Introduction
As chemotherapy is used in adjuvant settings,
anthracyclins and taxanes are included in standard regimens due to
abundant evidence from several clinical trials over the past
decades demonstrating a significant reduction in the risk of
relapse or mortality of the disease (1–4). By
contrast, there is no standard regimen recommended in metastatic
settings. In most of the clinical trials for metastatic breast
cancer (MBC), the efficacy of chemotherapeutic agents used as the
first or second line of treatment for MBC was investigated
(5–8). Anthracyclins have shown favorable
activity that accounted for 30–50% of objective response rates
(ORR) and ≥12 months of overall survival (OS) when administered in
the first-line regimen for MBC (6,7).
Taxanes have shown efficacy consistent with that of anthracyclins
in this setting (9–11). However, in the second or later line
of treatment, many patients with MBC have already been treated with
anthracyclins and taxanes in either adjuvant/neoadjuvant or
metastatic settings. In these cases, alternative options should be
considered. Results of clinical trials testing the efficacy and
safety of vinorelbine, gemcitabine, TS-1, ixabepilone or
capecitabine as treatment for MBC have been reported (9–20).
Since these agents showed modest efficacy when administered alone,
they have been recommended in combination with other cytotoxic
agents. Taxanes were shown to have more benefit when used in
combination with capecitabine, vinorelbine or gemcitabine compared
with taxane monotherapy (21–25).
Notably, although clinical trials assessing the efficacy of these
agents, besides anthracyclins and taxanes, administered as
monotherapy have shown an ORR of 0–20% and progression-free
survival (PFS) of 2–5 months, these agents were expected to have
favorable toxicity and survival of 8–12 months (9–20).
Therefore, for palliative care, less toxic anticancer agents such
as capecitabine, vinorelbine and gemcitabine are often recommended
to be administered alone sequentially at the third or later line of
treatment for MBC rather than administered concurrently (26).
Although the aim of treatment for MBC is control of
the disease and disease-related symptoms, progression-free or
disease-free long-term survival is often achieved by chemotherapy
in patients with MBC. In these cases, the factors involved in
clinical responses to the regimens used remain to be determined. In
this study, we focused on time to treatment failure (TTF) as a
parameter to compare clinical outcomes of the treated patients
since prolonged TTF is thought to be correlated with long-term
treatment with one therapeutic regimen, long time to progression
(TTP) or OS with stable cancer status and good quality of life in
treated patients. TTF is determined predominantly by a number of
parameters that are predictable prior to treatment. Such parameters
include regimen-related adverse events that are predictable in
advance, patient agreement and physical and mental status, as well
as the physician’s confidence in the regimen and tumor responses to
regimens that are unpredictable. In contrast to TTF, TTP, duration
of response and OS are not predictable prior to treatment. Since
TTF is the only parameter predictable in many cases prior to
treatment and since TTF is closely correlated with the duration of
treatment with one therapeutic regimen and survival, chemotherapy
regimens that are expected to prolong TTF may be selected at the
physician’s discretion with consideration of patient status and
prior chemotherapeutic regimens.
Metronomic chemotherapy is defined as continuous or
frequent treatment of low doses of anticancer agents and is usually
used as palliative care in patients who have been heavily
pre-treated with cytotoxic drugs or who have poor performance
status (PS) (27). Of note,
metronomic chemotherapy used for palliation has been reported to
result in favorable tumor responses and prolonged survival
(28–30). The aim of this study was to
determine whether prolonged TTF is correlated with a favorable
clinical outcome and to determine which variable is responsible for
the prolongation of TTF by comparing the clinicopathological
characteristics and clinical outcomes between patients with MBC who
showed TTF ≥12 months and those who showed TTF <12 months. The
clinical efficacy of metronomic regimens and that of non-metronomic
regimens was also compared.
Patients and methods
Patients
In total, 55 patients with advanced or recurrent
breast cancer who were treated with chemotherapeutic regimens at
the Kagawa University Hospital between April, 2005 and December,
2011, were retrospectively analyzed for their clinico pathological
characteristics and clinical outcomes. Mean age and number of
pre-treated chemotherapeutic regimens for MBC of the patients were
58.11 (32 of 81) and 1.76 (0 of 4), respectively. Clinical outcomes
examined in this study included TTF, defined as the duration from
the initiation to the discontinuation of treatment; TTP, defined as
the duration from initiation of treatment to disease progression or
death from any cause; OS, defined as the duration from initiation
of treatment to death from any cause; and ORR.
