi-armed ATCs on
colorectal tumor cell proliferation in vitro, HT29-luc were
seeded (2×104/well) into 96-well plates in triplicates
and allowed to adhere overnight. The following day, the medium was
removed, and fresh medium alone or containing the unconjugated mAbs
(50 ng/ml), ATCs (2×105/well), HER2Bi-armed ATCs
(2×105/well, armed with 50 ng/HER2Bi/106
ATCs) or unarmed ATCs was added to wells. Cultures were incubated
for 18 h, then medium was removed and 100 μl of fresh serum-free
medium containing 1/10 (v/v) Cell Counting kit-8 (CCK8; Dojindo
Laboratories) reagent was added to each well and incubated for an
additional 3 h. After incubation, the absorbancy of colorectal
tumor cells was measured using a 96-well plate reader at 450 nm.
Cell proliferation was assessed by the absorbance values according
to the manufacturer’s protocol.
In vivo tumor inhibition studies
In tumor prevention studies, Colo205-luc cells
(1×106/mouse) were mixed with HER2Bi-armed ATCs
(1×107/mouse) or unarmed-ATCs. The cell mixtures were
immediately inoculated subcutaneously on the rear flank of five
SCID-Beige mice per group. In tumor growth delay studies,
SCID-Beige mice (n=5 mice per group) were injected i.p. with
3×106 Colo205-luc cells. Subsequently, HER2Bi-armed ATCs
(3×107/mouse) or control ATCs were administered i.p. on
day 3, 10, and 17. In order to follow up the tumor growth, in
vivo bioluminescence imaging was operated on the indicated days
for 4 weeks. Bioluminescent imaging was taken using Xenogen
IVIS-100 imaging system with Living Image software (Caliper Life
Sciences). The signal intensity of tumor burdens was expressed as
total photons/sec/cm2
(p/sec/cm2/sr).
Statistical analysis
All experiments were repeated at least twice and
mostly three times. Data were analyzed using Graphpad Prism 5
software, the data are presented as the means ± SD. Unpaired
Student’s t-test (two-tailed) or the Mann-Whitney test was used for
comparison of two groups where appropriate. One-way analysis of
variance (ANOVA) followed by Dunnett’s post hoc for multiple
comparison. P<0.05 was considered as statistically significant.
The number with a significant difference from a control is denoted
by an asterisk in the figures.
Results
HER2 overexpression in human CRC
cells
The surface expression of HER2 on human tumors from
different tissue origins was assessed by FACS analysis including
CRC (Colo205-luc and HT-29-luc), pancreatic cancer (BXPC3-luc),
prostate cancer (PC-3M-luc), cervix cancer (Hela-luc), and leukemia
(K652-luc). As shown in Fig. 1,
HER2 expression measured as mean fluorescent intensity (MFI) in CRC
cells (Colo205-luc: 366; HT29-luc: 75.7) was much higher than that
in other tumor cells (BXPC3-luc: 8.9; PC-3M-luc: 22.7; Hela-luc:
34.8). HER2 was not detected on K562 cells used as a negative
control.
Preparation and characterization of
HER2Bi and ATCs
Herceptin® antibody was hetero-conjugated
with OKT3 chemically and named as HER2Bi (Fig. 2A). The binding specificity of
HER2Bi against HER2 was tested. Colo205-luc cells were first
stained by HER2Bi, then an anti-mouse IgG-FITC was added to detect
the CD3 moiety of HER2Bi-Ab. Only functionally bispecific HER2Bi
antibody was able to bind to Colo205-luc cells by HER2 recognized
Herceptin® and be detected through mouse origin OKT3 by
anti-mouse secondary antibody. As shown in Fig. 2B, positively stained cells were
detected in 91.3% of the Colo205-luc population with an MFIof 48.8.
Moreover, binding of HER2Bi-Ab on HER2+ cells was
confirmed by FITC goat anti-human IgG to detect the anti-HER2
moiety of the HER2Bi-Ab (Fig. 2C).
To evaluate the binding of HER2Bi-Ab to CD3+ cells, PBMC
were incubated with HER2Bi-Ab, and the binding of HER2Bi-Ab to
CD3+ cells was evaluated by FITC goat anti-mouse IgG to
detect the anti-CD3 moiety of the HER2Bi-Ab (Fig. 2D). In contrast, HER2Bi-Ab did not
bind to CD3−HER2−-K652 cells (Fig. 2E).
