Introduction
Retroperitoneal abscess is a rare but
life-threatening infection, which may be caused by perforated or
penetrated diverticulitis, ruptured appendix and inflammatory bowel
disease (1–4). Appropriate medical and surgical
management is required in order to reduce the associated high
mortality rate. This is a rare case of retroperitoneal abscess,
which continued to spread, eventually leading to the formation of a
scrotal abscess, shortly after administration of chemotherapy for
lung cancer.
Case report
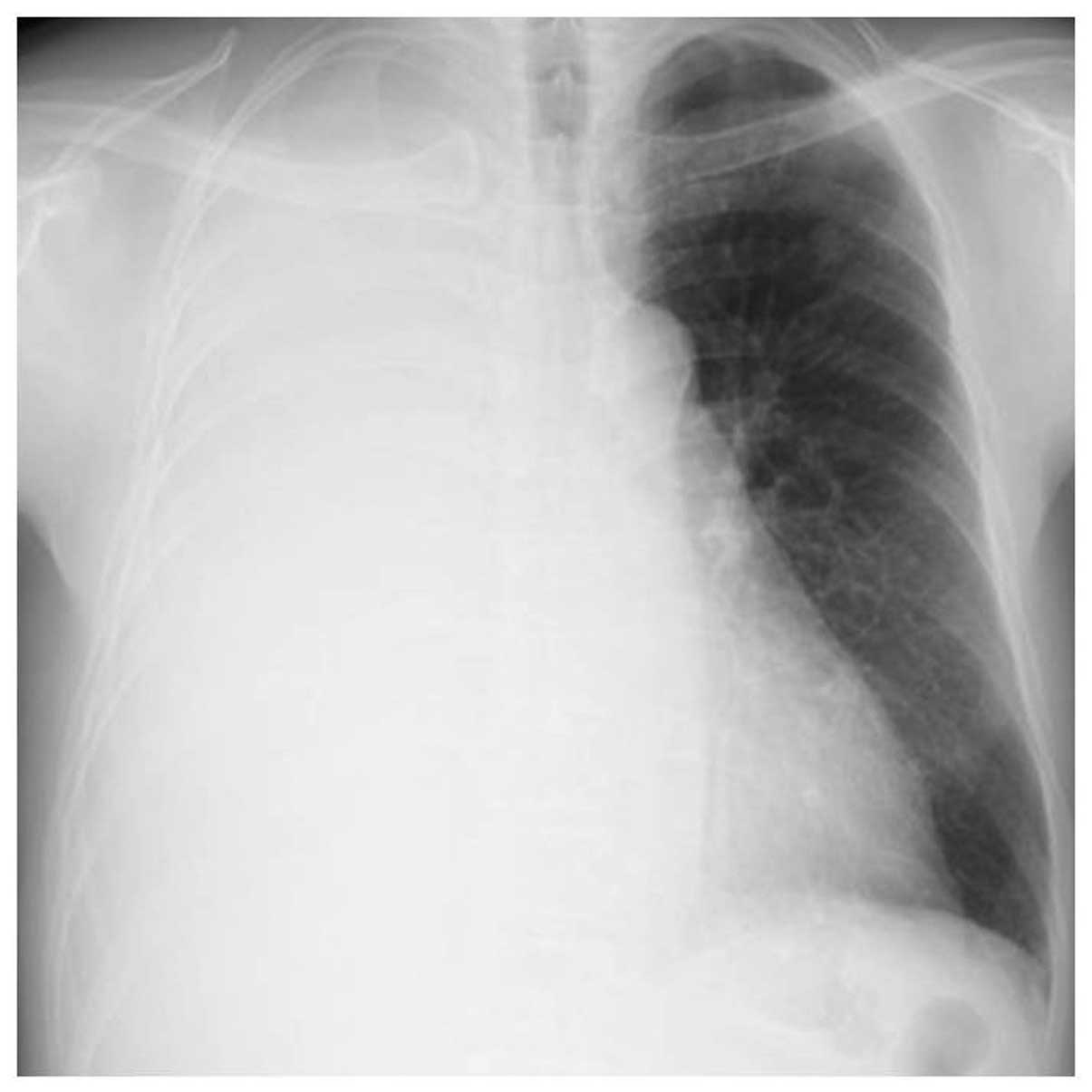
A 59-year-old male, with no previous reported health
issues, was referred to the Mito Medical Center (Mito, Japan) due
to a persistent productive cough over the last few months. Chest
radiography revealed a massive pleural fluid collection with a
mediastinal shift (Fig. 1). On the
basis of the results of a computed tomography (CT) scan and
bronchoscopy, the patient was diagnosed with lung adenocarcinoma
with pleuritis carcinomatosis, without any detected distant
metastasis. Subsequently, combination chemotherapy with cisplatin
and pemetrexed was administered. Nine days after the initiation of
chemotherapy, the patient developed right lower quadrant abdominal
pain and high fever. The blood examination data did not indicate
leukopenia (white blood cell count, 7,500 cells/μl), but revealed a
high C-reactive protein (CRP) level (16.7 mg/dl). A CT scan
revealed fluid and gas collection in the retroperitoneum adjacent
to the cecum (Fig. 2). The
appendix was not identified by imaging and, due to the presence of
a cecal diverticulum, the patient was diagnosed with pericolic
abscess and emergent drainage was performed. Administration of the
meropenem and clindamycin was initiated, a catheter was inserted
into the abscess and pus with gas and odor was drained, strongly
suggesting an infection by gas-producing anaerobic microorganisms.
The patient recovered temporarily; however, the infection continued
to spread and a scrotal abscess developed (Fig. 3), although the size of the initial
abscess had been reduced as a result of the drainage. X-ray imaging
using iodinated contrast media revealed a fistular tract between
the cecum and the abscess cavity. Perforated appendicitis was
suspected and an appendectomy as performed. A microbiological
examination of the pus revealed the presence of Escherichia
coli, in addition to other anaerobic bacteria. The patient