The patients were allocated the TTF ≥12 months and
TTF <12 months groups. Clinicopathological characteristics and
outcomes were compared in the two groups (Table I).
 | Table IClinicopathological characteristics of
patients with MBC. |
Table I
Clinicopathological characteristics of
patients with MBC.
| Characteristics | TTF ≥12 months | TTF <12
months | P-value |
|---|
| No. of patients | 26 | 29 | |
| Age (years) | 60.2±12.3 | 56.3±12.6 | 0.125 |
| DFI (months) | 62.2±50.4 | 59.3±53.5 | 0.19 |
| Line of CT for
MBC | 2.2±1.31 | 1.3±0.67 | 0.003 |
| Prior adjuvant CT
(%) | 61.1 | 78.9 | 0.242 |
| No. of metastatic
sites | 1.9±0.86 | 1.9±1.11 | 0.96 |
| IDC (%) | 94.1 | 100 | 0.395 |
| Tumor grade | 1.8±0.79 | 2.6±0.67 | 0.018 |
| HR-positive (%) | 73.1 | 37.9 | 0.0096 |
| HER2-overexpressed
(%) | 34.8 | 17.9 | 0.172 |
| Triple negative
(%) | 16 | 48.3 | 0.0129 |
| Metronomic CT
(%) | 80.8 | 24.1 | 0.00003 |
Evaluation of therapeutic efficacy
Tumor responses were assessed by physical
examination and computed tomography or magnetic resonance imaging,
based on the Response Evaluation Criteria in Solid Tumors every 2–3
months during treatment and every 6 months following treatment.
Complete response was defined as the absence of evidence of the
disease, partial response was defined as a reduction in the product
of the two largest perpendicular diameters of the target lesions by
<50%, and progressive disease was defined as an increase in
tumor size by <25% or presence of a new lesion.
Statistical analysis
The Mann-Whitney U test or standard Chi-square
procedures were used for comparison of the two groups. The effect
of baseline characteristics, clinical responses or prognostic
parameters on the risk of progression or death was calculated using
the Kaplan-Meier method and the log-rank test of significance. A
95% confidence interval for the median of each variable was
computed using the Brookmeyer and Crowley method. P<0.05 was
considered to indicate a statistically significant difference.
P-values were two-sided. The SPSS statistical software system (SPSS
Inc., Tokyo, Japan) was used for the calculations.
Ethical consideration
This study was in compliance with the guidelines of
the Ethics Committee of the Kagawa University Hospital and
conformed to the provisions of the Declaration of Helsinki, 1995.
Informed consent was obtained from all patients involved in the
study.
Results
Comparison of clinicopathological
characteristics and outcome between patients with TTF ≥12 M and
patients with TTF <12 M
There were 26 patients TTF ≥12 months and 29
patients with TTF <12 months (Table
I). Clinicopathological characteristics including age,
disease-free interval defined as the interval from surgery for
primary lesions to the diagnosis of cancer recurrence, number of
prior chemotherapy regimens for MBC, number of prior adjuvant
chemotherapy regimens, number of metastatic sites, histologic
types, tumor grade, hormone and HER2 status, as well as metronomic
chemotherapy were compared in the two groups. Tumor grade and the
proportion of triple negative cancers were significantly higher in
the TTF <12 months group compared to the TTF ≥12 months group.
The proportion of hormone-sensitive breast cancers and the number
of prior chemotherapy regimens for MBC were significantly higher in
the TTF ≥12 months group compared to the TTF <12 months group.
Of note, the proportion of patients who received metronomic
chemotherapy was significantly higher in the TTF ≥12 months group
compared to the TTF <12 months group (80.8 vs. 24.1%,
P=0.00003).