 | Figure 2General scheme for the generation of
anti-CD3 x anti-HER2 bispecific antibody (HER2Bi-Ab). (A) General
scheme for the generation of HER2Bi-Ab. (B) Flow cytometry based
binding assay for HER2Bi-Ab. Colo205-luc cells were incubated with
HER2Bi-Ab (shaded histogram) or combination of OKT3 and
Herceptin® (the black line), HER2Bi-Ab binding was
evaluated by FITC goat anti-mouse IgG to detect the anti-CD3 moiety
of the HER2Bi-Ab. (C) HT29-luc cells were incubated with HER2Bi-Ab
(shaded histogram), Herceptin® (dot histogram), or
control IgG (open histogram), HER2Bi-Ab binding was analyzed by
FITC goat anti-human IgG to detect the anti-HER2 moiety of the
HER2Bi-Ab. (D) Peripheral mononuclear blood cells (PBMCs) were
incubated with HER2Bi-Ab (shaded histogram), OKT3 (dot histogram),
or control IgG (open histogram), the HER2Bi-Ab binding was analyzed
by FITC goat anti-mouse IgG to detect the anti-CD3 moiety of the
HER2Bi-Ab. (E) K562cells were incubated with HER2Bi-Ab (shaded
histogram), OKT3 (dot histogram), or control IgG (open histogram),
the HER2Bi-Ab binding was analyzed by FITC-goat-anti-mouse IgG to
detect the anti-CD3 moiety of the HER2Bi-Ab. |
Cytotoxicity of HER2Bi-armed ATC with
IFN-γ production on different tumor cell lines
The amount of HER2Bi required to arm ATCs ranged
from 5 to 500 ng/106 cells. Since 50 and 500
ng/106 cells showed similar cytotoxicity, we chose 50
ng/106 ATCs as the concentration of HER2Bi for all
subsequent experiments, and ATCs mixed with both individual OKT3
and Herceptin® were used as unarmed ATC control.
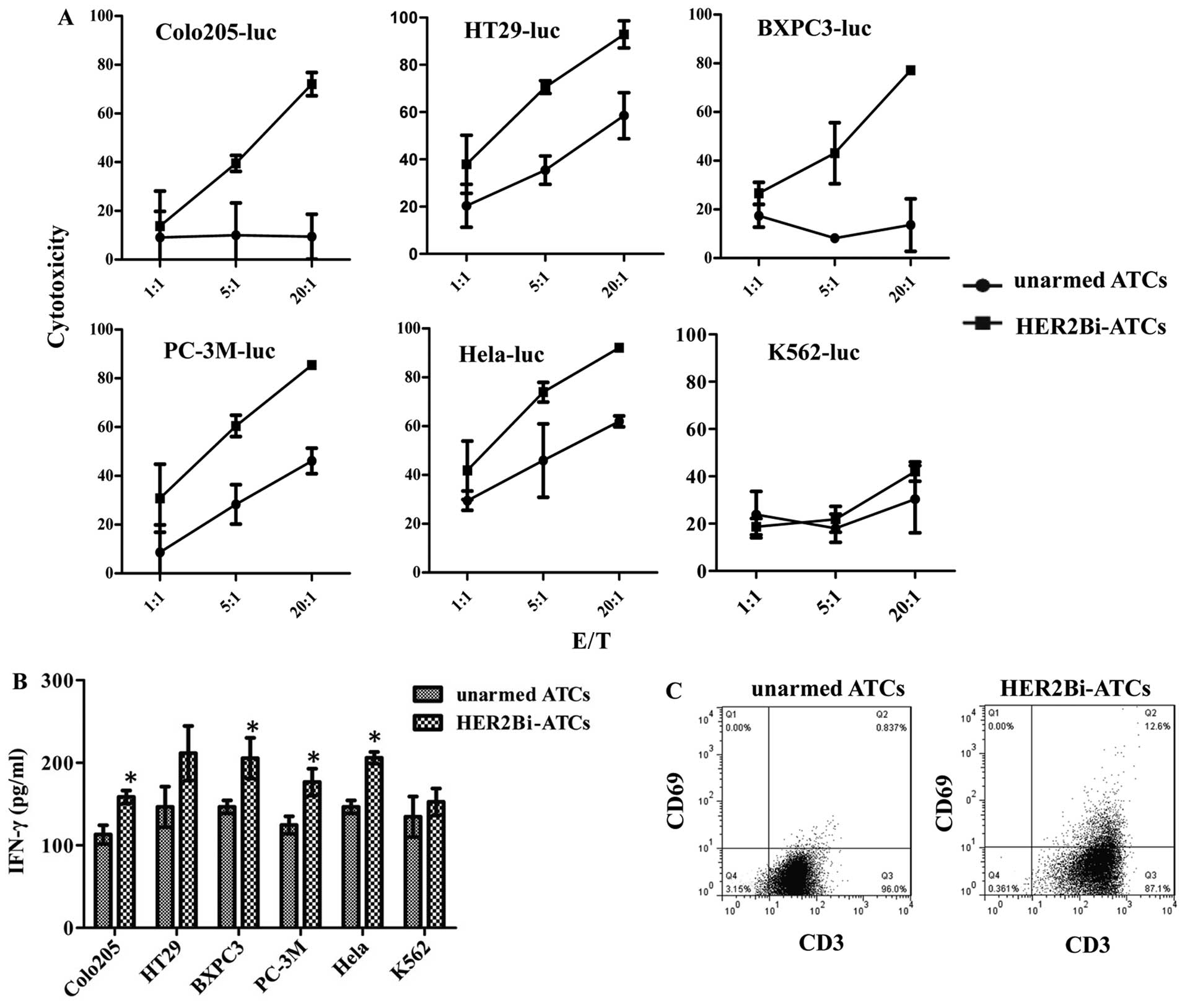
Cytotoxic effects of HER2Bi-armed ATCs on different
HER2+ tumor cells were tested in vitro. The
assays were performed at E/T ratios of 1:1, 5:1 and 20:1. After 18
h incubation with HER2Bi-armed ATCs or unarmed ATCs,
bioluminescence imaging signal in tumor cells expressed in photons
per second was converted into living cell number and the
cytotoxicity assays was calculated at the indicated E/T ratios. As
shown in Fig. 3A, the percentage
of cytotoxicity with armed ATCs was significantly greater than that
with unarmed effectors at E/T ratio of 5:1 and 20:1 in Colo205-luc,
HT29-luc, BXPC-3, PC-3M-luc, and Hela-luc cells.
