Introduction
Hepatocellular carcinoma (HCC) is one of the most
common malignant tumors worldwide. Various therapeutic modalities
are currently used to treat this disease, including liver
transplantation (1), surgical
resection (2,3), percutaneous ethanol injection
(4), radiofrequency ablation
therapy (RFA) (5–7) and transcatheter arterial
chemoembolization (TACE) (8).
Liver cirrhosis with a low Child-Pugh grade due to infection with
hepatitis virus is often present in HCC patients. Poor hepatic
reserve function makes surgical resection difficult and liver
transplantation is significantly limited by the shortage of organ
donors. RFA has recently gained wide acceptance worldwide, mainly
due to its relatively low level of invasiveness, ease of use and
effectiveness (9,10). The incidence of local tumor
progression of HCC reportedly ranges between 0.9 and 31.3%
(5,9,11–18).
Local tumor recurrence may occur due to untreated satellite
lesions, which are too small to detect on imaging prior to RFA
(19). HCC is generally considered
to spread via the bloodstream. A previous study by Sakon et
al (20) reported that
satellite lesions existed in the blood drainage area determined by
computed tomography during hepatic arteriography (CTHA). In our
experience, local recurrence often occurs in this blood drainage
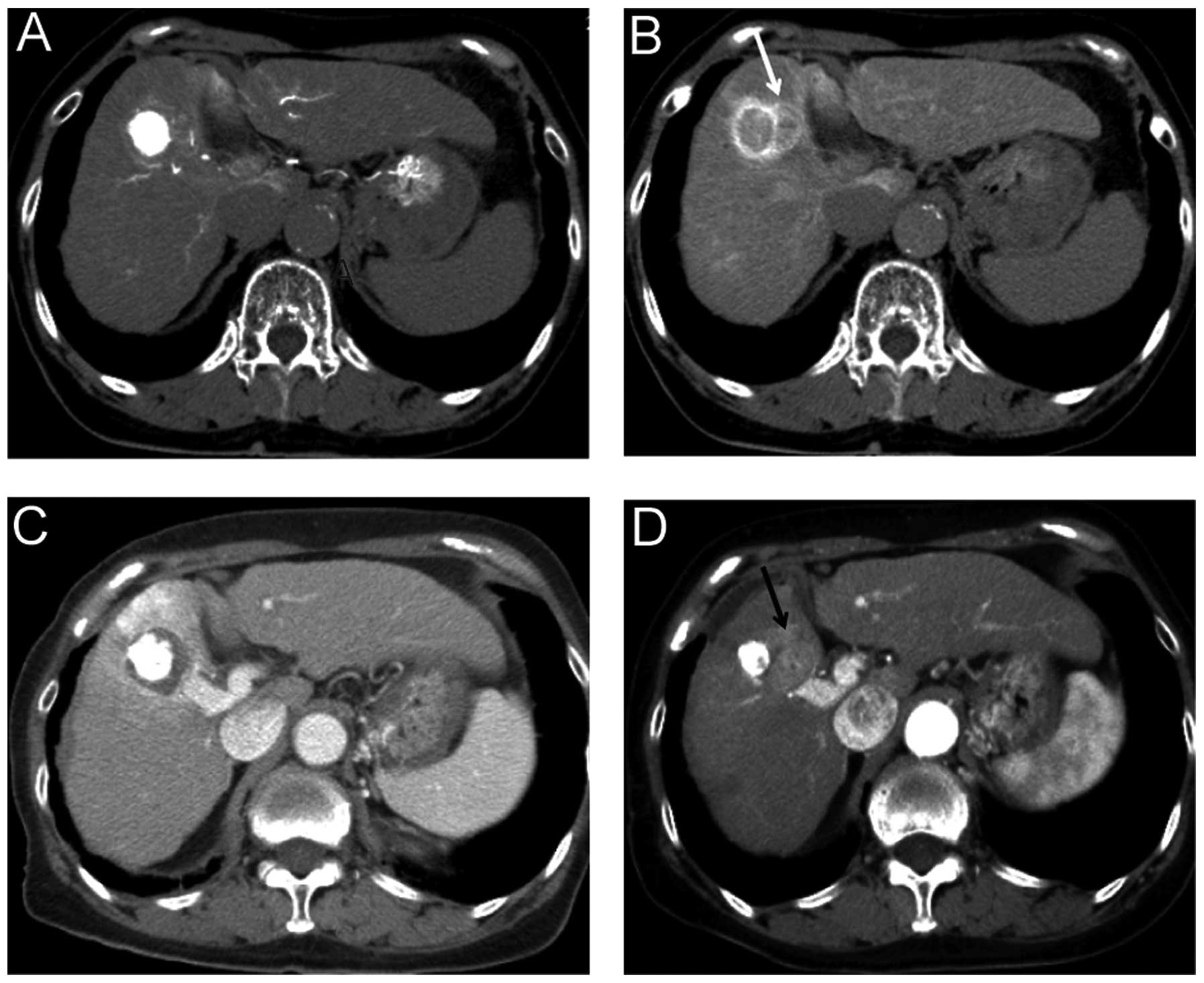
area, despite complete ablation of the primary nodule (Fig. 1). To the best of our knowledge, no
prior study has evaluated the association between local recurrence
following RFA and ablation of the blood drainage area.