Metronomic thermotherapy used in this study included
capecitabine or TS-1 alone or in combination with oral
cyclophosphamide and/or trastuzumab, which was used only for
HER2-overexpressed cancer, or oral cyclophosphamide alone (data not
shown). The metronomic chemotherapeutic regimens also included
bisphosphonates or endocrine agents in certain cases with bone
lesions or hormone-responsive cancer, respectively. Non-metronomic
chemotherapy included paclitaxel, docetaxel or vinorelbine alone or
in combination with capecitabine and/or trastuzumab, which was used
only for HER2-overexpressed cancer, or anthracyclin-based regimens
comprising cyclophosphamide, epirubucin and 5-fluorouracil. The
non-metronomic therapeutic regimens included bisphosphonates in
cases with bone lesions.
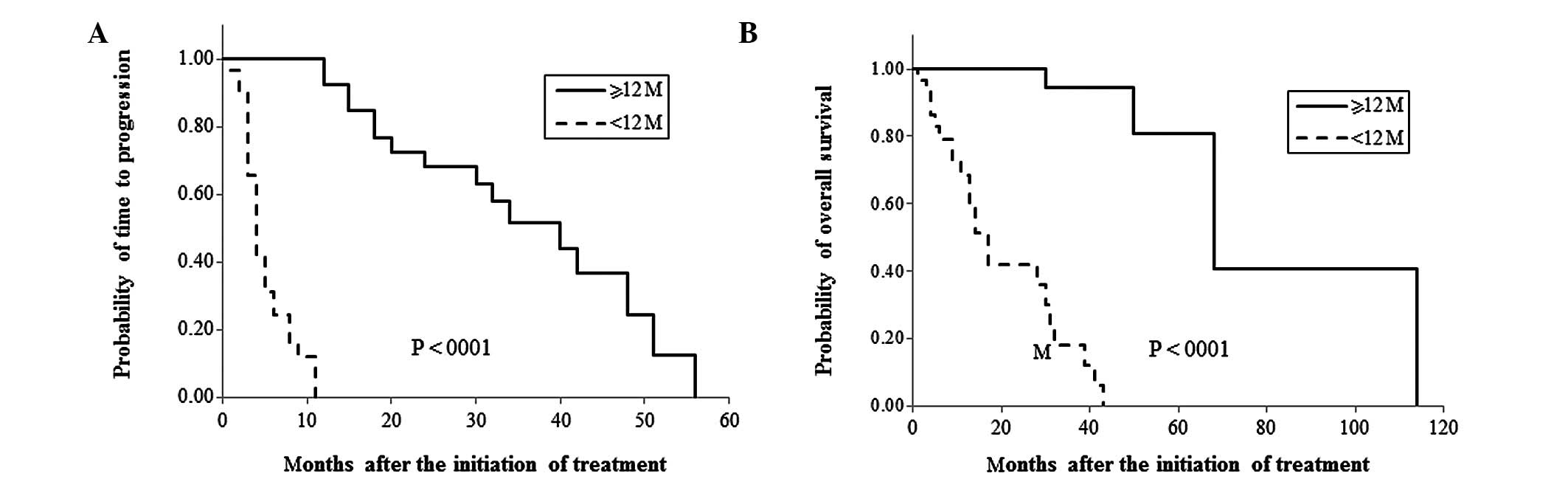
When clinical outcomes were compared in the two
groups, ORR was significantly higher in the TTF ≥12 months group
compared to the TTF <12 months group (69.2 vs. 25%, P=0.0009,
Table II). Furthermore, patients
in the TTF ≥12 months group showed significantly longer median TTP
and OS compared to patients in the TTF <12 months group (TTP: 40
vs. 4 months, P<0.0001; OS: 68 vs. 17 months, P<0.0001,
Table II and Fig. 1).
| Table IIComparison of clinical outcomes in
patients with TTF of ≥12 months or <12 months. |
Table II
Comparison of clinical outcomes in
patients with TTF of ≥12 months or <12 months.