To analyze the cytokines along with the
cytotoxicity, supernatants of cell cultures were analyzed for IFN-γ
production at E/T ratio of 5:1. As shown in Fig. 3B, significant increase was observed
for IFN-γ secretion by HER2Bi-armed ATCs over their unarmed ATC
counterparts when ATCs were co-cultured with Colo205-luc,
BXPC3-luc, PC-3M-luc or Hela-luc cells, respectively (P<0.05).
Moreover, FACS analysis of HER2Bi-armed ATCs showed an increased
CD69 expression over their unarmed ATCs counterparts (Fig. 3C).
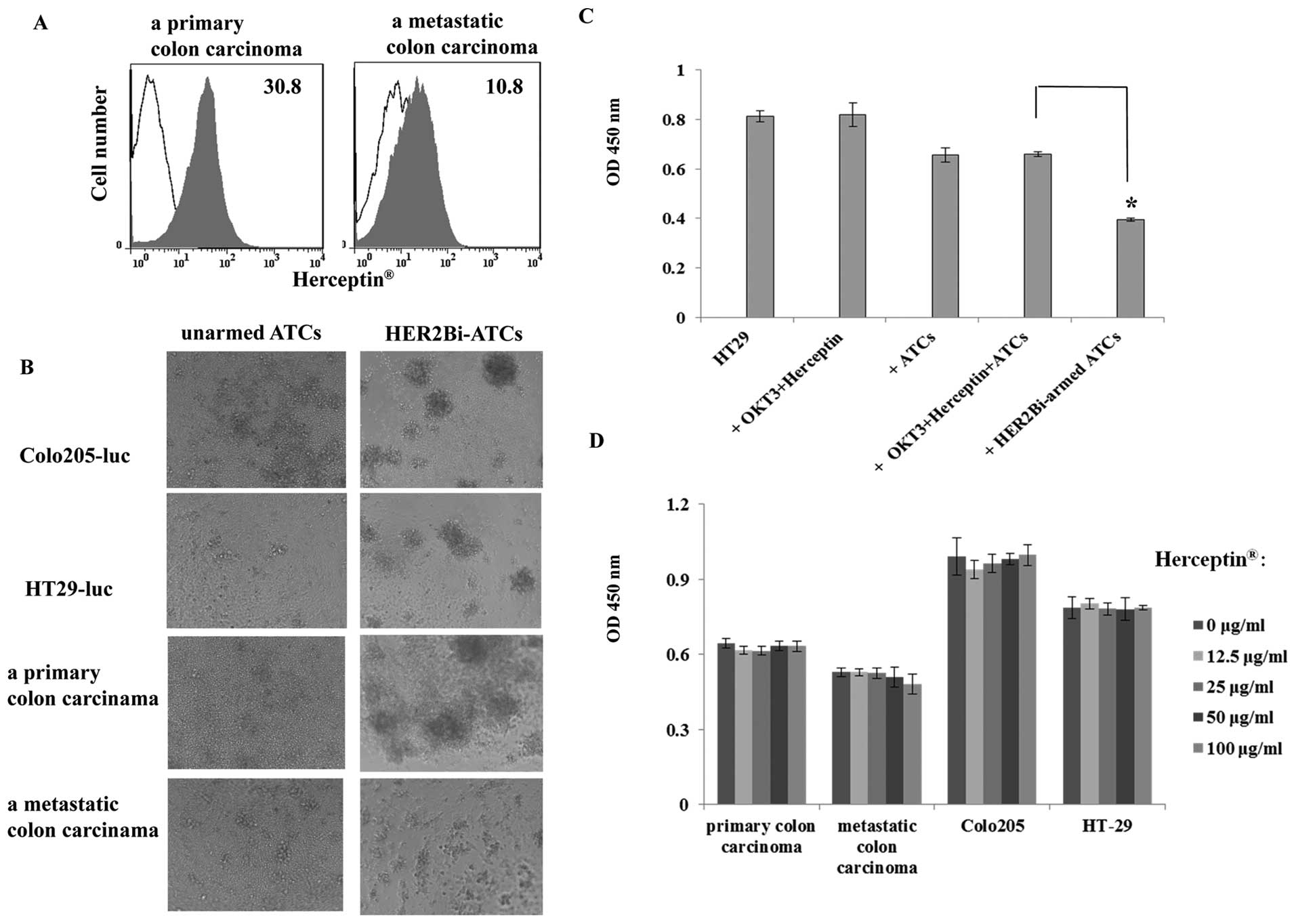
Cells derived from both primary and metastatic human
colorectal carcinoma were tested to evaluate whether they also
expressed high levels of HER2 proteins. As shown in Fig. 4A, HER2-positive stained cells were
detected by FACS analysis in 90% of the primary colorectal
carcinoma cell population with an MFIof 30.8 and in 50% of the
metastatic colorectal carcinoma cell population with an MFIof 10.8.
