Introduction
Myoepithelial carcinoma (MC) is defined as a
malignant salivary neoplasm composed almost exclusively of tumor
cells with myoepithelial differentiation (1). MC was first described by Stromeyer
et al in 1975, and was included in the World Health
Organization (WHO) classification of salivary gland neoplasms as a
distinct clinicopathological entity, in 1991. MC is rare,
accounting for ∼0.4–0.6% of the salivary gland tumors and 1.2–1.5%
of carcinomas, as noted in a recent large series (2). It arises predominantly from the
parotid glands, while other carcinomas occur in the submandibular
or the accessory glands of the oral cavity. Such carcinomas may
arise from the glands of the respiratory tract (3). However, primary MC of the bone is
extremely rare. In the present study, a case of MC originating from
the maxilla bone showing extremely high malignancy was examined.
This study was approved by the Ethics Committee of Sichuan
University, Chengdu, China. Informed consent was obtained from the
patient.
Case report
A 41-year-old, previously healthy woman was referred
to the Department of Stomatology, West China Hospital (Chengdu,
China) due to dysfunction of chewing in the left superior incisor.
During clinical examination, a cystic opacity was observed in the
left superior section of the maxilla, with a clear smooth boundary
and sharp edge. Dental status in other sections of the maxilla was
normal. The patient was first diagnosed with a bone cyst of the
left maxilla, and received local surgical excision in October,
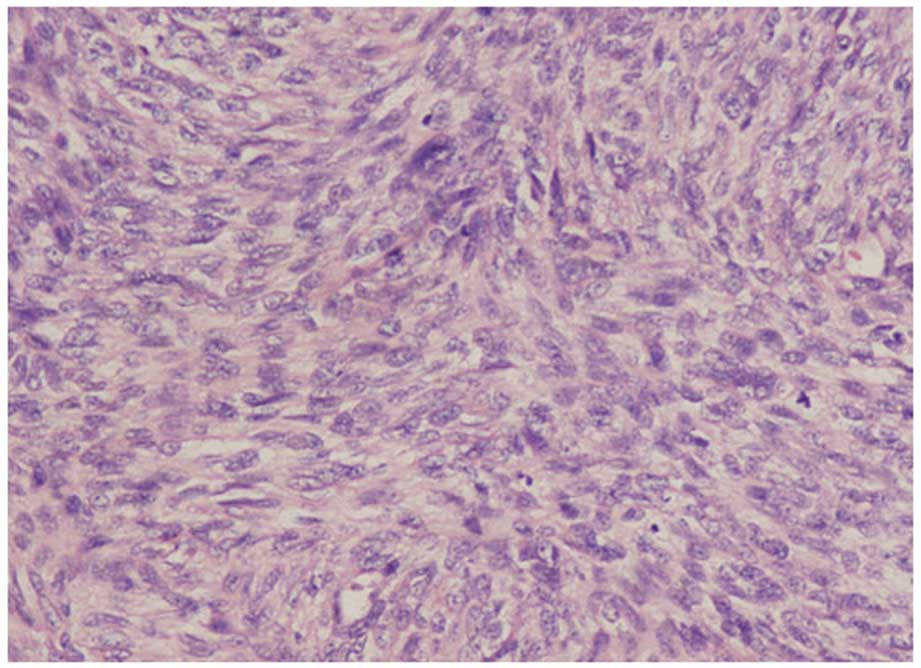
2007. The post-operative biopsy showed massive muscular spindle
cells in combination with small epithelial and plasmacytoid cells.
The matrix was mainly myxoid (Fig.
1). The immunohistochemical examination detected the cyst as CK
(+); GFAP (+); α-SMA (+++); CD10 (−); S-100 (−); and Ki-67, 10%.
The final diagnosis was myoepithelial carcinoma. The patient was
then treated with three-dimensional conformal radiotherapy at a
dosage of 7000 cGy 30 times, immediately after surgery. However,
the patient was suffering from constant, extreme pain in the
buttocks 7 months later.