The aim of this prospective cohort study was to
evaluate the frequency of intrahepatic metastases within the blood
drainage area of the tumor following RFA.
Materials and methods
Patients
All participants provided written informed consent
prior to enrollment and the study protocols were approved by the
Institutional Ethics Committee. The participants comprised 364
patients [260 men and 104 women; mean age ± SD, 67.4±8.6 years] who
had been diagnosed with HCC at the Department of Gastroenterology
and Metabology of Ehime University Hospital, Japan, between April,
2002 and December, 2011. The criteria for inclusion in the study
were as follows: i) Eastern Cooperative Oncology Group (ECOG)
performance status 0–2; ii) patients with unresectable lesions or
who had declined hepatectomy; iii) presence of a single lesion ≤5
cm in diameter; iv) liver function A or B according to Child-Pugh
classification; and v) no extrahepatic metastases or vascular
invasion. The exclusion criteria were as follows: i) total
bilirubin level ≥3.0 mg/dl; ii) platelet count
<50,000/mm3; iii) prothrombin activity <50%; and
iv) refractory ascites. HCC was defined as a nodule showing
equivalent to decreased portal perfusion on computed tomography
during arterial portography (CTAP) and increased arterial perfusion
on early-phase CTHA with corona enhancement on late-phase CTHA. The
combination of transarterial chemoembolization with RFA was
performed for all the nodules.
RFA procedure and post-treatment
analysis
RFA was performed with an internally cooled
electrode (Radionics, Burlington, MA, USA). In each lesion, in
order to obtain a suitable safety margin around the viable tumor,
we selected a 2- or 3-cm ablation-type needle. A total of 340
patients underwent ablation under ultrasonographic guidance
(6,7), 21 patients using a laparoscopic
procedure (21) and 3 patients by
surgical incision. To assess the ablated area and complications,
dynamic CT was performed within 3 days of the ablation. The goal of
the treatment was to achieve complete ablation of the
hypoattenuating areas visualized during the portal venous phases
and extending beyond the tumor itself. Images from the portal
venous phase were used, as the increase in inflammatory blood flow
caused by the ablation could not be overlooked in the arterial
phase. Additional ablation sessions were scheduled if the presence
of residual lesions was confirmed. The diagnostic and treatment
procedures were repeated until complete ablation was achieved
during a single hospitalization.
CTHA
CTAP and CTHA were performed in all the patients
prior to RFA, as previously described (22). A 4-Fr catheter was inserted through
the femoral artery into the superior mesenteric artery for CTAP and
into the common, proper, or replaced right hepatic artery for CTHA.
CTHA scans were obtained at a section thickness and collimation of
3–5 mm. Helical scanning was initiated 7 sec after the infusion of
iohexol (320–350 mg/ml of iodine) (Omnipaque; Daiichi, Tokyo,
Japan) into the common, proper, or replaced hepatic artery at a
rate of 1.8 ml/sec. The infusion of contrast material was continued
until 5 sec after the completion of early-phase CTHA. The scanning
time varied according to the individual liver size (~20–25 sec).
Thirty seconds after completing the contrast material infusion
(~62–67 sec after the initiation of the infusion), late-phase
scanning was commenced (22). When
a hypervascular tumor was identified on CTHA, the performance of
transcatheter arterial embolization was considered mandatory prior
to RFA, by injecting iodized oil (Lipiodol; Laboratoire Guerbet,
Paris, France) with a gelatin sponge (Gelfoam; Upjohn, Kalamazoo,
MI, USA) or gelatin sponge particles (Gelpart; Nippon Kayaku,
Tokyo, Japan) into the segmental or subsegmental branch of the
hepatic artery.