Then, HER2Bi-armed ATCs were tested for cytotoxicity on HER2
positive primary cells derived from colorectal carcinoma. The
assays were performed at E/T ratio of 10:1. After 18 h incubation
with HER2Bi-armed ATCs or unarmed ATCs, as shown in Fig. 4B, real-time photographs of each
colorectal carcinoma group were taken at ×200 magnification. It was
demonstrated that HER2Bi-ATCs, but not equivalent number of
unarmed-ATCs, aggregated with all the four colorectal carcinoma
cell types, clustering around the edge of targeting cell bulk,
which showed the specific lysis of HER2Bi-ATCs.
The growth inhibition of colorectal
carcinoma cells by HER2Bi-armed ATCs
Furthermore, HER2Bi-armed ATCs were tested for the
inhibitory efficacy on HER2 positive colorectal carcinoma. In cell
proliferation assay, unconjugated mAbs (OKT3 and
Herceptin®), ATC alone, a combination of OKT3 and
Herceptin® with ATC (unarmed ATC), or HER2Bi-armed ATC
(E/T ratio of 10:1) were co-cultured with HT29-luc cells for 18 h,
respectively. As expected, HER2Bi-armed ATCs showed a superior
growth inhibition on colorectal carcinoma cells, compared to the
other groups (Fig. 4C).
Unexpectedly, even at the concentration of 100 μg/ml,
Herceptin® did not inhibit the proliferation of
colorectal tumor cells after 72 h incubation in vitro
(Fig. 4D).
HER2Bi-armed ATCs inhibited Colo205 tumor
growth in SCID-Beige mice
To determine whether HER2Bi-armed ATCs could prevent
tumor growth in vivo, SCID-Beige mice were engrafted
subcutaneously with Colo205-luc cells. The growth of tumor was
monitored with bioluminescent imaging. In Fig. 5A, results of three representative
mice of each group are shown. When mice were co-injected with
unarmed-ATCs, the light signal increased over time from day 1 to
28. In contrast, the signal disappeared on day 1 and vanished
completely from day 7 to 28 when mice were co-injected with
HER2Bi-armed ATCs. Once injected, mice were given no further
treatment but were monitored weekly for tumor development up
through day 28 following initial injection. The mean
bioluminescence signal of each test group correlated with the
number of living Colo205-luc cells as shown in Fig. 5B.