recovered well postoperatively and proceeded to receive treatment
for the lung adenocarcinoma, achieving a partial response with
additional courses of chemotherapy one month after the surgery. The
operative findings indicated perforated appendicitis. Six months
after the surgical treatment, the patient remains alive and is
treated with chemotherapy in the outpatient clinic.
Discussion
There have been several reports on the incidence of
bowel perforation in patients with acute appendicitis or colon
cancer resulting in the development of retroperitoneal, psoas, or
scrotal abscesses (1,5,6).
Takakura et al (6) reported
a case of retroperitoneal abscess complicated by necrotizing
fasciitis of the thigh in a patient with sigmoid colon cancer. The
authors of that study reported that the abscess developed 4 months
following the initiation of chemotherapy (6). Maguire and Kaye (7) reported two cases in which patients
developed a psoas abscess after undergoing chemotherapy for bulky
retroperitoneal deposits of teratoma. In those cases, the abscess
developed 4 weeks after the last course of chemotherapy and 2 years
after undergoing surgery and radiotherapy (7). In both cases, the primary lesion was
located in the abdomen or in the retroperitoneal space. There was
no chemotherapy-induced myelosuppression in those patients and
their abscesses developed long after treatment (7). We also previously reported a case of
retrocecal appendicitis, which resulted in perforation shortly
after chemotherapy for lung cancer (8). In that case, the complication
developed under conditions of leukocytopenia (white blood cell
count, 500/μl), but did not result in the formation of a
retroperitoneal abscess (8). We
successfully treated that condition with effective antibiotics and
appendectomy after the recovery of leukocytopenia. We could not
identify any case with retroperitoneal abscess during or shortly
after chemotherapy for tumors originated in sites other than the
abdomen or retroperitoneum. Therefore, to the best of our
knowledge, this is the first case exhibiting development of
retroperitoneal and scrotal abscesses due to the spread of the
infection cause by perforated appendicitis, during or shortly after
the administration of chemotherapy for lung cancer. The causes
underlying the development of a complication such as
retroperitoneal abscess shortly after chemotherapy for lung cancer
have not been elucidated.