| Clinical
outcomes | TTF ≥12 months | TTF <12
months | P-value |
|---|
| ORR (%) | 69.2 | 25 | 0.0009 |
| Median TTP
(months) | 40.0 | 4 | <0.0001 |
| Median OS | 68.0 | 17 | <0.0001 |
Comparison of clinical outcomes in
patients receiving metronomic regimens and patients receiving
non-metronomic regimens
As described above, there was a statistically
significant difference between the proportion of patients who
received metronomic chemotherapy in the TTF ≥12 months group and
TTF <12 months groups. The 29 patients who received metronomic
regimens included 11 patients who had been heavily pre-treated, 9
patients who requested the regimen including 5 patients who were
reluctant to experience hair loss, 7 patients who were elderly or
had poor PS and 2 patients who had mental or psychiatric conditions
(Table III). Clinical outcomes in
patients receiving metronomic regimens and those receiving
non-metronomic regimens were compared, since only the
chemotherapeutic regimens listed in Table I could be selected by physicians
prior to treatment. As shown in Table
IV, none of the clinicopathological characteristics, with the
exception of age, varied in the two groups. Mean age in the
metronomic group was significantly higher compared to the
non-metronomic group (63.75 vs. 52.26 years, P=0004). Patients in
the metronomic group showed a trend to receive more prior
chemotherapy for MBC compared to patients in the non-metronomic
group, although there was no statistically significant difference
(P=0.056) (Table IV). The results
suggested that metronomic regimens were indicated for elderly
patients or patients who had been heavily pre-treated with
chemotherapy. Median TTF, TTP and OS were significantly longer in
the metronomic compared to the non-metronomic group (TTF: 18 vs. 4
months, P=0.00003; TTP: 30 vs. 4 months, P=0.0017; OS: 68 vs. 28
months, P=0.0005, Table V).
Furthermore, 75% of the patients who received metronomic regimens
had ≥12 months TTF, while only 18.5% of the patients who received
non-metronomic regimens had ≥12 months TTF (Table V). By contrast, no statistically
significant difference was detected in ORR in the two groups.
| Table IIIReasons for selecting metronomic
chemotherapy. |
Table III
Reasons for selecting metronomic
chemotherapy.
| Reasons | No. of patients |
|---|
| Heavy
pretreatment | 11 |
| Patients’ choice | 9 |
| Elderly or poor
PS | 7 |
| Mental problem | 2 |
| Total | 29 |
| Table IVComparison of clinicopathologic
features in patients receiving metronomic regimens and those
receiving non-metronomic regimens. |
Table IV
Comparison of clinicopathologic
features in patients receiving metronomic regimens and those
receiving non-metronomic regimens.
| Characteristics | Metronomic | Non-metronomic | P-value |
|---|
| No. of
patients | 28 | 27 | |
| Age (years) | 63.75±11.53 | 52.26±10.80 | 0.0004 |
| DFI (months) | 49.20±48.51 | 50.59±58.70 | 0.939 |
| No. of prior CT for
MBC | 2.03±1.20 | 1.46±0.95 | 0.056 |
| Prior adjuvant CT
(%) | 60 | 82.4 | 0.144 |
| Tumor grade | 2.14±0.86 | 2.43±0.78 | 0.461 |
| No. of metastatic
sites | 1.71±0.81 | 2.07±1.14 | 0.185 |
| Hormone receptor
(%) | 59.3 | 48.1 | 0.417 |
| HER2-overexpressed
(%) | 32 | 20 | 0.3 |
| Triple negative
(%) | 25.9 | 40.7 | 0.253 |
| Table VComparison of clinical outcomes in
patients receiving metronomic regimens and those receiving
non-metronomic regimens. |
Table V
Comparison of clinical outcomes in
patients receiving metronomic regimens and those receiving
non-metronomic regimens.
| Outcomes | Metronomic | Non-metronomic | P-value |
|---|
| ORR (%) | 50 | 42.3 | 0.575 |
| Median TTF
(months) | 18 | 4.0 | 0.00003 |
| TTF ≥12 months
(%) | 75 | 18.5 | <0.00001 |
| Median TTP | 30 | 4.0 | 0.0017 |
| Median OS | 68 | 28.0 | 0.0005 |
Discussion
In this study, we retrospectively compared clinical
outcomes in patients with MBC who had a long TTF (≥12 months) and
those who had a short TTF (<12 months) to determine the factors
predicting prognosis of patients with MBC who have received
chemotherapy. The reason for selecting TTF for the comparison is
that prolongation of the duration of one regimen is the most
crucial characteristic for achieving long survival with minimized
toxicity in treated patients. TTF is determined by tumor responses
to the regimen used as well as by regimen-related adverse events,
the patient’s condition and agreement and the physician’s
confidence in the regimen for treatment of MBC. While tumor
responses are unpredictable prior to treatment, possible
regimen-related adverse events are predictable in several cases.