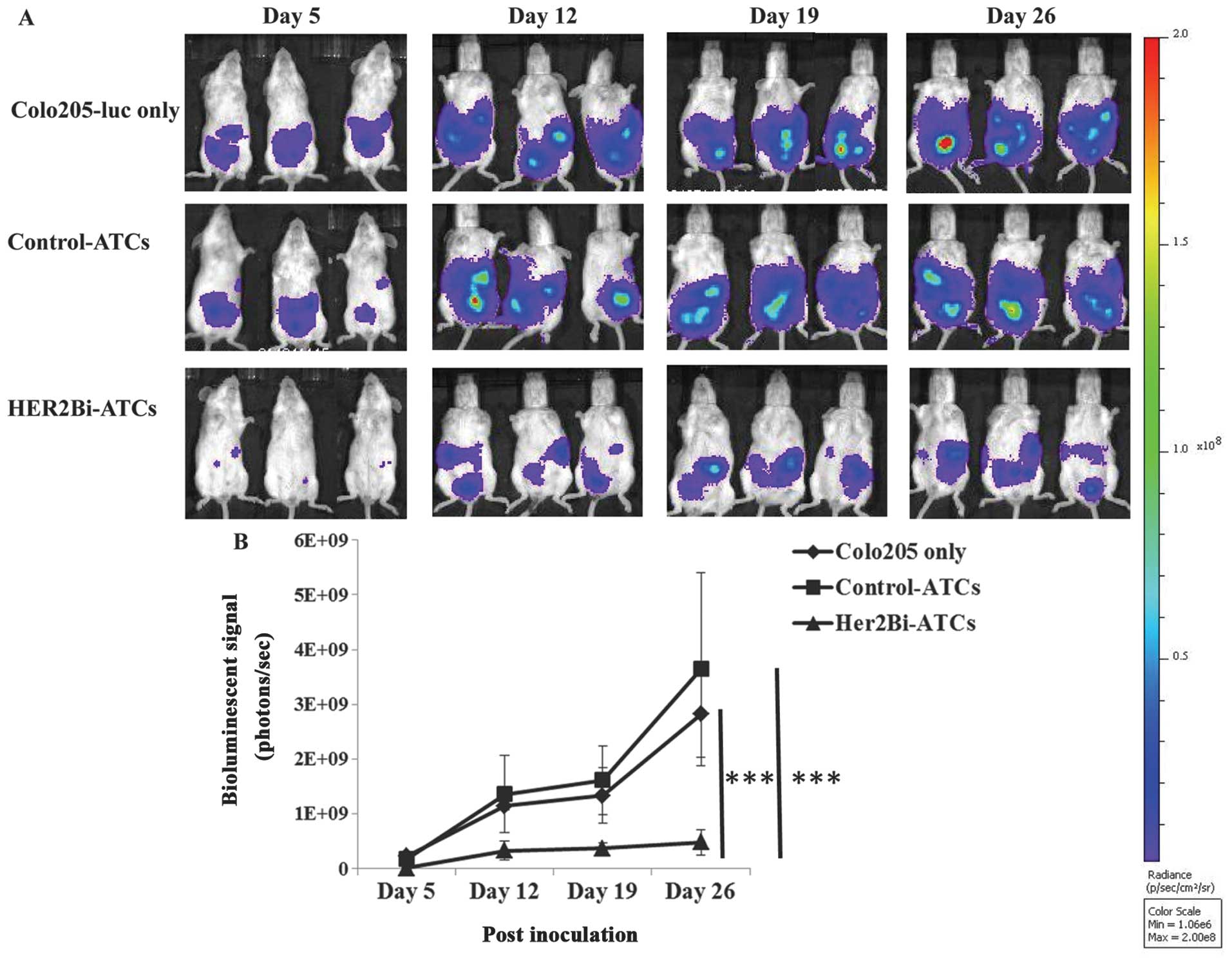
To further determine whether HER2Bi-armed ATCs could
suppress tumor growth in vivo, SCID-Beige mice were
engrafted intraperitoneally with Colo205-luc cells. Three days
later, mice were treated with HER2Bi-armed ATCs or control ATCs
weekly three times. The growth of tumor was monitored with
bioluminescent imaging. In Fig.
6A, three representative mice of each group are shown. When
Colo205-luc cells were inoculated alone, light signal increased
over time. A similar kinetics of tumor growth was shown in mice
that were injected with control ATCs. As for mice treated with
HER2Bi-armed ATCs, the signal diminished from day 5 to 26 compared
with other two groups. The mean bioluminescence signal of each test
group correlated with the number of living Colo205-luc cells was
shown in Fig. 6B. HER2Bi-armed
ATCs inhibited the tumor growth significantly, whereas control ATCs
did not, at every check point.
Discussion
Therapeutic antibodies such as bevacizumab,
cetuximab, and panitumumab significantly improve survival rates of
patients with advanced CRC. However, due to the limitations of
conventional antibodies, including the redundancy in antibody
targeted molecular pathways, inadequate exposure of the tumor due
to the antibody limited tissue distribution, and immunogenicity
caused by repeatable treatment, alternative approaches to improve
current antibody strategy are urgently needed. One improvement is
the use of T cell directed bispecific antibodies, comprising of an
anti-CD3 mAb hetero-conjugated to a different mAb specific to a
selected tumor-associated antigen (TAA). Such a bispecific antibody
will make every T cell TAA-specific to redirect T cells to target
tumor cells. HER2 is an ideal candidate used as a target by various
tumor imaging and antibody-based therapeutic approaches. Phase I/II
immunotherapy with HER2Bi-Ab and/or armed ATCs are currently
ongoing in women with metastatic breast cancer (26,27).
