Introduction
Uterine sarcomas are extremely rare, non-epithelial
malignant uterine tumors. Uterine sarcomas account for 8% of all
malignant tumors of the corpus uteri and the most common
histological types are carcinosarcoma (CS), leiomyosarcoma (LMS)
and endometrial stromal sarcoma (ESS), in decreasing order of
frequency (1). In Japan, it was
reported that the most common histological types are CS (46%), LMS
(36%) and ESS (13%) (2). CS is a
malignant tumor consisting of an epithelial and a non-epithelial
component, which mainly affects postmenopausal women. A combination
tumor theory suggested that the majority of CSs originate from a
single cell and differentiate into epithelioid-like and
stromal-like components, whereas they are considered to exhibit
cellular characteristics and progression similar to those of poorly
differentiated endometrioid adenocarcinoma (3). Therefore, CSs tend to be treated in
accordance with the treatment for epithelial endometrial cancer.
However, LMS and ESS possess totally different properties compared
to epithelial endometrial cancer.
LMS and ESS are malignant tumors that are mainly
encountered during the perimenopausal period. Uterine leiomyomas
may exhibit malignant transformation to LMS in 0.13–0.81% of the
cases (4). These tumors are
diagnosed based on the number of mitoses, degree of cellular atypia
and presence of coagulation necrosis. ESS may be classified as low-
or high-grade, based on the number of mitoses. However, these
sarcomas are currently considered as different types of tumors.
High-grade ESS, in particular, is referred to as undifferentiated
endometrial sarcoma (UES). Total hysterectomy and bilateral
salpingo-oophorectomy (BSO) are currently considered the first
choice for the treatment of uterine sarcomas, although a consensus
has not been reached regarding retroperitoneal lymphadenectomy
(5,6). However, these tumors cannot be
sufficiently controlled by surgical treatment alone, since a number
of patients develop progression and recurrence of uterine sarcoma.
As LMS often develops distant hematogenous metastases to the lungs
and the liver, chemotherapy is commonly required as a systemic
treatment. However, there is insufficient evidence to recommend a
specific chemotherapeutic regimen as standard treatment for uterine
sarcomas, as these are rare tumors and the number of reported cases
is limited.
We administered a combination of ifosfamide (IFM),
adriamycin (ADM) and cisplatin (CDDP) (IAP therapy) to patients
with progressive and recurrent uterine sarcomas and retrospectively
investigated treatment effectiveness and toxicity.
Patients and methods
Patients
We investigated 11 patients who were diagnosed with
uterine sarcoma and treated with IAP between 1990 and 2010 at the
Keio University Hospital, Tokyo, Japan.
Total hysterectomy and BSO or tumorectomy were
performed in our hospital. The pathological diagnosis in all the
cases was LMS, UES or adenosarcoma. The median follow-up period was
298 days (range, 36–2,757 days). Remission induction chemotherapy
was performed in all the cases, as 8 of the patients had
progressive disease (PD) and 3 patients had recurrent disease.
This study was approved by the Keio University
School of Medicine Ethics Committee (approval no. 20120236) and all
the patients provided informed consent.
Treatment plan
The treatment schedule was based on a case report of
uterine sarcoma that was treated with IAP (7,8). The
administration was every 3 weeks as follows: IFM 1.5 g/body on days
1–5, mesna 900 mg/body on days 1–5, ADM 50 mg/m2 on day
1 and CDDP 50 mg/m2 on day 1, intravenously. Granulocyte
colony-stimulating factor (G-CSF) was used according to the
criteria of the American Society of Clinical Oncology. This
treatment schedule was repeated every 3 weeks until disease
progression or until discontinuation due to adverse events.
Evaluation of response and toxicity
The adverse events were assessed according to the
Common Terminology Criteria for Adverse Events, version 4.0, based
on the interviews and blood tests conducted once a week or more
frequently after each cycle. The subsequent cycle was initiated
after the adverse events were resolved. As regards hematotoxicity,
if patients presented with grade 4 leukopenia or neutropenia for
>7 days, grade 3–4 thrombocytopenia, or febrile neutropenia, we
considered reducing the dose or withdrawing drugs for the
subsequent cycle.