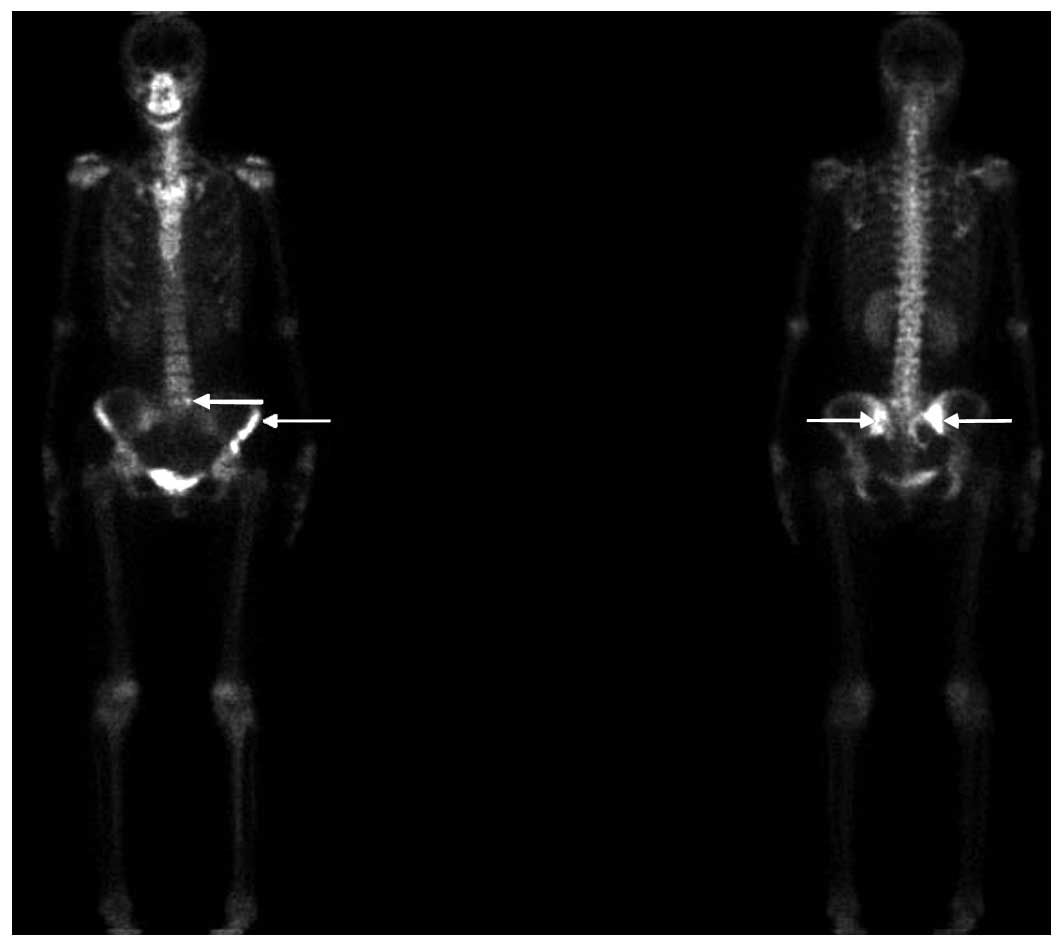
Subsequent to computed tomography (CT) and bone scan
examinations showed metastases to the first sacral vertebra, right
sacroiliac joint as well as the left anteroinferior iliac spine
(Fig. 2). The patient then
received radiotherapy for the metastasis at a dosage of 5000 cGy 25
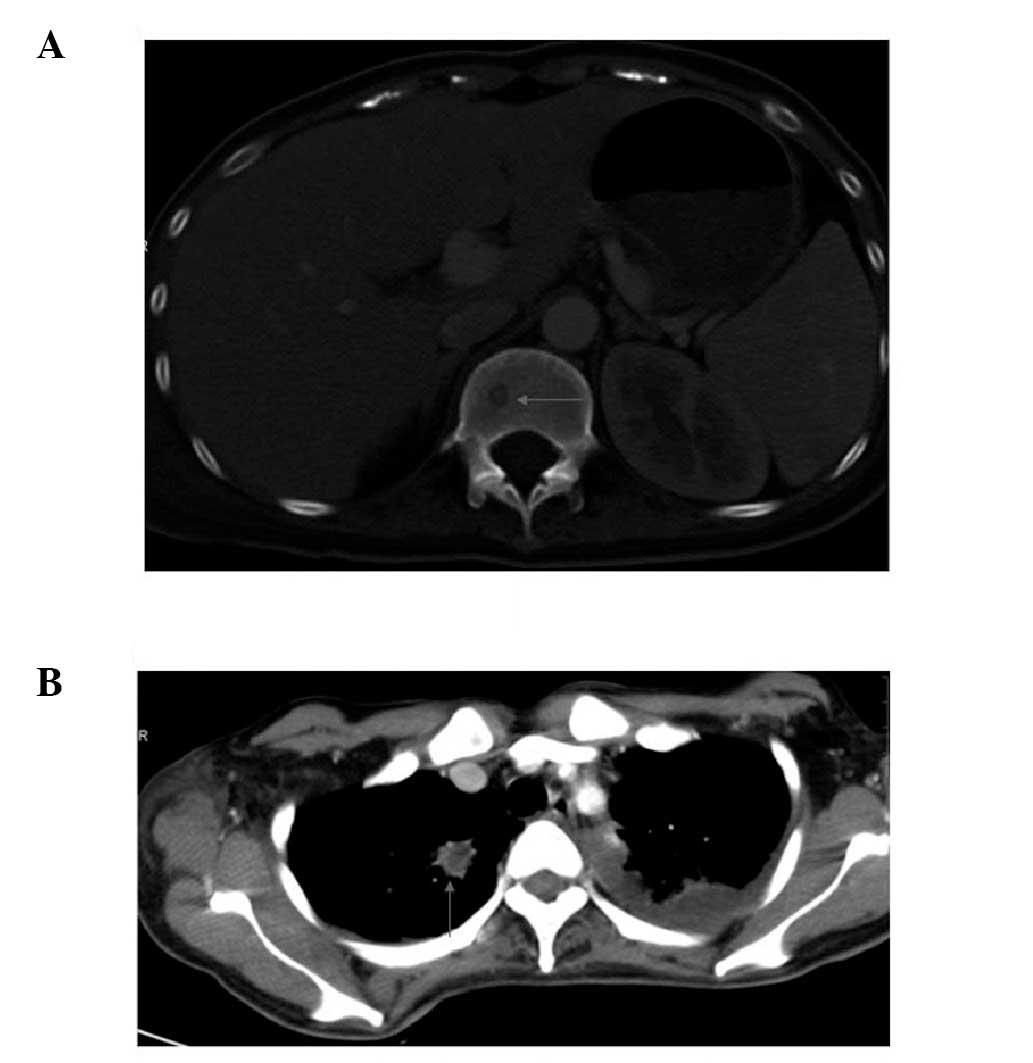
times, as well as chemotherapy. The post-treatment CT examination
showed progression of the metastasis to the iliac bone.
Additionally, certain thoracic and lumber vertebras had also been
invaded (Fig. 3A). Several days
later, the patient had a pathological bone fracture in the right
femoral bone. The patient received chemotherapy a number of times,
with several schemes, such as IFO+EPI+DPP, IFO+EPI and
paclitaxel+DTIC. However, the progression of cancer could not be
controlled. During the upcoming months, the patient presented with
paralysis of the right leg, disability of the iliac joints,
repeated episodes of high fever, extreme pain, as well as urinary
frequency and tenderness. On January 29, 2009, the patient was
diagnosed with lung metastasis by CT (Fig. 3B), succumbing to the disease 1
month later.
Discussion
The diagnosis of MC is based on two main histologic
criteria: unequivocal malignancy and an exclusively myoepithelial
nature. The malignancy is supported by the infiltrative growth, the
necrotic areas and the cellular pleomorphism in the neoplasm. The
myoepithelial nature is suggested by the cytological
differentiation of the tumor cells towards myoepithelial elements
and the lack of ductal or acinar differentiation (1). The pathological and
immunohistochemical examination and clinical process of our patient
confirmed the diagnosis of MC.
MC is an extremely rare type of cancer. It is mainly
found in the salivary gland, especially the parotid gland. Although
certain cases of the maxillary sinus and hard palate have been
reported (3–5), those cases originated from the minor
salivary gland on the surface of these bones. The MC of bones in
other sites were metastases (6).