In this study, we tested whether HER2 is a useful
target for the development of novel bispecific Ab therapeutics in
CRC, and examined in vitro and in vivo antitumor
effects of HER2Bi-armed ATCs. Our study findings are relevant to
the therapeutic application of target HER2 against CRC. The high
expression of HER2 in colorectal carcinoma was confirmed by FACS
analysis. In addition, primary or metastatic colon carcinoma cell
cultures were also shown to express high level of HER2 antigen. In
our present study HER2Bi-armed ATCs provided significant
anti-proliferative and cytotoxic activity against HER2-positive
colorectal carcinoma cells although anti-HER2 antibody alone had no
inhibitory effect to colorectal carcinoma cells tested in
vitro. Additionally, HER2Bi-armed ATCs expressed higher level
of activation marker CD69 and secreted a higher level of IFN-γ than
unarmed ATC counterpart against colorectal carcinoma target cells.
Furthermore, infusion of HER2Bi-armed ATCs remarkably inhibited the
growth of colorectal carcinoma cells in the xenograft mouse tumor
model.
Our results have shown that ATCs armed with HER2Bi
released cytokine IFN-γ upon incubation with the tumor cells. The
increased secretion of cytokine demonstrated that ATCs were being
reactivated upon binding to tumor cells. IFN-γ secreted by
HER2Bi-armed ATCs in the presence of tumor may not only cause
direct tumor killing but also serve to modulate immune networks to
induce local and/or systemic immune responses to tumors, capable of
counteracting tumor-induced suppression by TGF-β, IL-4, and IL-10
(28,29). Flow cytometry results provided
evidence that HER2Bi-armed ATCs expressed higher level of CD69 than
the unarmed-ATC counterparts. CD69 represents a marker of early
T-cell activation and acts as a costimulatory molecule that
increased T-cell responses following TCR-ligand interaction
(30). Therefore, IFN-γ produced
by HER2Bi-armed ATC upon its binding to tumor antigen may be
clinically beneficial. HER2Bi-Ab did not bind to
CD3−HER2−-K562 cells, confirming the
specificity of the HER2Bi-Ab.
In tumor growth delay studies, HER2Bi-armed ATCs
prevented and furthermore significantly inhibited tumor growth in
mice bearing established HER2-positive Colo205 xenografts, whereas
control unarmed ATCs did not, confirming the specificity of the
targets. Similarly, in a pilot study, HER2Bi-armed ATCs injected
intratumorally induced remission of human hormone-refractory
prostate tumor in severe combined immunodeficient mice (31). Conceivably, the binding of the
effector cells at the tumor site by armed ATCs may not only augment
tumoricidal activity but also increase local cytokine secretion
leading to the recruitment of other immune effectors (32,33).
Although clinical studies have shown that
Herceptin® significantly improves the overall survival
of breast cancer patients, an unforeseen significant side-effect of
cardiotoxicity manifested as left ventricular dysfunction and heart
failure (34). In our study,
HER2Bi-armed ATCs were highly effective in eliminating tumor cells
both in vitro and in vivo at very low concentration
of HER2-Bi-Ab. Also, our studies showed Herceptin®
failed to inhibit proliferation of colon carcinoma cells in
vitro, partly because of the HER2 expression on colon carcinoma
cell lines were barely middle or low compared with the HER2
overexpressing breast cancer cell line SKBR3 (35). Therefore, more importantly, our
study provided a new strategy for treatment of colon cancer in the
event when the expression of the target tumor antigen e.g., HER2,
is not high.
In conclusion, taken together with the in
vitro cytotoxicity and cytokine secretion studies, the ability
of HER2Bi-armed ATCs to prevent the development and suppress the
growth of tumors in xenograft mice suggests that HER2Bi-armed ATCs
could be used as a good strategy for the treatment of
HER+ CRC patient and produce clinically significant
antitumor effects.
Acknowledgements
This study was funded by the grants from the Basic
Research Program of China (973 Program, No. 2013CB531502), the
Ministry of Science and Technology of China (S&T major Program:
No. 2012ZX1004701-001-002), and the National Nature Science
Foundation of China (No. 31370889 and 31170829).
Abbreviations:
|
CRC
|
colorectal cancer
|
|
ATCs
|
activated T cells
|
|
VEGF
|
vascular endothelial growth factor
|
|
EGFR
|
epidermal growth factor receptor
|
|
HER2Bi-Ab
|
anti-CD3 x anti-HER2 bispecific
antibody
|
|
PBMCs
|
peripheral mononuclear blood cells
|
|
ANOVA
|
one-way analysis of variance
|
|
TAA
|
tumor-associated antigen
|
References
|
1
|
Jochems C and Schlom J: Tumor-infiltrating
immune cells and prognosis: the potential link between conventional
cancer therapy and immunity. Exp Biol Med (Maywood). 236:567–579.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Xiang J, Pan Z, Attah-Poku S, Babiuk L,
Zhang Y and Liu E: Production of hybrid bispecific antibody
recognizing human colorectal carcinoma and CD3 antigen. Mol
Biother. 4:15–23. 1992.PubMed/NCBI
|
|
3
|
Gautherot E, Rouvier E, Daniel L, Loucif
E, Bouhou J, Manetti C, Martin M, Le Doussal JM and Barbet J:
Pretargeted radioimmunotherapy of human colorectal xenografts with
bispecific antibody and 131I-labeled bivalent hapten. J Nucl Med.