We assessed the overall response rate of 11 cases
who had received remission induction therapy and had evaluable
lesions in accordance with the World Health Organization evaluation
criteria and recorded the progression-free survival. The tumors
were measured by computed tomography after every 2 cycles. After
the product of the two longest perpendicular diameters was
calculated, the response was assessed as follows: complete response
(CR), complete disappearance of all known lesions for a minimum of
4 weeks; partial response (PR), >50% reduction in the sum of the
length × width of each measurable lesion for a minimum of 4 weeks;
PD, >25% increase in the sum of the products of all measurable
lesions or appearance of any new lesions; no change (NC), any
outcome that did not qualify as response or progression.
Statistical analysis
SPSS software, version 20 (IBM-SPSS Software,
Chicago, IL, USA) was used for statistical analysis, using Fisher’s
exact test. P<0.05 was considered to indicate a statistically
significant difference. Kaplan-Meier curves were used for the
estimation of progression-free survival and were compared with
standard log-rank tests.
Results
Clinicopathological characteristics
The clinicopathological characteristics of the 11
cases who underwent IAP therapy are presented in Tables I and II. The median age at IAP therapy was 50
years (range, 34–72 years). The primary tumor sites were the uterus
(10 cases, 90.9%) or the retroperitoneum (1 case, 9.1%). The
histological types were LMS (6 cases, 54.5%), adenosarcoma (3
cases, 27.3%) and UES (high-grade ESS; 2 cases, 18.2%).
 | Table IClinicopathological characteristics of
the 11 cases. |
Table I
Clinicopathological characteristics of
the 11 cases.
| Characteristics | No. |
|---|
| Age (years) |
| <50 | 5 |
| ≥50 | 6 |
| Origin |
| Uterus | 10 |
| Retroperitoneum | 1 |
| Histological
type |
| Leiomyosarcoma | 6 |
| Adenosarcoma | 3 |
| Undifferentiated
endometrial sarcoma | 2 |
| Stage (FIGO
1988) |
| I | 4 |
| II | 0 |
| III | 1 |
| IV | 5 |
| Other | 1 |
| Type of disease |
| Progressive | 6 |
| Recurrent | 5 |
| Initial
treatment |
| Surgery | 11 |
| Chemotherapy | 0 |
| Type of surgery |
| Hysterectomy + BSO
(USO) | 7 |
| Other | 4 |
| Chemotherapy prior to
IAPa |
| None | 9 |
| CYVADICb | 1 |
| DOC + GEM | 1 |
| Table IIClinicopathological and treatment
details of the 11 cases. |
Table II
Clinicopathological and treatment
details of the 11 cases.
| Age at diagnosis
(years) | Age at IAPa therapy (years) | Histological
type | Disease status | Initial
treatment | Prior
chemotherapy | No. of cycles | Effectiveness | Recurrence after
IAPa therapy | PFS (days) |
|---|
| 33 | 34 | Leiomyosarcoma | Recurrent | ATH + BSO | CYVADICb | 8 | SD | Yes | 1,321 |
| 67 | 72 | Adenosarcoma | Recurrent | ATH + BSO | - | 2 | SD | No | - |
| 51 | 51 | Leiomyosarcoma | Recurrent | Tumorectomy +
BSO | - | 3 | CR | Yes | 213 |
| 62 | 62 | Leiomyosarcoma | Progressive | Tumorectomy | - | 8 | SD | Yes | 125 |
| 57 | 56 | ESS, high-grade | Progressive | Virchow LN
biopsy | - | 1 | SD | Yes | 307 |
| 43 | 43 | Adenosarcoma | Progressive | ATH + BSO + PLN + OMT
+ tumorectomy | - | 6 | SD | Yes | 44 |
| 50 | 50 | ESS, high-grade | Progressive | ATH + BSO | - | 2 | SD | Unknown | - |
| 40 | 40 | Leiomyosarcoma | Progressive | ATH + BSO + PLN +
tumorectomy | - | 8 | PD | Yes | 25 |
| 38 | 39 | Adenosarcoma | Progressive | ATH +
tumorectomy | - | 6 | PR | Yes | 80 |
| 35 | 35 | Leiomyosarcoma | Progressive | ATH + BSO | DOC + GEM | 6 | CR | No | - |
| 56 | 57 | Leiomyosarcoma | Progressive | Tumorectomy | - | 6 | CR | Yes | 1,539 |
Treatment
A total of 2 cases (18.2%) had received
pretreatment; 1 case had received cyclophosphamide, vincristine,
ADM and dacarbazine (DTIC) (CYVADIC therapy) and 1 case had
received docetaxel (DOC) + gemcitabine (GEM).
