Introduction
Gefitinib, which is one of the highly promising
epidermal growth factor receptor-tyrosine kinase inhibitors
(EGFR-TKIs), is administered orally once daily for patients with
non-small-cell lung cancer (NSCLC) (1). Among NSCLCs, adenosquamous cell lung
cancer (ASCLC) is a morphologically mixed type of tumor, including
two cell components, adenocarcinoma and squamous cell carcinoma, in
varying proportions, each representing ≥10% of the entire tumor
(2). Previous studies evaluated
the possibility of monoclonality and similar biological
characteristics, including the frequency of EGFR mutation, of the
two components (3–12). However, the number of currently
available studies on the response of EGFR-positive ASCLC to
gefitinib therapy is limited (13). We herein report a case of
metastatic ASCLC successfully treated with gefitinib.
Case report
A 66-year-old female, with no smoking history,
presented at the Mito Medical Center (Mito, Japan) with a cough and
intermittent hemoptysis over the past 6 weeks. Chest radiography
and computed tomography (CT) revealed a large cavitary mass in the
lower lobe of the left lung (Fig.
1). Bronchoscopy revealed a tumor occluding the left lower
bronchus, with active bleeding. The patient was initially diagnosed
with adenocarcinoma on the basis of histopathological examination
of transbrochial biopsy specimens. Distant metastasis was not
detected. The patient’s Eastern Cooperative Oncology Group
performance status score was 1. In order to prevent deterioration
of the respiratory condition due to hemoptysis, the patient
underwent lobectomy of the left lower lung and mediastinal lymph
node dissection. The resected tumor exhibited adenocarcinomatous
and squamous cell carcinomatous components, with each comprising
≥10% of the tumor (Fig. 2). The
final pathological diagnosis was ASCLC staged as pT2bN2M0. The two
components of the surgically resected tumor were precisely
separated by manual microdissection under microscopic observation,
to avoid contamination of each sample from different components. An
EGFR exon 19 deletion was identified in both components. Soon after
the surgical resection, the patient received four courses of
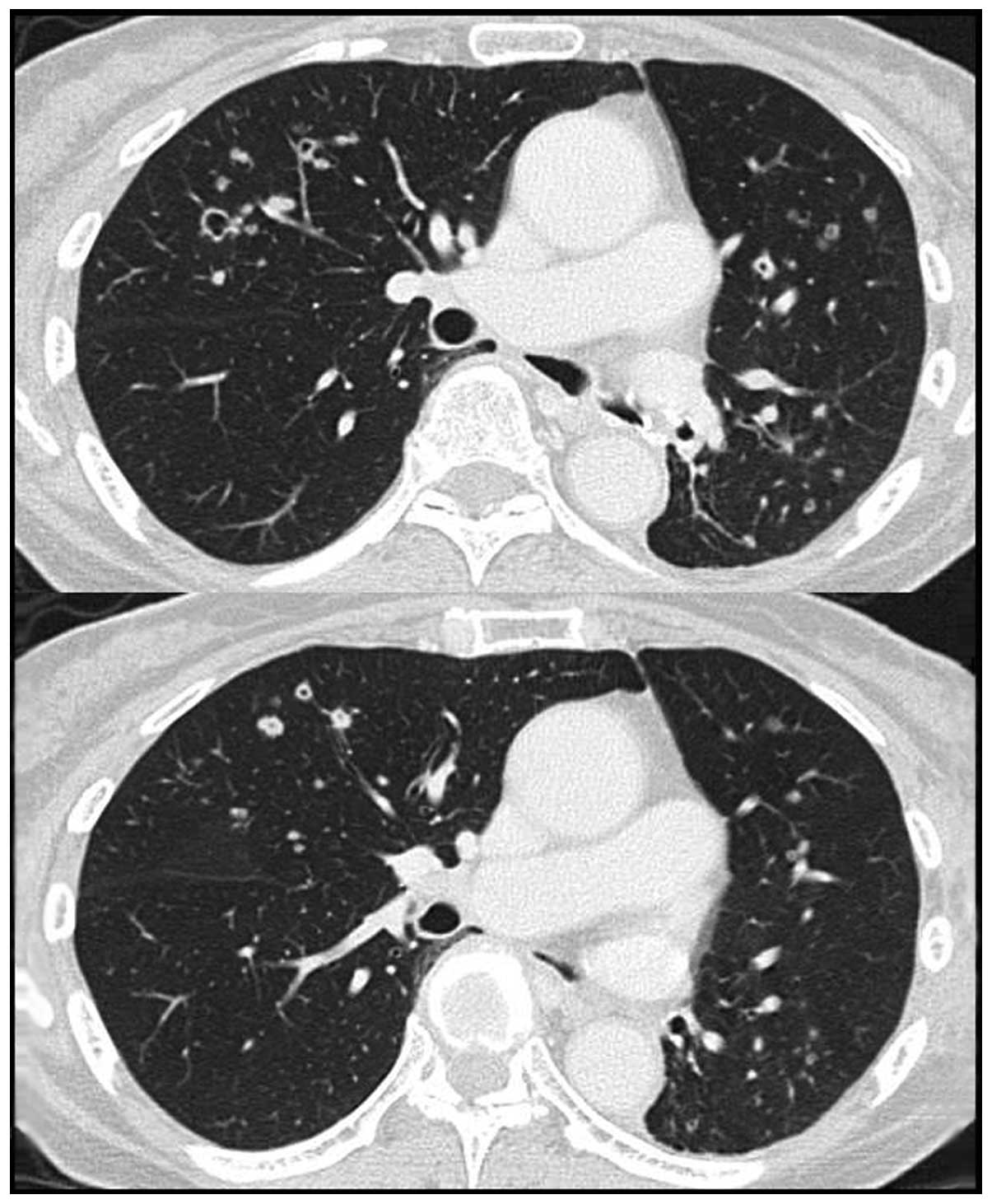
chemotherapy with carboplatin and pemetrexed. However, six months
after the chemotherapy, small cavitary metastases (≤10 mm) were
identified in the lungs bilaterally (Fig. 3). Therefore, treatment with 250 mg
of gefitinib once daily was initiated. A chest CT scan on day 28 of
gefitinib administration revealed a substantial regression of the
metastatic cavitary tumors in both lungs, with thinning of the
walls (Fig. 4). There were no
severe side-effects, such as lung toxicity. Treatment with
gefitinib was continued in the outpatient clinic without any signs
of tumor progression 19 months after the initiation of the
treatment.