Furthermore, using regimens that have abundant evidence concerning
their efficacy and safety may be more readily accepted by patients
and physicians. Thus, we thought that it is crucial to attempt to
prolong the duration of one regimen, minimizing adverse events and
maintaining satisfaction for both patients and physicians. Since
ORR does not appear to correlate with survival, and TTP and OS are
unpredictable prior to treatment, these parameters cannot be used
for the predefined aim of treatment for MBC when selecting regimens
(10,31,32).
Furthermore, a difference in OS has not been observed in several
clinical trials comparing the efficacy of chemotherapeutic
regimens.
For first-line chemotherapeutic regimens for MBC,
anthracyclins have been recommended in chemonaive cases and taxanes
in cases of prior treatment with anthracyclins in adjuvant
settings. However, since anthracyclins and taxanes are standard
chemotherapeutic agents in adjuvant settings, a number of patients
with recurrent breast cancer have already been treated with
regimens that included these agents. Anthracyclins and taxanes are
also not indicated for patients with poor PS, insufficient bone
marrow or organ function, or for elderly patients. Since patients
with insufficient expression of the estrogen receptor (ER), i.e.,
<50% of ER-positive cancer cells in the tumor or
ER-positive/progesterone receptor-negative tumors, are not expected
to respond to endocrine therapy alone, chemotherapy is occasionally
indicated in combination with endocrine therapy even in patients
with hormone-sensitive tumors. For patients previously treated with
anthracyclins or taxanes, therapeutic options are limited to less
toxic agents such as vinorelbine, gemcitabine, capecitabine, TS-1
and ixabepilone. When vinorelbine, gemcitabine or liposomal
doxorubicine was used alone for palliative care, ORR or PFS were
reported to be modest, while OS was expected to be ∼12 months
(26). Capecitabine, approved by
the Federal Diet and Food Association for administration in
patients with MBC who were refractory to anthracyclins and taxanes,
has shown favorable efficacy with ORR of 15–29%, PFS of 3.1–4.9
months, and OS of 9.1–15 months in patients (16,17,33).
Therefore, capecitabine is strongly recommended for patients with
MBC who have been heavily pre-treated, are elderly or have poor
PS.
Metronomic chemotherapy is defined as ‘continuous or
frequent treatment with low doses of anticancer drugs, often given
with other methods of therapy’ in the dictionary of the ‘Cancer
Terms’ of the National Cancer Institute. In this study, 29 of the
55 patients with MBC were selected to receive metronomic regimens.
However, 20 of the 29 patients had mental or physical conditions,
including insufficient bone marrow or organ function due to heavy
prior chemotherapy or comorbidities, advanced age or poor PS. The
remaining 9 patients requested this regimen, while 5 of them were
reluctant to experience hair loss. Patients receiving metronomic
regimens were older and had received more prior chemotherapy
regimens compared to patients who received non-metronomic regimens
(Table IV). A comparison of
clinical outcomes in patients receiving metronomic regimens and
patients receiving non-metronomic regimens showed that median TTF,
TTP and OS were significantly prolonged in the metronomic group
compared with those in the non-metronomic group (Table V). Seventy-five percent of patients
in the metronomic group had ≥12 months TTF, while >80% of the
patients in the non-metronomic group had <12 months TTF. The
results showing no difference in ORR in the two groups suggest no
correlation between ORR and survival.
In conclusion, metronomic chemotherapy for long-term
administration is strongly recommended for patients with MBC who
are elderly, have been heavily pre-treated with cytotoxic agents or
have poor PS since it may lead to prolonging survival with
minimized toxicity.
Acknowledgements
This study was supported in part by a
Grant-in-Aid for Scientific Research from the Ministry of
Education, Science, Sports and Culture, Japan (nos. 10671249,
13671380, 14571262 and 15591340).
References
|
1
|
Smith I and Chua S: Medical treatment of
early breast cancer. I: adjuvant treatment. BMJ. 332:34–37. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Early Breast Cancer Trialists’
Collaborative Group (EBCTCG): Effects of chemotherapy and hormonal
therapy for early breast cancer on recurrence and 15-year survival:
an overview of the randomized trials. Lancet. 365:1687–1717.