The median number of cycles of IAP therapy was 6
(range, 1–8 cycles). In 72.7% of the cases, a dose reduction was
required. Among cases who received >6 cycles, in particular,
71.4% required a dose reduction. The chemotherapy was interrupted
after 1 to 2 cycles for the patients who requested treatment
discontinuation due to intolerable adverse events.
Adverse events
The adverse events of IAP therapy are summarized in
Table III. Hematotoxicity,
particularly grade ≥3 leukopenia or neutropenia, developed in all
the cases during the first cycle. Febrile neutropenia developed in
45.5% of the cases and resolved with administration of antibiotics
and G-CSF. Grade 4 thrombopenia developed in 3 cases (27.3%), one
of which required a platelet transfusion. Non-hematological adverse
events other than anorexia, nausea and vomiting were not reported.
Hemorrhagic cystitis or cardiotoxicity, which are adverse events
characteristic of IFM and ADM, were also not reported.
| Table IIIAdverse events following IAPa therapy. |
Table III
Adverse events following IAPa therapy.
| Adverse events | Grade | N | % |
|---|
| Hematological |
| Leukopenia | 3 | 2 | 18.2 |
| 4 | 9 | 81.8 |
| Neutropenia | 3 | 2 | 18.2 |
| 4 | 9 | 81.8 |
| Febrile
neutropenia | 3 | 5 | 45.5 |
|
Thrombocytopenia | 4 | 3 | 27.3 |
|
Non-hematological | 3 | 0 | 0 |
| 4 | 0 | 0 |
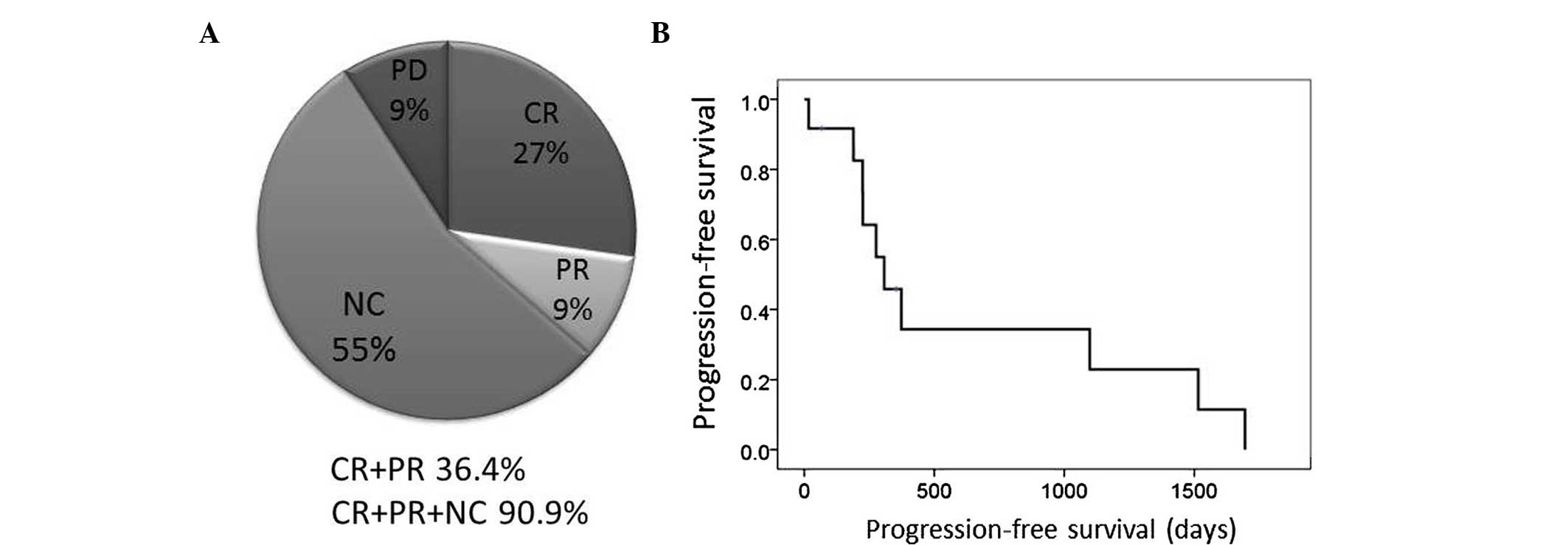
Effectiveness
The therapeutic effects of remission induction
chemotherapy are presented in Fig.
