Introduction
Colorectal cancer (CRC) is the second most commonly
diagnosed type of cancer in females and the third in males
worldwide, with an estimated >1.2 million new cancer cases and
608,700 deaths in 2008 (1). While
colon cancer (CC) and rectal cancer (RC) are often referred to as
CRC due to their adjacent anatomic location, several studies
investigating risk factors to underlying molecular mechanisms, have
reported differences between CC and RC.
Dietary risk factors appeared to be considerably
different between CC and RC (2)
and the Cancer Genome Atlas Network reported differences between
tumors located in the right colon and all other sites (3). Whether CC and RC are of a markedly
different nature has not been clearly determined and the number of
clinical studies that have emphasized the differences between CC
and RC is currently limited.
Several tumor markers, including carcinoembryonic
antigen (CEA), carbohydrate antigen (CA) 19.9 and CA 12.5, have
been detected in a number of malignancies, including CRC. The
levels of CEA and CA19.9 are often elevated in advanced CRC
(4) and have been considered as an
early sign of CRC recurrence (5).
CEA, originally identified in human fetal intestine
and adult CC tissue in 1965 by Gold and Freedman (6), was subsequently characterized as a
glycosylated cell-surface glycoprotein with a molecular weight of
180,000 Da (7); further research
identified it as a significant tumor-associated antigen that is
highly overexpressed in breast, lung and pancreatic cancer and,
particularly, in CRC (8,9). CEA is routinely detected as a tumor
biomarker and an auxiliary indicator for the preoperative diagnosis
of CRC (10), as well as an early
predictor of recurrence (5), which
to some extent accounts for CEA reflecting the nature of CRC.
As there are currently few available studies
reporting the variations in the expression of CEA between CC and
RC, the present study aimed to investigate the possible differences
in the serum CEA level between CC and RC, which may highlight the
distinct natures of these two types of cancer.
Materials and methods
Serum CEA concentrations
A total of 240 cases were investigated between July,
2010 and July, 2012 from The First and Second Affiliated Hospitals
of Dalian Medical University, including 117 CC and 123 RC patients.
The patients underwent potentially curative resection of colorectal
carcinomas, which were classified as Duke’s stage A-C and patients
diagnosed as stage D were classified by biopsy or radiographic
findings (endorectal ultrasound, computed tomography and magnetic
resonance imaging). The disease stage was determined according to
the Dukes’ staging system, which is equivalent to the TNM staging
system of the American Joint Committee on Cancer (11). All the clinical findings were
prospectively recorded in detail and stored in computerized files,
which included name, gender, age, family history, CEA level and the
location and stage of the tumors.
The serum CEA concentrations were measured
preoperatively in the 240 patients by radioimmunoassays performed
in the clinical laboratories of the two affiliated hospitals. CEA
kits from Roche Diagnostics (Basel, Switzerland) were used for
detection following the manufacturer’s instructions. High CEA
concentrations were redefined as those >5 ng/ml.
Statistical analysis
In the present study, all the data were included in
the analysis and are expressed as means ± SD. Statistical
significance was calculated using the non-parametric t-test and
differences were considered to be statistically significant when
P<0.05.
Results
Clinicopathological characteristics of
CRC patients
A total of 240 patients with primary CRC (mean age,
62.0±12.3 years; range, 33–89 years), including 117 CC patients
(mean age, 62.5±12.5 years; range, 33–89 years) and 123 RC patients
(mean age, 61.4±12.1 years; range, 34–86 years), were recruited for
this study. The Duke’s stage and other relevant information are
summarized in Table I.
 | Table IClinicopathological characteristics in
colon and rectal cancer patients. |
Table I
Clinicopathological characteristics in
colon and rectal cancer patients.