Imaging analysis
To assess the safety margins, the fusion imaging
method was used. We used an open source DICOM software (OsiriX
Foundation; Geneva, Switzerland) capable of performing imaging
fusion of CT images prior to and following RFA, as described
previously (23). CT data were
acquired from the CT workstation, with a 0.69-mm thickness. One of
two experienced radiologists performed CT image fusion using the
manual segmentation registration method. The late phase of CTHA
that depicted corona enhancement was selected and the portal phase
of dynamic CT following RFA was fused to this image (Fig. 2).
Statistical analysis
Consecutive case series were enrolled in this study.
Following ablation, the enrolled patients were divided into two
groups, as follows: i) group A, ablated area covering the entire
blood drainage area; or ii) group B, ablated area not covering the
entire blood drainage area. The cumulative local recurrence rate
was calculated using the Kaplan-Meier method and assessed using the
log-rank test. Continuous parameters were expressed as median and
range (10th and 90th percentiles) or as the means ± SD. Statistical
analysis was performed using the Student’s t-test for unpaired
data, the Mann-Whitney U test, χ2 test, Fisher’s exact
test, or Wilcoxon signed-ranks test, as applicable. P<0.05 was
considered to indicate a statistically significant difference. All
data were analyzed using JMP software, version 9 (SAS Institute
Japan, Tokyo, Japan).
Results
Clinical characteristics
The differences in the clinical characteristics
between the two groups are shown in Table I. Except for the width of the