1. The sum of CR + PR was 36.4% (95% CI: 8.0–64.8%) and that of
CR + PR + NC was 90.9% (95% CI: 73.9–100%). The median
progression-free survival was 307 days (95% CI: 168–446 days).
Discussion
Although several chemotherapeutic options for
uterine sarcoma were previously suggested, the number of
large-scale studies on uterine sarcomas is limited, as this type of
tumor is relatively rare. The overall rate of response to
single-agent chemotherapy is presented in Table IV. The response rate for ADM, IFM
and gemcitabine (GEM) was 25.0, 17.0 and 21.0%, respectively
(9–11); these are considered to be the key
drugs in the treatment of uterine sarcoma. However, the response
rate with paclitaxel and CDDP was 9.0 and 3.0%, respectively
(12,13); thus, these drugs are considered to
be less effective.
| Table IVOverall rate of response to
single-agent chemotherapy. |
Table IV
Overall rate of response to
single-agent chemotherapy.
| Agents | Dose and
regimen | Response rate
(%) | First author | Refs. |
|---|
| ADM | 60 mg/m2
day 1 | 25 | Omura | (9) |
| Etoposide | 100
mg/m2 day 1–3 | 11 | Slayton | (19) |
| CDDP | 50 mg/m2
day 1 | 3 | Thigpen | (13) |
| Ifosfamide | 1.5 g/m2
day 1–5 | 17 | Sutton | (10) |
| Paclitaxel | 175
mg/m2 day 1 | 9 | Sutton | (12) |
| Gemcitabine | 50 mg/m2
day 1, 8 and 15 | 21 | Look | (11) |
| Liposomal
doxorubicin | 50 mg/m2
day 1 | 14 | Sutton | (20) |
| Topotecan | 1.5
mg/m2 day 1–5 | 11 | Miller | (21) |
| Trabectedin | 1.5
mg/m2 day 1 | 10 | Monk | (22) |
The efficiency of multi-agent chemotherapy for
uterine sarcoma is summarized in Table
V. Omura et al (9)
investigated the efficiency of ADM + DTIC therapy and reported
that, among 66 cases with measurable lesions of uterine sarcoma, 16
(24.2%) achieved a remission (CR + PR). Specifically, the response
rate was 30.0% (6/20) in cases with LMS.
| Table VOverall rate of response to
multi-agent chemotherapy. |
Table V
Overall rate of response to
multi-agent chemotherapy.
| Agents | Dose and
regimen | Cases | Response rate
(%) | Disease control
rate (%) | First author | Refs. |
|---|
| ADM + DTIC | ADM 60
mg/m2 day 1
DTIC 250 mg/m2 days 1–5 | 20 | 30.0 | | Omura | (9) |
| IFM + ADM | IFM 5
g/m2 day 1
ADM 50 mg/m2 day 3 | 33 | 30.3 | 81.8 | Sutton | (14) |
| CYVADIC | CPA 400
mg/m2 day 2
Vicristine 1 mg/m2 days 1–5
ADM 40 mg/m2 day 2
DTIC 200 mg/m2 days 1–5 | 10 | 20.0 | 60.0 | Piver | (15) |
| GEM + DOC | GEM 900
mg/m2 day 1
DOC 100 mg/m2 days 1 and 8 | 42 | 35.8 | 62.0 | Hensley | (16,17) |
| MAID | Mesna 1.5
g/m2 days 1–4
IFM 1.5 g/m2 days 1–3
ADM 15 mg/m2 days 1–3
DTIC 250 mg/m2 days 1–5 | 6 | 33.3 | 50.0 | Pearl | (18) |
| IAP | IFM 1.5 g/body days
1–5
ADM 50 mg/m2 day 1
CDDP 50 mg/m2 day 1 | 11 | 36.4 | 90.9 | Present study | |
Sutton et al (14) investigated ADM + IFM therapy in 33
patients with LMS. As regards adverse events, grade >3
neutropenia developed in 17 cases (48.6%), of which 2 developed
febrile neutropenia. Grade ≥3 thrombocytopenia was observed in 2
cases and nephrotoxicity in 1 case. There were 2 reported deaths
due to the development of severe adverse events, specifically
sepsis and cardiotoxicity. CR was achieved in 1 case and PR in 9
cases. The overall response rate was 30.3% and the disease control
rate (CR + PR + SD) was 82.0%.