41:480–487. 2000.PubMed/NCBI
|
|
4
|
Herrmann I, Baeuerle PA, Friedrich M, Murr
A, Filusch S, Rüttinger D, Majdoub MW, Sharma S, Kufer P, Raum T
and Münz M: Highly efficient elimination of colorectal
tumor-initiating cells by an EpCAM/CD3-bispecific antibody engaging
human T cells. PLoS One. 5:e134742010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kim DD and Eng C: The promise of mTOR
inhibitors in the treatment of colorectal cancer. Expert Opin
Investig Drugs. 21:1775–1788. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Misale S, Yaeger R, Hobor S, Scala E,
Janakiraman M, Liska D, Valtorta E, Schiavo R, Buscarino M,
Siravegna G, et al: Emergence of KRAS mutations and acquired
resistance to anti-EGFR therapy in colorectal cancer. Nature.
486:532–536. 2012.PubMed/NCBI
|
|
7
|
Tol J and Punt CJ: Monoclonal antibodies
in the treatment of metastatic colorectal cancer: a review. Clin
Ther. 32:437–453. 2010. View Article : Google Scholar
|
|
8
|
Wang ZH, Gao QY and Fang JY: Loss of PTEN
expression as a predictor of resistance to anti-EGFR monoclonal
therapy in metastatic colorectal cancer: evidence from
retrospective studies. Cancer Chemother Pharmacol. 69:1647–1655.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ross JS, Slodkowska EA, Symmans WF,
Pusztai L, Ravdin PM and Hortobagyi GN: The HER-2 receptor and
breast cancer: ten years of targeted anti-HER-2 therapy and
personalized medicine. Oncologist. 14:320–368. 2009.PubMed/NCBI
|
|
10
|
Hillig T, Thode J, Breinholt MF, Franzmann
MB, Pedersen C, Lund F, Mygind H, Sölétormos G and Rudnicki M:
Assessing HER2 amplification by IHC, FISH, and real-time polymerase
chain reaction analysis (real-time PCR) following LCM in
formalin-fixed paraffin embedded tissue from 40 women with ovarian
cancer. APMIS. 120:1000–1007. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Janjigian YY, Werner D, Pauligk C,
Steinmetz K, Kelsen DP, Jäger E, Altmannsberger HM, Robinson E,
Tafe LJ, Tang LH, Shah MA and Al-Batran SE: Prognosis of metastatic
gastric and gastroesophageal junction cancer by HER2 status: a
European and USA International collaborative analysis. Ann Oncol.
23:2656–2662. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jørgensen JT and Hersom M: HER2 as a
prognostic marker in gastric cancer-a systematic analysis of data
from the literature. J Cancer. 3:137–144. 2012.PubMed/NCBI
|
|
13
|
Takenaka M, Hanagiri T, Shinohara S,
Kuwata T, Chikaishi Y, Oka S, Shigematsu Y, Nagata Y, Shimokawa H,
Nakagawa M, Uramoto H, So T and Tanaka F: The prognostic
significance of HER2 overexpression in non-small cell lung cancer.
Anticancer Res. 31:4631–4636. 2011.PubMed/NCBI
|
|
14
|
Bergmann F, Moldenhauer G, Herpel E, Gaida
MM, Strobel O, Werner J, Esposito I, Müerköster SS, Schirmacher P
and Kern MA: Expression of L1CAM, COX-2, EGFR, c-KIT and Her2/neu
in anaplastic pancreatic cancer: putative therapeutic targets?
Histopathology. 56:440–448. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Krähn G, Leiter U, Kaskel P, Udart M,
Utikal J, Bezold G and Peter RU: Coexpression patterns of EGFR,
HER2, HER3 and HER4 in non-melanoma skin cancer. Eur J Cancer.
37:251–259. 2001.PubMed/NCBI
|
|
16
|
Schuell B, Gruenberger T, Scheithauer W,
Zielinski Ch and Wrba F: HER 2/neu protein expression in colorectal
cancer. BMC Cancer. 6:1232006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kountourakis P, Pavlakis K, Psyrri A,
Rontogianni D, Xiros N, Patsouris E, Pectasides D and Economopoulos
T: Clinicopathologic significance of EGFR and Her-2/neu in
colorectal adenocarcinomas. Cancer J. 12:229–236. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kavanagh DO, Chambers G, O’Grady L, Barry
KM, Waldron RP, Bennani F, Eustace PW and Tobbia I: Is
overexpression of HER-2 a predictor of prognosis in colorectal
cancer? BMC Cancer. 9:12009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mann M, Sheng H, Shao J, Williams CS,
Pisacane PI, Sliwkowski MX and DuBois RN: Targeting cyclooxygenase
2 and HER-2/neu pathways inhibits colorectal carcinoma growth.