| Total (n=240)* | Colon (n=117)* | Rectum
(n=123)* |
|---|
|
|
|
|
|---|
| Characteristics | No. (%) | No. (%) | No. (%) |
|---|
| Gender |
| Male | 139 (57.9) | 68 (58.1) | 71 (57.7) |
| Female | 101 (42.1) | 49 (41.9) | 52 (42.3) |
| Age, years |
| ≤50 | 45 (18.8) | 19 (16.2) | 26 (21.1) |
| >50 | 195 (81.2) | 98 (83.8) | 97 (78.9) |
| Duke’s stage |
| A | 57 (23.8) | 29 (24.8) | 28 (22.8) |
| B | 58 (24.2) | 31 (26.5) | 27 (21.9) |
| C | 60 (25.0) | 29 (24.8) | 31 (25.2) |
| D | 65 (26.1) | 28 (23.9) | 37 (30.1) |
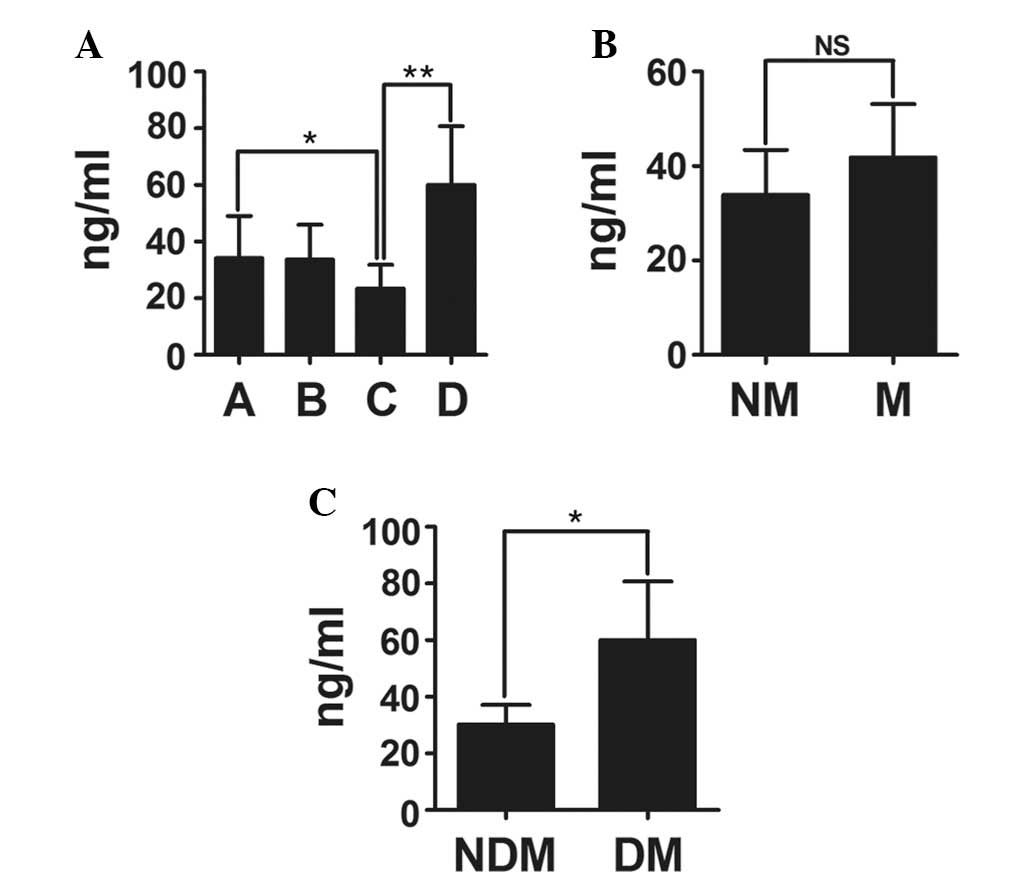
Lower CEA level in stage C of CRC differs
from that in other stages
The mean value of CEA in patients with CRC in stage
A, B, C and D were 34.14, 33.66, 23.35 and 60.05 ng/ml,
respectively. Of note, the CEA level in patients with CRC at stage
C was lower compared to that in any of the other stages, with
significant differences from stages A and D (Fig. 1), indicating the significance of
stage C, which contrasts the previous hypotheses that CEA levels
increased with advancing stage (12,13).