Piver et al (15) investigated CYVADIC therapy in 26
patients with intrapelvic sarcoma. As regards adverse events,
neurotoxicity was observed in 8 cases (30.7%), including 6
mild-to-moderate and 2 severe cases. No patient developed
cardiotoxicity. However, sepsis developed in 4 cases (15.3%) and 1
patient succumbed to the complications. The effectiveness was
determined in 10 uterine sarcoma cases. The overall response rate
and disease control rate were 20.0 and 60.0%, respectively.
Hensley et al (16,17)
investigated docetaxel (DOC) + GEM therapy in 42 patients with
uterine LMS. The adverse events were grade ≥3 neutropenia in 17.0%,
grade ≥3 anemia in 24.0% and grade ≥ thrombocytopenia in 14.5% of
the cases. Grade 3 allergic reactions and grade 4 pulmonary
toxicity developed in all the patients. As regards effectiveness,
the overall response rate was 35.8% and the disease control rate
was 62.0%.
Pearl et al (18) investigated MAID therapy in 23
patients with gynecological sarcoma, including uterine LMS and
adenosarcoma. The overall response rate was 33.3% and the disease
control rate was 50.0%.
The number of studies on IAP therapy for uterine
sarcoma is currently limited. Yamawaki et al (6) reported that IAP was effective in a
case with progressive UES. Yamaguchi et al (23) also reported that the rate of PR
with IAP therapy for uterine sarcomas was 40.0% in the first-line
and 9.1% in the second-line chemotherapy setting.
In this study, IAP therapy achieved an overall
response rate of 36.4% and a disease control rate, including NC, of
90.9%. Our results were comparable to those of IFM + ADM or DOC +
GEM therapy. The adverse events recorded in the present study were
mainly hematological, with grade ≥3 leukopenia and neutropenia in
all the cases. However, these adverse events were manageable with
dose reduction and G-CSF administration for severe hematotoxicity.
Only one patient experienced severe thrombocytopenia requiring
platelet transfusion. The median number of administered cycles was
6. There were no severe non-hematological complications or
treatment-related deaths in the present study.
In conclusion, taking into consideration the
abovementioned findings, IAP therapy may be a feasible
chemotherapeutic option for progressive or recurrent uterine
sarcoma.
Acknowledgements
The authors would like to thank Ms. Keiko Abe and
Ms. Tomomi Noda for their secretarial assistance.
References
|
1
|
Brooks SE, Zhan M, Cote T and Baquet CR:
Surveillance, epidemiology, and end results analysis of 2,677 cases
of uterine sarcoma 1989–1999. Gynecol Oncol. 93:204–208. 2004.
|
|
2
|
Fujita H, Adachi S, Kigawa J, et al:
Clinicopathological analysis for uterine sarcoma. Sampu no shimpo.
56:463–465. 2004.(In Japanese).
|
|
3
|
Wada H, Enomoto T, Fujita M, et al:
Molecular evidence that most but not all carcinosarcomas of the
uterus are combination tumors. Cancer Res. 57:5379–5385.
1997.PubMed/NCBI
|
|
4
|
Lurain JR: Uterine cancer. Berek &
Novak’s Gynecology. Berek JS: 14th edition. Lippincott Williams
& Wilkins; Philadelphia: pp. 1343–1402. 2006
|
|
5
|
Goff BA, Rice LW, Fleischhacker D, et al:
Uterine leiomyosarcoma and endometrial stromal sarcoma: lymph node
metastases and sites of recurrence. Gynecol Oncol. 50:105–109.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sagae S, Yamashita K, Ishioka S, et al:
Preoperative diagnosis and treatment results in 106 patients with
uterine sarcoma in Hokkaido, Japan. Oncology. 67:33–39. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ushijima M, Yamakawa Y, Sakabe E, et al: A
case of recurrent high-grade endometrial stromal sarcoma controlled
by a combination of ifosfamide, adriamycin, and cisplatin. Jpn J
Canc Chemother. 37:2003–2005. 2010.(In Japanese).
|
|
8
|
Yamawaki T, Shimizu Y and Hasumi K:
Treatment of stage IV ‘high-grade’ endometrial stromal sarcoma with
ifosfamide, adriamycin, and cisplatin. Gynecol Oncol. 64:265–269.