The clinical characteristics of retroperitoneal
abscesses include high fever with chills and tenderness over the
affected area, along with changes in skin color and palpable
crepitus (1,5,6).
However, the insidious occult characteristics of these abscesses
may sometimes lead to diagnostic delay. Additionally, due to its
acute and rapidly progressive course, retroperitoneal abscess is
associated with a high morbidity and mortality rate (1,5,6). In
the present case, the development of retroperitoneal abscess did
not occur as febrile neutropenia. Had this complication developed
during myelosuppression, the clinical course may have been more
complicated. We initiated administration of intravenous antibiotics
immediately after obtaining samples for blood culture. Following an
improvement in CRP levels and leukocytosis, a drainage tube was
inserted. Recent advances in antimicrobial agents, such as
carbapenems and new quinolones, have achieved higher disease
control rates, even in severe infections (9,10).
The appropriate selection of antibiotics and surgical drainage are
considered to be mandatory for patients with retroperitoneal
abscesses, whereas surgical debridement is indicated when the
abscess is accompanied by symptoms such as intestinal obstruction
or bleeding. Our reported case highlights the importance of early
diagnosis and appropriate treatment in order to avoid subsequent
serious complications, such as septicemia and septic shock.
Accurate and timely clinical judgment and a careful consideration
of the balance between the risks and benefits are required prior to
medical and surgical intervention.
Retroperitoneal abscess is a rare but potentially
fatal complication in patients treated with chemotherapy for lung
cancer, particularly those who are under, or shortly after,
chemotherapy-induced myelosuppression. Unexpected infectious
complications, such as retroperitoneal abscess, may also develop in
patients with lung cancer and physicians should be alert on such a
rare complication.
References
|
1
|
Rotstein OD, Pruett TL and Simmons RL:
Thigh abscess. An uncommon presentation of intraabdominal sepsis.
Am J Surg. 151:414–418. 1986.PubMed/NCBI
|
|
2
|
Hall JF, Roberts PL, Ricciardi R, et al:
Long-term follow-up after an initial episode of diverticulitis:
what are the predictors of recurrence? Dis Colon Rectum.
54:283–288. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Banner MP: Genitourinary complications of
inflammatory bowel disease. Radiol Clin North Am. 25:199–209.
1987.PubMed/NCBI
|
|
4
|
Cybulsky IJ and Tam P: Intra-abdominal
abscesses in Crohn’s disease. Am Surg. 56:678–682. 1990.
|
|
5
|
Panwalker AP: Unusual infections
associated with colorectal cancer. Rev Infect Dis. 10:347–364.
1988. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Takakura Y, Ikeda S, Yoshimitsu M, et al:
Retroperitoneal abscess complicated with necrotizing fasciitis of
the thigh in a patient with sigmoid colon cancer. World J Surg
Oncol. 7:742009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Maguire J and Kaye SB: Psoas abscess:
unusual complication of effective chemotherapy for teratoma. Br Med
J (Clin Res Ed). 290:18701985. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Satoh H, Yano H, Naitoh T, et al: A case
of retrocecal appendicitis occurrence during effective chemotherapy
in lung cancer. Jpn J Cancer Clin. 35:389–392. 1989.(In
Japanese).
|
|
9
|
Rodriguez CL, Ferran NA, Lyons K and Evans
RO: Bilateral glenohumeral septic arthritis secondary to
retroperitoneal abscess. Bull NYU Hosp Jt Dis. 67:378–380.
2009.PubMed/NCBI
|
|
10
|
Brook I: Urinary tract and genito-urinary
suppurative infections due to anaerobic bacteria. Int J Urol.
11:133–141. 2004. View Article : Google Scholar : PubMed/NCBI
|