Additionally, the CEA level of the non-distant metastasis (NDM)
group was different from that in the distant metastasis (DM) group,
whereas no differences were observed between the non-metastasis
(NM) and metastasis (M) groups. An analysis of other factors, such
as patient gender and age, revealed no statistically significant
differences (Table II).
| Table IIDifferences in the serum
carcinoembryonic antigen level among patients with colorectal
cancer. |
Table II
Differences in the serum
carcinoembryonic antigen level among patients with colorectal
cancer.
| Variables | Mean, ng/ml | P-value |
|---|
| Duke’s stage |
| A/B | 34.14/33.66 | 0.3508 |
| A/D | 34.14/60.05 | 0.3967 |
| B/C | 33.66/23.35 | 0.2577 |
| B/D | 33.66/60.05 | 0.0711 |
| Gender |
| Male/female | 29.47/49.70 | 0.9735 |
| Age, years |
| ≤50/>50 | 10.90/43.95 | 0.0509 |
CC and RC are generally considered to be of the same
nature due to their neighbouring anatomical position. Therefore,
the indices of CC and RC are analyzed considering these two types
of cancer as a singe entity. In order to investigate the hypothesis
that CC and RC may be of different natures, possibly reflected by
the differences in the serum CEA level among different stages of
CRC (Fig. 1), we divided the cases
into two groups and analyzed them accordingly.
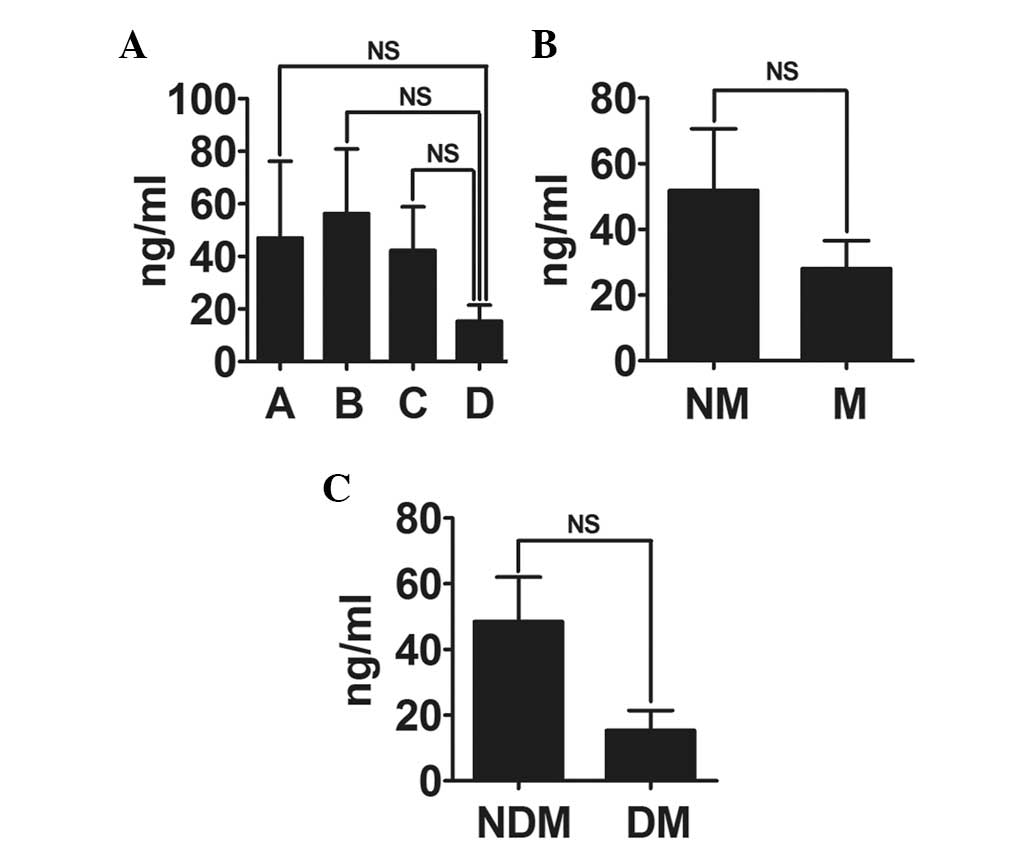
Significant differences in serum CEA
level are observed among the four stages of CC, but not RC
The mean values of CEA in patients with CC of stage
A, B, C and D were 21.25, 12.37, 4.96 and 113.40 ng/ml,
respectively (Table III),
whereas those in RC patients were 47.04, 56.28, 42.29 and 15.34
ng/ml, respectively (Table IV).