Discussion
Lung cancer is the leading cause of cancer-related
mortality worldwide (14). NSCLCs
are the most frequent type of lung tumors, with two major
histological subtypes: adenocarcinomas and squamous cell
carcinomas. A less frequent subtype of NSCLCs, ASCLC, is a
morphologically mixed type of tumor, including two cell components,
adenocarcinoma and squamous cell carcinoma, in varying proportions,
each representing ≥10% of the entire tumor (2). Previous studies have suggested that
ASCLC represents 0.3–5% of NSCLCs (15,16).
In certain ASCLC patients, cavitary formation was observed
(17,18). Kazerooni et al (18) reported that four of 30 cases
exhibited cavitary formation. Cavities may be formed as a result of
a unidirectional check-valve mechanism (17). Another mechanism of cavity
formation may depend on the ischemic or colliquative tumor necrosis
associated with neutrophil infiltration into the central portion of
lesion. Cavitary formation due to tumor necrosis is common in
squamous cell carcinomas, particularly in those developing
peripherally in the lung (19). In
our patient, the primary lesion exhibited cavitary formation and
its wall was composed of the squamous cell carcinomatous component,
which was pathologically confirmed. Certain metastatic lesions ≤10
mm also exhibited cavitation. Notably, the wall of the cavities,
which were composed of the squamous cell carcinomatous component,
were thinned with gefitinib therapy, although the cavities
themselves did not change in size in the majority of the pulmonary
lesions. The frequency of EGFR mutation-positive ASCLC patients was
previously reported (3–12). However, the number of studies on
the response of the lesions, either shrinkage or disappearance of
pulmonary metastases with cavitary formation, specifically to
gefitinib therapy is limited (13). Furthermore, there has been no
report on long-term survivors who were successfully treated with
gefitinib. Recently, Shukuya et al (13) reviewed the efficacy of gefitinib
for non-adenocarcinoma NSCLC patients, including two ASCLC
patients, and reported a response rate of 50%, a disease control
rate 100% and a median progression-free survival of 5.3 months
(13).
Although ASCLC is included in NSCLCs, the frequency
of EGFR abnormalities has not been completely evaluated, due to the
rarity of ASCLC (3–12). Two previous studies (4,5),
reported EGFR abnormalities in ASCLC tumors identical to those
previously described in primary lung adenocarcinoma: Ohtsuka et
al (4) identified EGFR
TK-domain gene mutations in 2 (50%) of 4 patients with ASCLC,
whereas Kang et al (5)
identified EGFR mutations in 11 (44%) of 25 ASCLC patients.
However, Sasaki et al (11)
reported that only four (15.4%) of 26 patients with ASCLC were
positive for EGFR mutation.
The possibility of monoclonality and similar
biological characteristics regarding genetic alterations,
chromosomal abnormalities and immunohistochemical reactions in the
two components of ASCLCs were evaluated in previous studies
(3–12). With regard to EGFR mutations, Kang
et al (5) demonstrated
identical changes in the two components of ASCLC tumors, with of
the nine mutations in 11 ASCLC patients being located in exon 19
(5). Furthermore, Toyooka et
al (8) reported that three
(27%) of the 11 ASCLC patients harboured EGFR mutations (two
mutations in exon 19 and one in exon 21), which were identical in
the two components. In our case, an EGFR mutation (exon 19
deletion) was identified in the two components of the surgically
resected tumor. Taken together, the results of previous studies and
our findings indicated that TKIs may be a reasonable therapeutic
option for ASCLC patients harbouring EGFR mutations. Furthermore,
identical EGFR mutations in the adenocarcinomatous and squamous
cell carcinomatous components suggest the possibility of
monoclonality and similar biological characteristics of the two
components.