2005.PubMed/NCBI
|
|
3
|
Bria E, Nistico C, Cuppone F, et al:
Benefit of taxanes as adjuvant chemotherapy for early breast
cancer: pooled analysis of 15,500 patients. Cancer. 106:2337–2344.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Buzdar AU, Singletary SE, Valero V, et al:
Evaluation of paclitaxel in adjuvant chemotherapy for patients with
operable breast cancer: preliminary data of a prospective
randomized trial. Clin Cancer Res. 8:1073–1079. 2002.PubMed/NCBI
|
|
5
|
Bontenbal M, Andersson M, Wildiers J, et
al: Doxorubicin vs epirubicin, report of a second-line randomized
phase II/III study in advanced breast cancer. EORTC Breast Cancer
Cooperative Group. Br J Cancer. 77:2257–2263. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jassem J, Pieńkowski T, Płuzańska A, et
al: Doxorubicin and paclitaxel versus fluorouracil, doxorubicin,
and cyclophosphamide as first-line therapy for women with
metastatic breast cancer: final results of a randomized phase III
multicenter trial. J Clin Oncol. 19:1707–1715. 2001.
|
|
7
|
Perez DJ, Harvey VJ, Robinson BA, et al: A
randomized comparison of single-agent doxorubicin and epirubicin as
first-line cytotoxic therapy in advanced breast cancer. J Clin
Oncol. 9:2148–2152. 1991.PubMed/NCBI
|
|
8
|
Bonneterre J, Dieras V, Tubiana-Hulin M,
et al: Phase II multicentre randomised study of docetaxel plus
epirubicin vs 5-fluorouracil plus epirubicin and cyclophosphamide
in metastatic breast cancer. Br J Cancer. 91:1466–1471.
2004.PubMed/NCBI
|
|
9
|
Sledge GW, Neuberg D, Bernardo P, Ingle
JN, Martino S, Rowinsky EK and Wood WC: Phase III trial of
doxorubicin, paclitaxel, and the combination of doxorubicin and
paclitaxel as front-line chemotherapy for metastatic breast cancer:
an intergroup trial (E1193). J Clin Oncol. 21:588–592. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Paridaens R, Biganzoli L, Bruning P, et
al: Paclitaxel versus doxorubicin as first-line single-agent
chemotherapy for meta-static breast cancer: a European Organization
for Research and Treatment of Cancer Randomized Study with
cross-over. J Clin Oncol. 18:724–733. 2000.
|
|
11
|
Chan S, Friedrichs K, Noel D, et al:
Prospective randomized trial of docetaxel versus doxorubicin in
patients with metastatic breast cancer. J Clin Oncol. 17:2341–2354.
1999.PubMed/NCBI
|
|
12
|
Rha SY, Moon YH, Jeung HC, et al:
Gemcitabine monotherapy as salvage chemotherapy in heavily
pretreated metastatic breast cancer. Breast Cancer Res Treat.
90:215–221. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Spielmann M, Llombart-Cussac A, Kalla S,
et al: Single-agent gemcitabine is active in previously treated
metastatic breast cancer. Oncology. 60:303–307. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zelek L, Barthier S, Riofrio M, et al:
Weekly vinorelbine is an effective palliative regimen after failure
with anthracyclines and taxanes in metastatic breast carcinoma.
Cancer. 92:2267–2272. 2001. View Article : Google Scholar
|
|
15
|
Gasparini G, Caffo O, Barni S, Frontini L,
Testolin A, Guglielmi RB and Ambrosini G: Vinorelbine is an active
antiproliferative agent in pretreated advanced breast cancer
patients: a phase II study. J Clin Oncol. 12:2094–2101.
1994.PubMed/NCBI
|
|
16
|
Blum JL, Dieras V, Lo Russo PM, Horton J,
Rutman O, Buzdar A and Osterwalder B: Multicenter, Phase II study
of capecitabine in taxane-pretreated metastatic breast carcinoma
patients. Cancer. 92:1759–1768. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Blum JL, Jones SE, Buzdar AU, et al:
Multicenter phase II study of capecitabine in paclitaxel-refractory
metastatic breast cancer. J Clin Oncol. 17:485–493. 1999.PubMed/NCBI
|
|
18
|
Jassem J, Carroll C, Ward SE, Simpson E
and Hind D: The clinical efficacy of cytotoxic agents in locally
advanced or metastatic breast cancer patients pretreated with an
anthracycline and a taxane: a systematic review. Eur J Cancer.