The statistical analysis revealed that CC exhibited a more
significant variation among the four stages (Fig. 2) compared to that in the RC group
(Fig. 3). No differences were
observed between male and female patients and between patients aged
<50 and >50 years regarding the distribution of serum CEA
levels.
| Table IIIDifferences in the serum
carcinoembryonic antigen level among patients with colon
cancer. |
Table III
Differences in the serum
carcinoembryonic antigen level among patients with colon
cancer.
| Variables | Mean, ng/ml | P-value |
|---|
| Duke’s stage |
| A/B | 21.25/12.37 | 0.0634 |
| A/D | 21.25/113.40 | 0.0506 |
| B/C | 12.37/4.96 | 0.1792 |
| Gender |
| Male/female | 34.16/40.26 | 0.6475 |
| Age, years |
| ≤50/>50 | 9.731/42.02 | 0.3259 |
| Table IVDifferences in the serum
carcinoembryonic antigen level among patients with rectal
cancer. |
Table IV
Differences in the serum
carcinoembryonic antigen level among patients with rectal
cancer.
| Variables | Mean, ng/ml | P-value |
|---|
| Duke’s stage |
| A/B | 47.04/56.28 | 0.6420 |
| A/C | 47.04/42.29 | 0.7360 |
| A/D | 47.04/15.34 | 0.6140 |
| B/C | 56.28/42.29 | 0.5951 |
| B/D | 56.28/15.34 | 0.3007 |
| C/D | 42.29/15.34 | 0.8738 |
| AB/CD | 51.80/28.05 | 0.3801 |
| ABC/D | 48.50/15.34 | 0.4766 |
| Gender |
| Male/female | 24.97/59.13 | 0.6279 |
| Age, years |
| ≤50/>50 | 11.85/45.92 | 0.0771 |
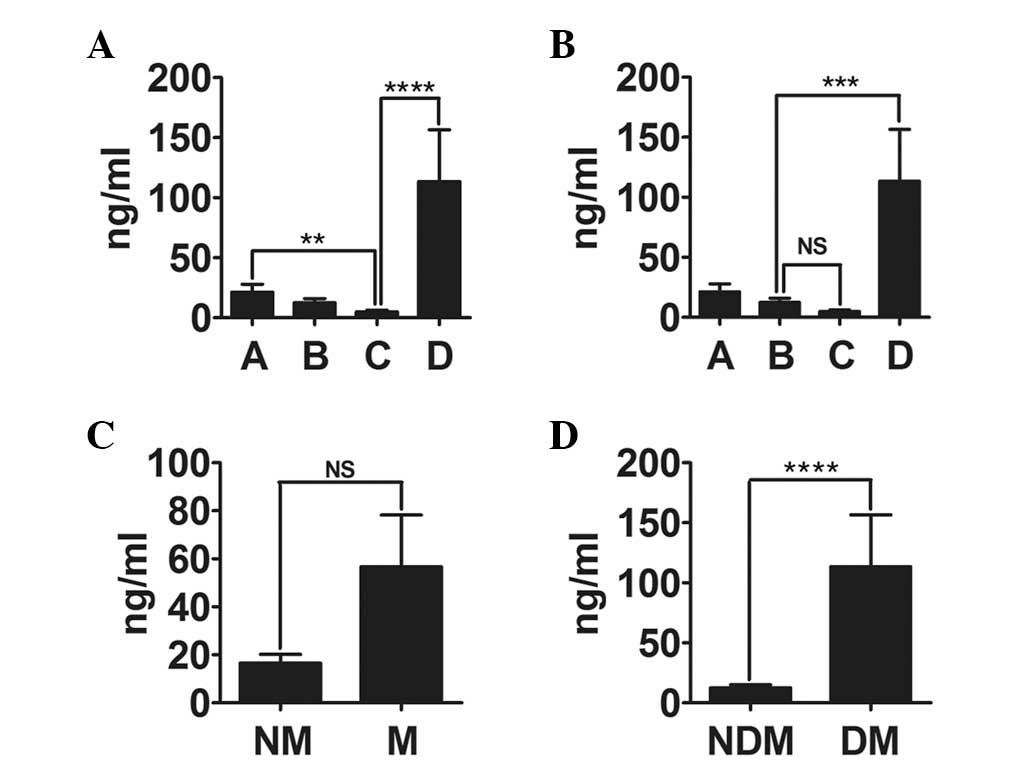
Serum CEA level is the lowest in stage C
of CC
Similar to the tendency reported for CRC, the CEA
value in stage C of CC (4.96 ng/ml) was lower compared to that in
stages A (21.25 ng/ml) and D (113.40 ng/ml). Of note, the CEA level
was the lowest in stage C with a significant difference from stages
A (P=0.0031) and D (P<0.0001), as shown in Fig. 2A. A significant difference was also
observed between stages B and D (P=0.0004; Fig. 2B), whereas no significant
difference was observed between stages B and C (P=0.3216).