The present study suggested that gefitinib is a
viable therapeutic option for EGFR mutation-positive patients with
ASCLC. However, further investigations into the molecular
determinants of tumor monoclonality in the histogenesis of ASCLC
and response to EGFR-targeted therapies in patients with ASCLC are
required.
References
|
1
|
D’Incecco A and Cappuzzo F: Gefitinib for
non-small-cell lung cancer treatment. Expert Opin Drug Saf.
10:987–996. 2011.
|
|
2
|
Travis WD, Brambilla E, Muller-Hermelink
HK and Harris CC: Pathology and Genetics: Tumours of the Lung,
Pleura, Thymus and Heart. IARC Press; Lyon: 2004
|
|
3
|
Qin BM, Chen X, Zhu JD and Pei DQ:
Identification of EGFR kinase domain mutations among lung cancer
patients in China: implication for targeted cancer therapy. Cell
Res. 15:212–217. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ohtsuka K, Ohnishi H, Fujiwara M, et al:
Abnormalities of epidermal growth factor receptor in lung
squamous-cell carcinomas, adenosquamous carcinomas, and large-cell
carcinomas: tyrosine kinase domain mutations are not rare in tumors
with an adenocarcinoma component. Cancer. 109:741–750. 2007.
View Article : Google Scholar
|
|
5
|
Kang SM, Kang HJ, Shin JH, et al:
Identical epidermal growth factor receptor mutations in
adenocarcinomatous and squamous cell carcinomatous components of
adenosquamous carcinoma of the lung. Cancer. 109:581–587. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Niho S, Yokose T, Kodama T, Nishiwaki Y
and Mukai K: Clonal analysis of adenosquamous carcinoma of the
lung. Jpn J Cancer Res. 90:1244–1247. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kanazawa H, Ebina M, Ino-Oka N, et al:
Transition from squamous cell carcinoma to adenocarcinoma in
adenosquamous carcinoma of the lung. Am J Pathol. 156:1289–1298.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Toyooka S, Yatabe Y, Tokumo M, et al:
Mutations of epidermal growth factor receptor and K-ras genes in
adenosquamous carcinoma of the lung. Int J Cancer. 118:1588–1590.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Huang SF, Liu HP, Li LH, et al: High
frequency of epidermal growth factor receptor mutations with
complex patterns in non-small cell lung cancers related to
gefitinib responsiveness in Taiwan. Clin Cancer Res. 10:8195–8203.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kosaka T, Yatabe Y, Endoh H, Kuwano H,
Takahashi T and Mitsudomi T: Mutations of the epidermal growth
factor receptor gene in lung cancer: biological and clinical
implications. Cancer Res. 64:8919–8923. 2004. View Article : Google Scholar
|
|
11
|
Sasaki H, Endo K, Yukiue H, Kobayashi Y,
Yano M and Fujii Y: Mutation of epidermal growth factor receptor
gene in adenosquamous carcinoma of the lung. Lung Cancer.
55:129–130. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mitsudomi T, Kosaka T, Endoh H, et al:
Mutations of the epidermal growth factor receptor gene predict
prolonged survival after gefitinib treatment in patients with
non-small-cell lung cancer with postoperative recurrence. J Clin
Oncol. 23:2513–2520. 2005. View Article : Google Scholar
|
|
13
|
Shukuya T, Takahashi T, Kaira R, et al:
Efficacy of gefitinib for non-adenocarcinoma non-small-cell lung
cancer patients harboring epidermal growth factor receptor
mutations: a pooled analysis of published reports. Cancer Sci.
102:1032–1037. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Alberg AJ, Brock MV and Samet JM:
Epidemiology of lung cancer: looking to the future. J Clin Oncol.
23:3175–3185. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ruffini E, Rena O, Oliaro A, et al: Lung
tumors with mixed histologic pattern. Clinico-pathologic
characteristics and prognostic significance. Eur J Cardiothorac
Surg. 22:701–707. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
de Jong WK, Schaapveld M, Blaauwgeers JL
and Groen HJ: Pulmonary tumours in the Netherlands: focus on
temporal trends in histology and stage and on rare tumours. Thorax.
63:1096–1102. 2008.PubMed/NCBI
|
|
17
|
Sugimoto Y, Semba H, Fujii S, Furukawa E
and Kurano R: Clinical analysis of primary lung cancer with a
thin-walled cavity to explain the mechanism of thin-walled cavity
formation. Nihon Kokyuki Gakkai Zasshi. 45:460–464. 2007.(In
Japanese).
|
|
18
|
Kazerooni EA, Bhalla M, Shepard JA and
McLoud TC: Adenosquamous carcinoma of the lung: radiologic
appearance. AJR Am J Roentgenol. 163:301–306. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Honda O, Tsubamoto M, Inoue A, et al:
Pulmonary cavitary nodules on computed tomography: differentiation
of malignancy and benignancy. J Comput Assist Tomogr. 31:943–949.
2007. View Article : Google Scholar : PubMed/NCBI
|