In the present study, a case of MC located in the left superior
part of the maxilla was reported. The MC was extensively treated in
our hospital and showed extremely high malignancy and bad
prognosis.
The pathogenesis of MC in the bone was unclear,
likely because of the presence of residual epithelium in the
maxilla bone during the embryonic period. However, in most of these
situations, a bone cyst is formed. However, no MC originating from
the epithelium within the bone has yet been reported.
The biological behavior and prognosis of MC are not
likely to be due to its rarity only. Generally, most MCs showed a
low-grade malignancy, although certain reports of MC showed a
high-grade malignancy and bad prognosis (2,7,8). As
far as the treatment of MC is concerned, experience is limited,
with complete surgical excision being mainstay of therapy (8). The role of chemotherapy or
radiotherapy in the treatment of MC was unclear (9,10).
In this report, the MC of our patient showed an extremely high
grade of malignancy. Local surgical excision was performed due to
the misdiagnosis as a bone cyst. The patient had distant metastases
subsequently, despite the post-operative chemoradiation treatment.
Moreover, the disease progressed during the chemoradiation
treatment of metastases. These results showed that MC may be
extremely malignant. Chemoradiation treatment had limited effect on
the treatment of MC, and complete surgical excision was highly
important.
In conclusion, in the present study an extremely
rare case of MC within the maxilla bone was reported. Following
misdiagnosis as a bone cyst, local excision was performed. The
patient then presented with an extremely high malignancy and showed
no response to chemoradiation treatment. The bone cyst of the oral
cavity was likely to be MC, thus early diagnosis with complete
surgical excision was extremely important. After confirmation of
MC, a secondary extensive surgery may be of great importance,
following the primary local surgical resection.
References
|
1
|
Suba Z, Nemeth Z, Gyulai-Gaal S, Ujpal M,
Szende B and Szabo G: Malignant myoepithelioma. Clinicopathological
and immunohistochemical characteristics. Int J Oral Maxillofac
Surg. 32:339–341. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yang S, Li L, Zeng M, Zhu X, Zhang J and
Chen X: Myoepithelial carcinoma of intraoral minor salivary glands:
a clinicopathological study of 7 cases and review of the
literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
110:85–93. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ren J, Liu Z, Liu X, Li Y, Zhang X, Li Z,
Yang Y, Chen Y and Jiang S: Primary myoepithelial carcinoma of
palate. World J Surg Oncol. 9:1042011. View Article : Google Scholar
|
|
4
|
Zhou SH, Ruan LX, Gong L and Wang SQ:
Primary malignant myoepithelioma of the left maxillary sinus: a
case report. J Int Med Res. 36:362–365. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hata M, Tokuuye K, Shioyama Y, Nomoto S,
Inadome Y, Fukumitsu N, Nakayama H, Sugahara S, Ohara K, Noguchi M
and Akine Y: Malignant myoepithelioma in the maxillary sinus: case
report and review of the literature. Anticancer Res. 29:497–501.
2009.PubMed/NCBI
|
|
6
|
Bohnstedt BN, Tomcik M, Eads T, Hagen MC
and Shah M: Metastasis of soft-tissue myoepithelial carcinoma to
clivus. J Neurosurg Pediatr. 9:161–164. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Savera AT, Sloman A, Huvos AG and Klimstra
DS: Myoepithelial carcinoma of the salivary glands: a
clinicopathologic study of 25 patients. Am J Surg Pathol.
24:761–774. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kane SV and Bagwan IN: Myoepithelial
carcinoma of the salivary glands: a clinicopathologic study of 51
cases in a tertiary cancer center. Arch Otolaryngol Head Neck Surg.
136:702–712. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kyriazi MA, Carvounis EE, Kitsou M,
Arkadopoulos N, Nicolaidou E, Fotiou S and Smyrniotis V:
Myoepithelial carcinoma of the vulva mimicking bartholin gland
abscess in a pregnant woman: case report and review of literature.
Int J Gynecol Pathol. 29:501–504. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Miyata M, Hasegawa K, Ishikawa K, Kato R,
Udagawa Y and Kuroda M: Primary myoepithelial carcinoma of the
vulva and review of the literature. J Obstet Gynaecol Res.
37:617–622. 2011. View Article : Google Scholar : PubMed/NCBI
|