Additionally, due to the high CEA level in stage D coexisting with
the lower CEA level in stages A, B and C, a significant difference
was also observed between the NDM and DM groups (P<0.0001;
Fig. 2D). However, no difference
was observed between the NM and M groups (P=0.5781; Fig. 2C). There were no differences among
other factors, such as patient gender and age (Table III).
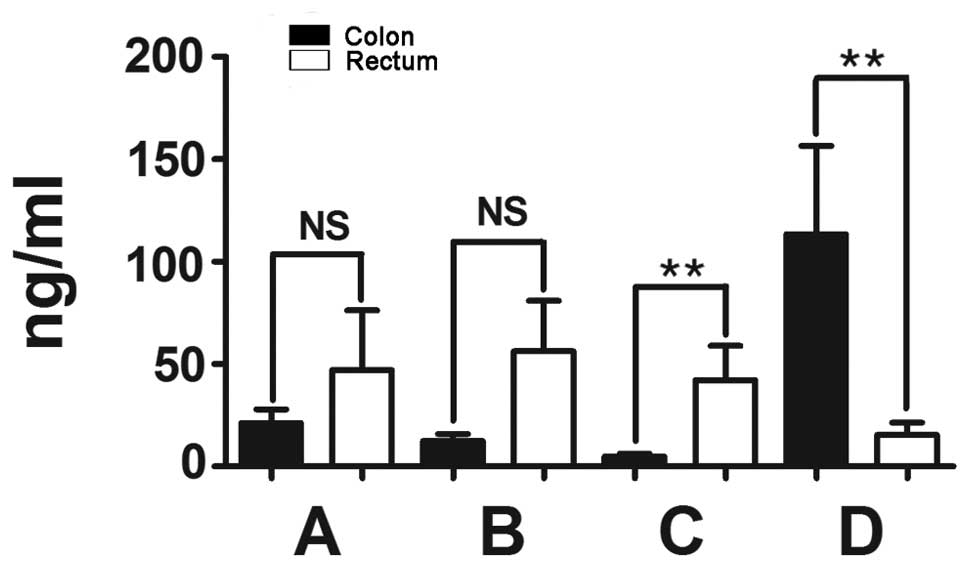
Significant differences in the serum CEA
level are observed in stages C and D between CC and RC
As described above, the different variation
tendencies of the serum CEA level between CC and RC prompted the
comparison of the CEA level in the four stages between CC and RC.
The results revealed no differences in the CEA levels in stage A
(P=0.9764), or in stage B (P=0.1221) between CC and RC (Table V). However, the CEA level in stage
C of CC was lower compared to that in stage C of RC, with a
significant difference (P=0.0096); the difference between stage D
of CC and RC was also significant (P=0.0063) (Fig. 4). There were also differences in
the CEA level in the NDM group between CC and RC (P=0.0155),
whereas there were no differences in the other factors shown in
Table V.
| Table VDifferences in the serum
carcinoembryonic antigen level between patients with colon and
rectal cancer. |
Table V
Differences in the serum
carcinoembryonic antigen level between patients with colon and
rectal cancer.
| Mean (ng/ml) | |
|---|
|
| |
|---|
| Variables | Colon | Rectum | P-value |
|---|
| Duke’s stage |
| A | 21.25 | 47.04 | 0.9764 |
| B | 12.37 | 56.28 | 0.1221 |
| AB | 16.53 | 51.80 | 0.2465 |
| CD | 56.68 | 28.05 | 0.8897 |
| ABC | 12.52 | 48.50 | 0.0155 |
| ABCD | 36.76 | 39.21 | 0.3516 |
| Gender |
| Male | 34.16 | 24.97 | 0.7250 |
| Female | 40.26 | 59.13 | 0.3373 |
| Age, years |
| ≤50 | 9.73 | 11.85 | 1.0000 |
| >50 | 42.02 | 45.92 | 0.2963 |
Discussion
Previous studies by Midiri et al (13) and Chen et al (12) reported a different tendency of the
serum CEA levels in CRC patients with advancing stage. Our results
of the present study revealed that the lowest CEA level was
observed in stage C, with significant differences from stages A and
D. The impacts of patient number, age and gender was not taken into
consideration as they could not be controlled in this analysis and
there were no differences between them. The physical condition of
the patients, including the coexistence of other benign diseases
(14), may affect the CEA level to
a certain extent. Additionally, the CC/RC ratio, which was reported
to be 56/44% by Chen et al (12) and 58.4/41.6% by Lin et al
(15), was different from the
49/51% that was observed in the present study, which may lead to a
different tendency if there is internal variation between CC and
RC.