ablation area, the baseline characteristics did not differ
significantly between the two groups.
 | Table IDifferences in clinical
characteristics. |
Table I
Differences in clinical
characteristics.
| Characteristics | Uncovered drainage
area | Covered drainage
area | P-value |
|---|
| No. | 114 | 250 | - |
| Female:male | 30:84 | 76:174 | 0.480 |
| Age (years) | 67.2±8.5 | 67.6±8.8 | 0.695 |
| Child-Pugh grade
(A:B) | 104:10 | 198:52 | 0.539 |
| Etiology
(HBV:HCV:other) | 11:93:10 | 39:169:42 | 0.843 |
| Tumor diameter
(mm) | 21.9±8.1 | 23.5±10.1 | 0.127 |
| Width of ablated area
(<5:6–10:>10 mm) | 54:60:0 | 153:65:32 | <0.0001 |
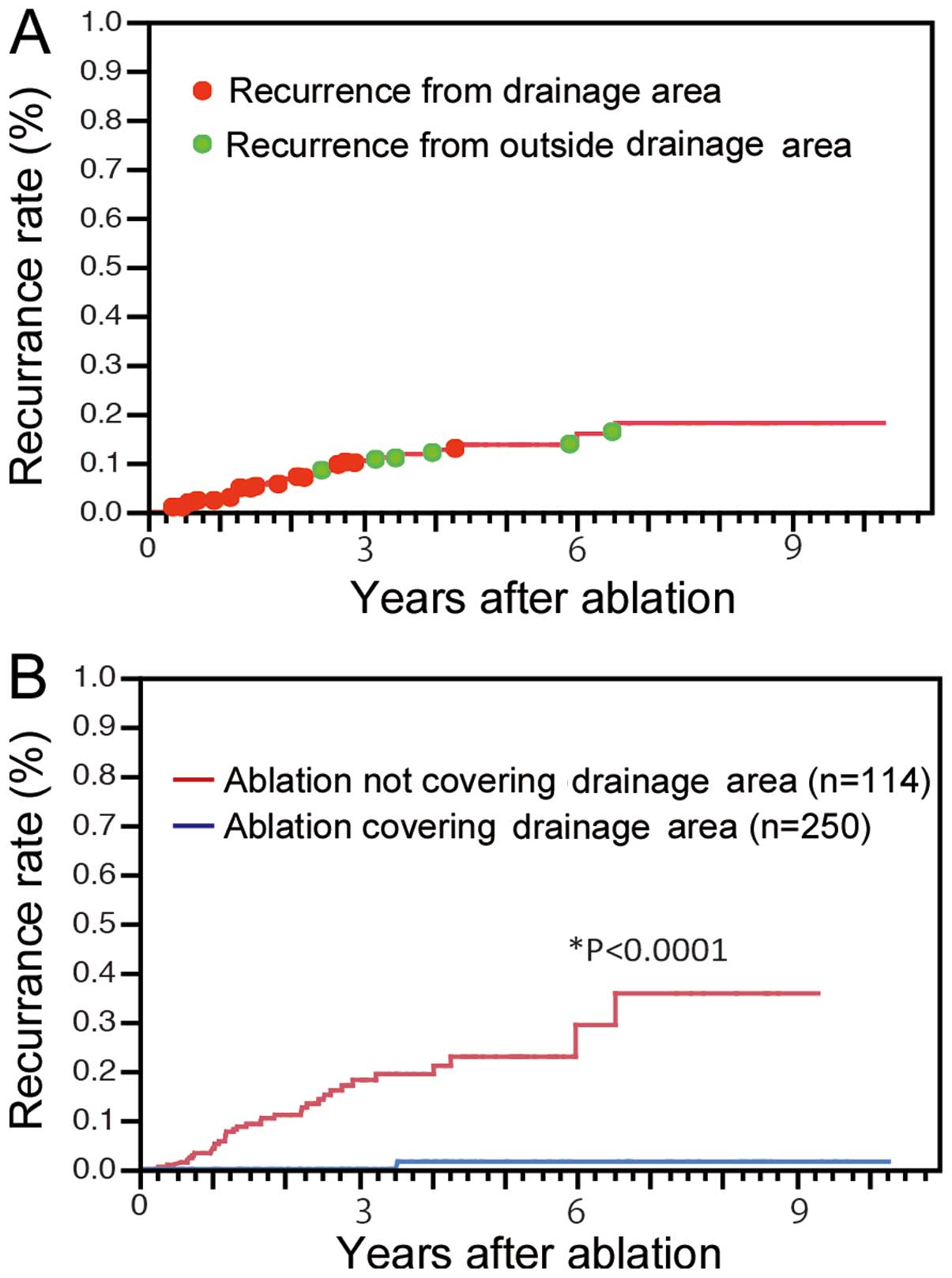
Recurrence
The cumulative local recurrence rates for all cases
were 2.2, 6.7 and 9.9% at 1, 2 and 3 years, respectively. Local
recurrence was detected in 30 cases from the drainage area and in 6
cases from outside the drainage area (Fig. 3A). The median time to recurrence
was 434 days (range, 170–959 days) for lesions in the drainage area
and 1,474 days (range, 815–2,383 days) for lesions outside the
drainage area (P=0.0037). Furthermore, the cumulative local
recurrence rates were 0, 0 and 1.5% at 1, 3 and 5 years,
respectively, for group A and 3.8, 17.0 and 22.8% at 1, 3 and 5
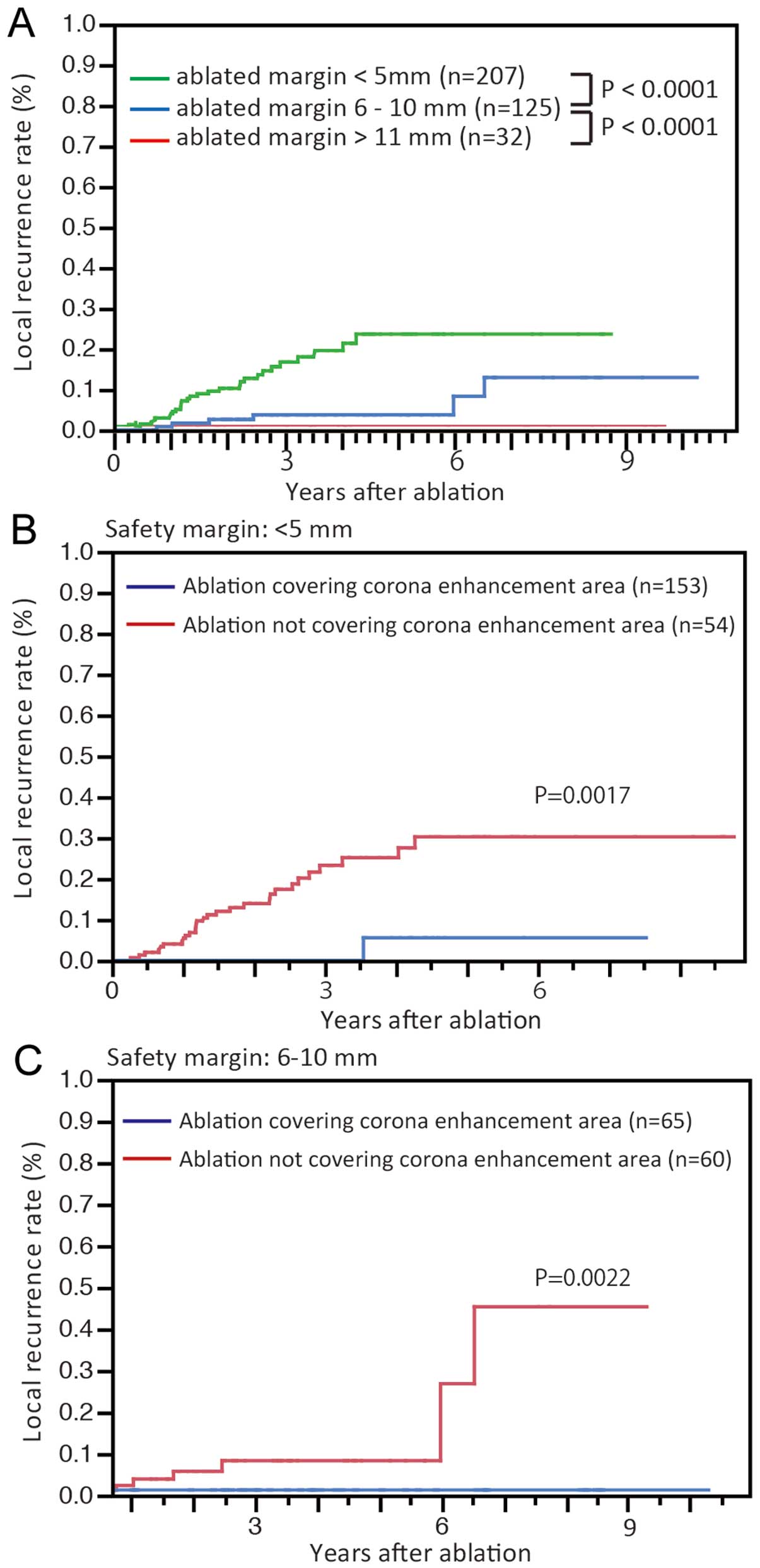
years, respectively, for group B (P<0.0001, Fig. 3B). As the width of the ablated
margin increased, the local recurrence rates were significantly
decreased (P<0.0001, Fig. 4A).
However, in cases without wide ablation margins (<5 mm), the