45:2749–2758. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Pivot XB, Li RK, Thomas ES, et al:
Activity of ixabepilone in oestrogen receptor-negative and
oestrogen receptor-progesterone receptor-human epidermal growth
factor receptor 2-negative metastatic breast cancer. Eur J Cancer.
45:2940–2946. 2009. View Article : Google Scholar
|
|
20
|
Ito Y, Osaki Y, Tokudome N, Sugihara T,
Takahashi S, Iwase T and Hatake K: Efficacy of S-1 in heavily
pretreated patients with metastatic breast cancer: cross-resistance
to capecitabine. Breast Cancer. 16:126–131. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Savio G, Laudani A, Leonardi V, Pepe A,
Scianna C, Gebbia V and Agostara B: Treatment of metastatic breast
cancer with vinorelbine and docetaxel. Am J Clin Oncol. 29:276–280.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Vici P, Di Lauro L, Sergi D, et al: A
phase II trial of docetaxel and vinorelbine in patients with
advanced breast cancer previously treated with anthracyclines.
Oncology. 75:175–181. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Albain KS, Nag SM, Calderillo-Ruiz G, et
al: Gemcitabine plus paclitaxel versus paclitaxel monotherapy in
patients with meta-static breast cancer and prior anthracycline
treatment. J Clin Oncol. 26:3950–3957. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Chan S, Romieu G, Huober J, et al: Phase
III study of gemcitabine plus docetaxel compared with capecitabine
plus docetaxel for anthracycline-pretreated patients with
metastatic breast cancer. J Clin Oncol. 27:1753–1760. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
O’Shaughnessy J, Miles D, Vukelja S, et
al: Superior survival with capecitabine plus docetaxel combination
therapy in anthracycline-pretreated patients with advanced breast
cancer: phase III trial results. J Clin Oncol. 20:2812–2823.
2002.PubMed/NCBI
|
|
26
|
Oostendorp LJ, Stalmeier PF, Donders AR,
van der Graaf WT and Ottevanger PB: Efficacy and safety of
palliative chemotherapy for patients with advanced breast cancer
pretreated with anthracyclines and taxanes: a systematic review.
Lancet Oncol. 12:1053–1061. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kerbel RS and Kamen BA: The
anti-angiogenic basis of metronomic chemotherapy. Nat Rev Cancer.
4:423–436. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
28
|
Colleoni M, Rocca A, Sandri MT, et al:
Low-dose oral methotrexate and cyclophosphamide in metastatic
breast cancer: antitumor activity and correlation with vascular
endothelial growth factor levels. Ann Oncol. 13:73–80. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Colleoni M, Orlando L, Sanna G, et al:
Metronomic low-dose oral cyclophosphamide and methotrexate plus or
minus thalidomide in metastatic breast cancer: antitumor activity
and biological effects. Ann Oncol. 17:232–238. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wong NS, Buckman RA, Clemons M, et al:
Phase I/II trial of metronomic chemotherapy with daily dalteparin
and cyclophosphamide, twice-weekly methotrexate, and daily
prednisone as therapy for metastatic breast cancer using vascular
endothelial growth factor and soluble vascular endothelial growth
factor receptor levels as markers of response. J Clin Oncol.
28:723–730. 2010.
|
|
31
|
Nabholtz JM, Falkson C, Campos D, et al:
Docetaxel and doxorubicin compared with doxorubicin and
cyclophosphamide as first-line chemotherapy for metastatic breast
cancer: results of a randomized, multicenter, phase III trial. J
Clin Oncol. 21:968–975. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Miller K, Wang M, Gralow J, et al:
Paclitaxel plus bevacizumab versus paclitaxel alone for metastatic
breast cancer. N Engl J Med. 357:2666–2676. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Fumoleau P, Largillier R, Clippe C, et al:
Multicentre, phase II study evaluating capecitabine monotherapy in
patients with anthracycline- and taxane-pretreated metastatic
breast cancer. Eur J Cancer. 40:536–542. 2004. View Article : Google Scholar : PubMed/NCBI
|