As regards CC, there was significant variation among
stages, with the lowest CEA level in stage C, whereas there was no
such variation in RC. In addition, CC and RC are distinguished by
the CEA level in stages B (P=0.0327), C (P=0.0092) and D
(P=0.0073). We cannot exclude the possibility of a deviation
arising due to insufficient patient number (<30 in several
stages), patient physical condition and statistical error. To
reduce the error arising from the insufficient number of patients,
several patients were added to the follow-up study; however, the
inner differences between CC and RC were not affected.
Several studies focused on the hypothesis that CC
and RC are likely two naturally different diseases; however, the
majority of the currently available studies consider CC and RC as a
single entity. Wakai et al (2) reported that the dietary risk factors
appeared to differ between CC and RC. Li et al (16) reported that the survival of CC
patients was significantly superior to that of RC patients. Nielsen
et al (17) also reported
that a combination of plasma tissue inhibitor of metalloproteinase
1 and CEA may be useful for the early detection of CRC,
particularly CC. Additionally, the Cancer Genome Atlas Network has
reported certain differences between tumors from the right colon
and all other sites (3). This
prompted us to investigate whether the differences in the CEA
levels between CC and RC, despite the overall close association
between CRC and CEA, reflect the fact that CC and RC are of a
different nature, which requires further investigation.
The lowest CEA level was observed in stage C of CC,
with significant differences from stages A and D. Despite the fact
that we added more patients in our subsequent study, we cannot
exclude the possibility that the patient number was insufficient
for analysis, resulting in the unusually low-level of CEA in stage
C, which is inconsistent with the findings of Lee et al
(18), who investigated 233 stage
C patients and reported that stage C patients are more
significantly associated with increased preoperative CEA levels, as
well as the findings of other studies. We also cannot exclude the
possibility that there may be a distinction between stage C and
other stages in several studies stressing the individual effects of
treatment on stage C. Li et al (16) reported that the survival of stage C
patients was significantly superior to that of other CRC patients.
Stage C refers to those patients suffering from cancer cell
metastasis to the lymph nodes. The 5-year overall survival improved
as the number of nodes sampled increased for patients with CC
(19) and the lymph node ratio is
known to be an independent prognostic factor in CC patients with
stage C disease (20). Therefore,
the improved survival rate mentioned above for CC patients with
stage C disease may be correlated with the number of lymph nodes
and should be investigated in the follow-up study. Due to the
limited number of studies on stage C of CC, the unique character of
stage C possibly plays a significant role in the evolution of CC;
however, the underlying mechanisms require further investigation in
the follow-up study.
In the present study, we demonstrated that there is
variation in CEA levels among different stages in patients with CC,
while no such variation was observed among RC patients. Of note,
the CEA level in stage C was the lowest among all stages in CC
patients. Apart from the factors affecting the results, including
age, gender, patient number and physical condition, any unknown
internal distinctions between CC and RC and between stage C and
other CC stages remain to be further investigated. Elucidating
whether there actually is a difference in the nature of CC and RC
may have important implications regarding treatment and prognosis
of these two types of cancer.
Acknowledgements
This study was supported by grants from the Chinese
National Science Foundation projects (no. 81372669), the Chinese
State Key Program in Basic Research (no. 2012CB822103), the Science
and Technology Planning Project of Liao Ning (no. 2012225020) and
the Project of Chinese Ministry of Health (no. W2012RQ23).
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar
|
|
2
|
Wakai K, Hirose K, Matsuo K, Ito H, Kuriki
K, Suzuki T, Kato T, Hirai T, Kanemitsu Y and Tajima K: Dietary
risk factors for colon and rectal cancers: a comparative
case-control study. J Epidemiol. 16:125–135. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cancer Genome Atlas Network. Comprehensive
molecular characterization of human colon and rectal cancer.