local recurrence rates for group A remained significantly low
(P=0.0017; Fig. 4B). Among the
cases in which sufficient ablation margins were achieved (6–10 mm),
group A nodules also exhibited low rates of local recurrence
(P=0.0022; Fig. 4C).
Discussion
In this study, the majority of local recurrences
occurred within the blood drainage area depicted as the area of
corona enhancement on CTHA. The prognosis for patients with local
recurrence within this region was relatively poor. Therefore,
treatment should be continued until the ablation area covers the
entire blood drainage area. If an adequate safety margin cannot be
achieved within the drainage area, a high risk of local recurrence
must be anticipated.
HCC often exhibits satellite lesions (19,24),
which cannot be diagnosed by imaging, due to their small size.
Previous studies reported satellite lesions located at a distance
from the main nodule (19,24). Various distances between the main
and satellite nodules were previously reported; therefore, the
ablated area may be determined based on those reports. Satellite
lesions were found to be located ≤2 mm from the main nodule in
66.7% and 2.1–5 mm in 11.1% of the cases (24). Okusaka et al (19) reported that, of the 149 resected
specimens, 28 (19%) exhibited satellite lesions, which were located
≤0.5 cm from the main tumor in 8 (33%), 0.6–1.0 cm in 12 (50%),
1.1–1.5 cm in 1 (4%) and 1.6–2.0 cm in 3 (13%) of the cases. A safe
margin was considered to be ≥5 mm (25). The present study also demonstrated
significantly lower local recurrence rates for nodules ablated with
wide safety margins (Fig. 4A).