Gastroenterology. 120:1713–1719. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Fury MG, Lipton A, Smith KM, Winston CB
and Pfister DG: A phase-I trial of the epidermal growth factor
receptor directed bispecific antibody MDX-447 without and with
recombinant human granulocyte-colony stimulating factor in patients
with advanced solid tumors. Cancer Immunol Immunother. 57:155–163.
2008. View Article : Google Scholar
|
|
21
|
Seimetz D, Lindhofer H and Bokemeyer C:
Development and approval of the trifunctional antibody catumaxomab
(anti-EpCAM x anti-CD3) as a targeted cancer immunotherapy. Cancer
Treat Rev. 36:458–467. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Clay TM, Custer MC, Sachs J, Hwu P,
Rosenberg SA and Nishimura MI: Efficient transfer of a tumor
antigen-reactive TCR to human peripheral blood lymphocytes confers
anti-tumor reactivity. J Immunol. 163:507–513. 1999.PubMed/NCBI
|
|
23
|
Ma J, Han H, Liu D, Li W, Feng H, Xue X,
Wu X, Niu G, Zhang G, Zhao Y, Liu C, Tao H and Gao B: HER2 as a
promising target for cytotoxicity T cells in human melanoma
therapy. PLoS One. 8:e732612013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Fu X, Tao L, Rivera A, Williamson S, Song
XT, Ahmed N and Zhang X: Simple and sensitive method for measuring
tumor-specific T cell cytotoxicity. PLoS One. 5:e118672010.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Brown CE, Wright CL, Naranjo A, Vishwanath
RP, Chang WC, Olivares S, Wagner JR, Bruins L, Raubitschek A,
Cooper LJ and Jensen MC: Biophotonic cytotoxicity assay for
high-throughput screening of cytolytic killing. J Immunol Methods.
297:39–52. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Repp R, van Ojik HH, Valerius T,
Groenewegen G, Wieland G, Oetzel C, Stockmeyer B, Becker W,
Eisenhut M, Steininger H, et al: Phase I clinical trial of the
bispecific antibody MDX-H210 (anti-FcgammaRI x anti-HER-2/neu) in
combination with Filgrastim (G-CSF) for treatment of advanced
breast cancer. Br J Cancer. 89:2234–2243. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lum LG, Rathore R, Cummings F, Colvin GA,
Radie-Keane K, Maizel A, Quesenberry PJ and Elfenbein GJ: Phase
I/II study of treatment of stage IV breast cancer with OKT3 x
trastuzumab-armed activated T cells. Clin Breast Cancer. 4:212–217.
2003.PubMed/NCBI
|
|
28
|
Sheu BC, Lin RH, Lien HC, Ho HN, Hsu SM
and Huang SC: Predominant Th2/Tc2 polarity of tumor-infiltrating
lymphocytes in human cervical cancer. J Immunol. 167:2972–2978.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Chen ML, Pittet MJ, Gorelik L, Flavell RA,
Weissleder R, von Boehmer H and Khazaie K: Regulatory T cells
suppress tumor-specific CD8 T cell cytotoxicity through TGF-beta
signals in vivo. Proc Natl Acad Sci USA. 102:419–424. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sathaliyawala T, Kubota M, Yudanin N,
Turner D, Camp P, Thome JJ, Bickham KL, Lerner H, Goldstein M,
Sykes M, Kato T and Farber DL: Distribution and
compartmentalization of human circulating and tissue-resident
memory T cell subsets. Immunity. 38:187–197. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Davol PA, Smith JA, Kouttab N, Elfenbein
GJ and Lum LG: Anti-CD3 x anti-HER2 bispecific antibody effectively
redirects armed T cells to inhibit tumor development and growth in
hormone-refractory prostate cancer-bearing severe combined
immunodeficient beige mice. Clin Prostate Cancer. 3:112–121. 2004.
View Article : Google Scholar
|
|
32
|
Karamouzis MV, Konstantinopoulos PA and
Papavassiliou AG: Trastuzumab-mechanism of action and use. N Engl J
Med. 357:16642007. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zitron IM, Thakur A, Norkina O, Barger GR,
Lum LG and Mittal S: Targeting and killing of glioblastoma with
activated T cells armed with bispecific antibodies. BMC Cancer.
13:832013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Baban T, Blomberg C, Hoffner E and Yan X:
Anti-HER2 cancer therapy and cardiotoxicity. Curr Pharm Des. June
4–2014.(Epub ahead of print).
|
|
35
|
Wang L, He Y, Zhang G, Ma J, Liu C, He W,
Wang W, Han H, Boruah BM and Gao B: Retargeting T cells for
HER2-positive tumor killing by a bispecific Fv-Fc antibody. PLoS
One. 8:e755892013. View Article : Google Scholar : PubMed/NCBI
|