Nature. 487:330–337. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mayer RJ, Garnick MB, Steele GD Jr and
Zamcheck N: Carcinoembryonic antigen (CEA) as a monitor of
chemotherapy in disseminated colorectal cancer. Cancer. 42(Suppl
3): 1428–1433. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Petrioli R, Licchetta A, Roviello G, et
al: CEA and CA19.9 as early predictors of progression in
advanced/metastatic colorectal cancer patients receiving
oxaliplatin-based chemotherapy and bevacizumab. Cancer Invest.
30:65–71. 2012. View Article : Google Scholar
|
|
6
|
Gold P and Freedman SO: Specific
carcinoembryonic antigens of the human digestive system. J Exp Med.
122:467–481. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shuster J, Thomson DM, Fuks A and Gold P:
Immunologic approaches to diagnosis of malignancy. Prog Exp Tumor
Res. 25:89–139. 1980.
|
|
8
|
Shively JE and Beatty JD: CEA-related
antigens: molecular biology and clinical significance. Crit Rev
Oncol Hematol. 2:355–399. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hefta LJ, Neumaier M and Shively JE:
Kinetic and affinity constants of epitope specific
anti-carcinoembryonic antigen (CEA) monoclonal antibodies for CEA
and engineered CEA domain constructs. Immunotechnology. 4:49–57.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kojima T, Yoshikawa K, Matsui T, Kodera Y
and Kojima H: Titration of serum CEA, p53 antibodies and CEA-IgM
complexes in patients with colorectal cancer. Mol Med Rep.
2:477–480. 2009.PubMed/NCBI
|
|
11
|
Edge SB and Compton CC: The American Joint
Committee on Cancer: the 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chen CC, Yang SH, Lin JK, Lin TC, Chen WS,
Jiang JK, Wang HS and Chang SC: Is it reasonable to add
preoperative serum level of CEA and CA19-9 to staging for
colorectal cancer? J Surg Res. 124:169–174. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Midiri G, Amanti C, Consorti F, Benedetti
M, Del Buono S, Di Tondo U, Castagna G, Peronace L and Di Paola M:
Usefulness of preoperative CEA levels in the assessment of
colorectal cancer patient stage. J Surg Oncol. 22:257–260. 1983.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pasanen PA, Eskelinen M, Partanen K,
Pikkarainen P, Penttila I and Alhava E: Clinical value of serum
tumour markers CEA, CA 50 and CA 242 in the distinction between
malignant versus benign diseases causing jaundice and cholestasis;
results from a prospective study. Anticancer Res. 12:1687–1693.
1992.
|
|
15
|
Lin JK, Lin CC, Yang SH, Wang HS, Jiang
JK, Lan YT, Lin TC, Li AF, Chen WS and Chang SC: Early
postoperative CEA level is a better prognostic indicator than is
preoperative CEA level in predicting prognosis of patients with
curable colorectal cancer. Int J Colorectal Dis. 26:1135–1141.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Li M, Li JY, Zhao AL and Gu J: Colorectal
cancer or colon and rectal cancer? Clinicopathological comparison
between colonic and rectal carcinomas. Oncology. 73:52–57. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nielsen HJ, Brunner N, Jorgensen LN, et
al: Plasma TIMP-1 and CEA in detection of primary colorectal
cancer: a prospective, population based study of 4509 high-risk
individuals. Scand J Gastroenterol. 46:60–69. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lee WS, Baek JH, Kim KK and Park YH: The
prognostic significant of percentage drop in serum CEA post
curative resection for colon cancer. Surg Oncol. 21:45–51. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hashiguchi Y, Hase K, Ueno H, Mochizuki H,
Kajiwara Y, Ichikura T and Yamamoto J: Prognostic significance of
the number of lymph nodes examined in colon cancer surgery:
clinical application beyond simple measurement. Ann Surg.
251:872–881. 2010. View Article : Google Scholar
|
|
20
|
Elias E, Mukherji D, Faraj W, Khalife M,
Dimassi H, Eloubeidi M, Hattoum H, Abou-Alfa GK, Saleh A and
Shamseddine A: Lymph-node ratio is an independent prognostic factor
in patients with stage III colorectal cancer: a retrospective study
from the Middle East. World J Surg Oncol. 10:632012. View Article : Google Scholar : PubMed/NCBI
|