However, cases with safety margins >5 mm but without ablation of
the entire blood drainage area often developed local recurrence
(Fig. 4C). Conversely, if a safety
margin >5 mm was not achieved, local recurrences were often not
seen (Fig. 4B). Thus, the
definition of safety margins should be determined using other
factors in addition to distance from the primary lesion. Corona
enhancement was recently proposed as reflecting the blood drainage
area. Kitao et al (22)
reported that intranodular capillarized sinusoids connect directly
or indirectly to extranodular portal veins through portal venules
within the fibrous septum. Sakon et al (20) reported that the high-risk area for
intrahepatic metastases in the blood drainage area was confirmed
from histopathological examination of the resected specimens.
Satellite nodules in the drainage area were also reported as
frequently being multiple moderately or poorly differentiated
carcinomas, consistent with the characteristics of intrahepatic
metastases. Furthermore, satellite nodules outside the drainage
area were commonly solitary foci of well-differentiated carcinoma,
suggestive of multicentric carcinogenesis. Those studies indicated
that the surgical margins differed in each case with respect to
tumor hemodynamics and, even in the same tumor, the width of safety
margins differed according to the location of the tumor within the
liver (20). The safety margin for
RFA should be considered in the same way as the surgical margins
for hepatectomy. Indeed, if the safety margin covered the entire
blood drainage area, local recurrence was rarely reported in our
study (Fig. 4).
Several limitations must be considered for this
study. First, unlike a previous report (20), the lack of histological examination
was problematic. Second, if the blood drainage area was >10 mm,
obtaining safety margins was difficult. For example, for an HCC
nodule diameter of >30 mm, an ablated area of >50 mm should
be obtained. In such cases, hepatectomy is warranted. If RFA is
performed, TACE should be used as well. Third, delayed-phase CTHA
was not performed at a single-slice level. Finally, fusion images
are not absolutely accurate for assessing safety margins. A slight
gap may be observed when images obtained on different days are
overlapped.
In conclusion, the safety margins for RFA should be
defined as the blood drainage area and ablation should be aimed at
acquiring adequate safety margins.
Abbreviations:
|
CTAP
|
computed tomography during arterial
portography
|
|
CTHA
|
computed tomography during hepatic
arteriography
|
|
ECOG
|
Eastern Cooperative Oncology Group
|
|
HCC
|
hepatocellular carcinoma
|
|
RFA
|
radiofrequency ablation
|
|
TACE
|
transcatheter arterial
chemoembolization
|
References
|
1
|
Mazzaferro V, Regalia E, Doci R, et al:
Liver transplantation for the treatment of small hepatocellular
carcinomas in patients with cirrhosis. N Engl J Med. 334:693–699.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Arii S, Yamaoka Y, Futagawa S, et al:
Results of surgical and nonsurgical treatment for small-sized
hepatocellular carcinomas: a retrospective and nationwide survey in
Japan. The Liver Cancer Study Group of Japan. Hepatology.
32:1224–1229. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ikai I, Itai Y, Okita K, et al: Report of
the 15th follow-up survey of primary liver cancer. Hepatol Res.
28:21–29. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Shiina S, Teratani T, Obi S, Hamamura K,
Koike Y and Omata M: Percutaneous ethanol injection therapy for
liver tumors. Eur J Ultrasound. 13:95–106. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Shiina S, Teratani T, Obi S, et al: A
randomized controlled trial of radiofrequency ablation with ethanol
injection for small hepatocellular carcinoma. Gastroenterology.
129:122–130. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Uehara T, Hirooka M, Ishida K, et al:
Percutaneous ultrasound-guided radiofrequency ablation of
hepatocellular carcinoma with artificially induced pleural effusion
and ascites. J Gastroenterol. 42:306–311. 2007. View Article : Google Scholar
|
|
7
|
Hirooka M, Iuchi H, Kumagi T, et al:
Virtual sonographic radiofrequency ablation of hepatocellular
carcinoma visualized on CT but not on conventional sonography. AJR
Am J Roentgenol. 186(Suppl 5): S255–S260. 2006. View Article : Google Scholar
|
|
8
|
Takayasu K, Arii S, Ikai I, et al:
Prospective cohort study of transarterial chemoembolization for
unresectable hepatocellular carcinoma in 8510 patients.
Gastroenterology. 131:461–469. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tateishi R, Shiina S, Teratani T, et al:
Percutaneous radiofrequency ablation for hepatocellular carcinoma.