1997.
|
|
9
|
Omura GA, Major FJ, Blessing JA, et al: A
randomized study of adriamycin with and without dimethyl
triazenoimidazole carboxamide in advanced uterine sarcomas. Cancer.
52:626–632. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sutton GP, Blessing JA, Manetta A, et al:
Gynecologic Oncology Group studies with ifosfamide. Semin Oncol.
19:31–34. 1992.PubMed/NCBI
|
|
11
|
Look KY, Sandler A, Blessing JA, Lucci JA
III and Rose PG; Gynecologic Oncology Group (GOG). Phase II trial
of gemcitabine as second-line chemotherapy of uterine
leiomyosarcoma: a Gynecologic Oncology Group (GOG) study. Gynecol
Oncol. 92:644–647. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sutton G, Blessing JA and Ball H: Phase II
trial of paclitaxel in leiomyosarcoma of the uterus: a Gynecologic
Oncology Group study. Gynecol Oncol. 74:346–349. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Thigpen JT, Blessing JA, Beecham J,
Homesley H and Yordan E: Phase II trial of cisplatin as first-line
chemotherapy in patients with advanced or recurrent uterine
sarcomas: a Gynecologic Oncology Group study. J Clin Oncol.
9:1962–1966. 1991.PubMed/NCBI
|
|
14
|
Sutton G, Blessing JA and Malfetano JH:
Ifosfamide and doxorubicin in the treatment of advanced
leiomyosarcomas of the uterus: a Gynecologic Oncology Group study.
Gynecol Oncol. 62:226–229. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Piver MS, DeEulis TG, Lele SB and Barlow
JJ: Cyclophosphamide, vincristine, adriamycin, and
dimethyl-triazeno imidazole carboxamide (CYVADIC) for sarcomas of
the female genital tract. Gynecol Oncol. 14:319–323. 1982.
View Article : Google Scholar
|
|
16
|
Hensley ML, Blessing JA, Degeest K, et al:
Fixed-dose rate gemcitabine plus docetaxel as second-line therapy
for metastatic uterine leiomyosarcoma: a Gynecologic Oncology Group
phase II study. Gynecol Oncol. 109:323–328. 2008. View Article : Google Scholar
|
|
17
|
Hensley ML, Blessing JA, Mannel R and Rose
PG: Fixed-dose rate gemcitabine plus docetaxel as first-line
therapy for metastatic uterine leiomyosarcoma: a Gynecologic
Oncology Group phase II trial. Gynecol Oncol. 109:329–334. 2008.
View Article : Google Scholar
|
|
18
|
Pearl ML, Inagami M, McCauley DL, et al:
Mesna, doxorubicin, ifosfamide, and dacarbazine (MAID) chemotherapy
for gynecological sarcomas. Int J Gynecol Cancer. 12:745–748. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Slayton RE, Blessing JA, Angel C and
Berman M: Phase II trial of etoposide in the management of advanced
and recurrent leiomyosarcoma of the uterus: a Gynecologic Oncology
Group Study. Cancer Treat Rep. 71:1303–1304. 1987.
|
|
20
|
Sutton G, Blessing J, Hanjani P and Kramer
P; Gynecologic Oncology Group. Phase II evaluation of liposomal
doxorubicin (Doxil) in recurrent or advanced leiomyosarcoma of the
uterus: a Gynecologic Oncology Group study. Gynecol Oncol.
96:749–752. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Miller DS, Blessing JA, Kilgore LC, Mannel
R and Van Le L: Phase II trial of topotecan in patients with
advanced, persistent, or recurrent uterine leiomyosarcomas: a
Gynecologic Oncology Group study. Am J Clin Oncol. 23:355–357.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Monk BJ, Blessing JA, Street DG, et al: A
phase II evaluation of trabectedin in the treatment of advanced,
persistent, or recurrent uterine leiomyosarcoma: a Gynecologic
Oncology Group study. Gynecol Oncol. 124:48–52. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yamaguchi M, Yanase T, Yokoo T, et al:
Clinical study and treatment of uterine sarcoma at Niigata City
General Hospital. Jpn J Canc Chemother. 31:209–213. 2004.(In
Japanese).
|