An analysis of 1000 cases. Cancer. 103:1201–1209. 2005.PubMed/NCBI
|
|
10
|
Hiraoka A, Horiike N, Yamashita Y, et al:
Efficacy of radiofrequency ablation therapy compared to surgical
resection in 164 patients in Japan with single hepatocellular
carcinoma smaller than 3 cm, along with report of complications.
Hepatogastroenterology. 55:2171–2174. 2008.
|
|
11
|
Kim YS, Rhim H, Cho OK, Koh BH and Kim Y:
Intrahepatic recurrence after percutaneous radiofrequency ablation
of hepatocellular carcinoma: analysis of the pattern and risk
factors. Eur J Radiol. 59:432–441. 2006. View Article : Google Scholar
|
|
12
|
Choi D, Lim HK, Rhim H, et al:
Percutaneous radiofrequency ablation for early-stage hepatocellular
carcinoma as a first-line treatment: long-term results and
prognostic factors in a large single-institution series. Eur
Radiol. 17:684–692. 2007. View Article : Google Scholar
|
|
13
|
Hori T, Nagata K, Hasuike S, et al: Risk
factors for the local recurrence of hepatocellular carcinoma after
a single session of percutaneous radiofrequency ablation. J
Gastroenterol. 38:977–981. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kim SH, Lim HK, Choi D, et al:
Percutaneous radiofrequency ablation of hepatocellular carcinoma:
effect of histologic grade on therapeutic results. AJR Am J
Roentgenol. 186(Suppl 5): S327–S333. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Komorizono Y, Oketani M, Sako K, et al:
Risk factors for local recurrence of small hepatocellular carcinoma
tumors after a single session, single application of percutaneous
radiofrequency ablation. Cancer. 97:1253–1262. 2003. View Article : Google Scholar
|
|
16
|
Lencioni R, Cioni D, Crocetti L, et al:
Early-stage hepatocellular carcinoma in patients with cirrhosis:
long-term results of percutaneous image-guided radiofrequency
ablation. Radiology. 234:961–967. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Livraghi T, Meloni F, Di Stasi M, et al:
Sustained complete response and complications rates after
radiofrequency ablation of very early hepatocellular carcinoma in
cirrhosis: is resection still the treatment of choice? Hepatology.
47:82–89. 2008. View Article : Google Scholar
|
|
18
|
Nakazawa T, Kokubu S, Shibuya A, et al:
Radiofrequency ablation of hepatocellular carcinoma: correlation
between local tumor progression after ablation and ablative margin.
AJR Am J Roentgenol. 188:480–488. 2007. View Article : Google Scholar
|
|
19
|
Okusaka T, Okada S, Ueno H, et al:
Satellite lesions in patients with small hepatocellular carcinoma
with reference to clinicopathologic features. Cancer. 95:1931–1937.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sakon M, Nagano H, Nakamori S, et al:
Intrahepatic recurrences of hepatocellular carcinoma after
hepatectomy: analysis based on tumor hemodynamics. Arch Surg.
137:94–99. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hirooka M, Kisaka Y, Uehara T, et al:
Efficacy of laparoscopic radiofrequency ablation for hepatocellular
carcinoma compared to percutaneous radiofrequency ablation with
artificial ascites. Dig Endosc. 21:82–86. 2009. View Article : Google Scholar
|
|
22
|
Kitao A, Zen Y, Matsui O, Gabata T and
Nakanuma Y: Hepatocarcinogenesis: multistep changes of drainage
vessels at CT during arterial portography and hepatic arteriography
- radiologic-pathologic correlation. Radiology. 252:605–614. 2009.
View Article : Google Scholar
|
|
23
|
Kim YS, Lee WJ, Rhim H, Lim HK, Choi D and
Lee JY: The minimal ablative margin of radiofrequency ablation of
hepatocellular carcinoma (>2 and <5 cm) needed to prevent
local tumor progression: 3D quantitative assessment using CT image
fusion. AJR Am J Roentgenol. 195:758–765. 2010.
|
|
24
|
Nakashima Y, Nakashima O, Tanaka M, Okuda
K, Nakashima M and Kojiro M: Portal vein invasion and intrahepatic
micrometastasis in small hepatocellular carcinoma by gross type.
Hepatol Res. 26:142–147. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kudo M: Local ablation therapy for
hepatocellular carcinoma: current status and future perspectives. J
Gastroenterol. 39:205–214. 2004. View Article : Google Scholar : PubMed/NCBI
|