Introduction
Breast cancer is a heterogeneous disease comprising
different subtypes defined at the clinical, pathological and
molecular levels. In clinical practice, the behavior of the various
different types of breast cancer is variable. The assessment of
hormone receptor and human epidermal growth factor receptor 2
(HER2) status at the time of breast cancer diagnosis is currently
used as a guide to determine the appropriate adjuvant therapy.
Estrogen receptor (ER) and HER2 expression are key factors for
predicting the benefits of using endocrine and HER2-targeted
therapies, respectively. Moreover, the Ki-67 index value is
effective in discriminating between luminal A and B type tumors and
the application of chemotherapy is commonly recommended for
patients with a high Ki-67 value (1). The Ki-67 index value has attracted
significant interest from clinical oncologists. Moreover, treatment
decisions for recurrent cases are generally based on the ER and
HER2 status in the primary tumor, disease-free interval (DFI),
recurrence site and performance status (2).
The important biological markers in early breast
cancer are tumor size, nuclear grade, proliferative activity
(mitotic index and Ki-67 index values), axillary lymph node
involvement, ER, progesterone receptor (PgR) and HER2 status.
Uncontrolled proliferation is a key characteristic of malignant
tumors and, therefore, tumor proliferation is one of the major
factors associated with prognosis (3,4). The
mitotic index (MI) and the Ki-67 index value are the two most
commonly used indices to measure proliferation. MI is defined as
the number of mitoses at the periphery of the tumor (5) and is the main determinant of the
histological grade (Nottingham system) (5). There is currently no standardization
of the Ki-67 measurement and it has not yet been accepted as a
routine biomarker (6). An
international working group reported (7) that substantial variability in the
Ki-67 scoring procedure is observed among some of the world’s most
experienced laboratories and Ki-67 values and cut-offs for clinical
decision-making cannot be transferred between laboratories without
first standardizing the scoring methodology. In our institute, the
Ki-67 index value has been evaluated using immunohistochemistry
(IHC) since 1987 in over 4,000 consecutive cases (8).
The use of the Ki-67 index value as a prognostic and
predictive marker has been extensively investigated in the
neoadjuvant as well as the adjuvant settings (9,10).
Certain studies reported that the Ki-67 index value is a
significant prognostic factor in terms of disease-free and overall
survival after initial treatment (8,11).
However, other studies have questioned the usefulness of the Ki-67
index value as a prognostic factor after recurrence. Delpech et
al (12) reported that high
Ki-67 expression in the primary tumor remained an independent,
adverse prognostic factor in metastatic disease. The Ki-67 index
value in the primary tumor is important for deciding the treatment
for recurrent cases. Therefore, it is important to elucidate the
role and clinical significance of the Ki-67 index value in the
primary tumor in recurrent breast cancer.
In this study, the Ki-67 index value was
investigated in the primary breast cancer tumors and the
association between the Ki-67 index value and the recurrence
profile was also assessed. Moreover, the clinical significance of
the Ki-67 index value in the primary tumor was evaluated as a
prognostic factor in recurrent breast cancer.
Patients and methods
Patients
Immunohistochemical analysis of the Ki-67 index was
performed in 4,701 patients with primary breast cancer from 1987
until March, 2013 at Kumamoto City Hospital. Among these patients,
there were 666 consecutive cases with recurrence after primary
surgery. In terms of the patient characteristics (Table I), the mean age of the patients was
51.6 years (range, 25–95 years) and the mean tumor diameter was 3.1
cm (range, 0.5–17.0 cm). One-third (33.3%) of the patients had
pathologically negative lymph nodes. The ER, PgR and HER2 positive
rates were 59.0, 40.7 and 18.8%, respectively. The median value for
DFI was 30.0 months and the DFI for 290 patients (43.6%) was within
2 years. The predominant sites of recurrence were as follows; soft
tissue, 260 cases (39.1%); bone, 158 cases (23.7%); and viscera,
248 cases (37.2%).
 | Table IPatient characteristics (n=666). |
Table I
Patient characteristics (n=666).
| Variables | Total | % |
|---|
| Primary tumor |
| Menopausal
status |
| Premenopausal | 353 | 53.0 |
| Postmenopausal | 313 | 47.0 |
| Nodal status |
| N0 | 220 | 33.0 |
| N+ | 426 | 64.0 |
| Unknown | 20 | 3.0 |
| Nuclear grade |
| 1 | 119 | 17.9 |
| 2 | 330 | 49.5 |
| 3 | 107 | 16.1 |
| Unknown | 110 | 16.5 |
| ER status |
| (+) | 393 | 59.0 |
| (−) | 273 | 41.0 |
| PgR status |
| (+) | 271 | 40.7 |
| (−) | 338 | 50.8 |
| Unknown | 57 | 8.5 |
| HER2 status |
| (−) | 309 | 46.4 |
| (+) | 125 | 18.8 |
| Unknown | 232 | 34.8 |
| Subtype |
| Luminal | 221 | 33.2 |
| Luminal/HER2 | 55 | 8.3 |
| HER2-enriched | 70 | 10.5 |
|
Triple-negative | 88 | 13.2 |
| Unknown | 232 | 34.8 |
| Recurrence |
| DFI (years) |
| <2 | 290 | 43.6 |
| <5 | 224 | 33.6 |
| ≥5 | 152 | 22.8 |
| Recurrence site |
| Soft tissue | 260 | 39.1 |
| Bone | 158 | 23.7 |
| Viscera | 248 | 37.2 |
| Primary surgery |
| Age (years) |
| Mean ± SD | 51.6±12.9 | |
| Tumor size (mm) |
| Mean ± SD | 30.7±24.1 | |
Histopathological examination
The investigated factors included the presence or
absence of lymph node metastasis, nuclear grade, ER/PgR status,
proliferation (Ki-67 index) and HER2 overexpression in the primary
tumor. The IHC for ER, PgR, Ki-67 and HER2 was performed as
previously described (13). The
positive cell rates for ER/PgR were determined by IHC and a value
of ≥1% was considered as positive. The proliferative activity was
determined by IHC for the Ki-67 antibody (Dako, Glostrup, Denmark).
The fraction of proliferating cells (Ki-67-positive) was based on a
count of at least 500 tumor cells in the peripheral area including
the hot spot and the Ki-67 values were divided into 3 groups as
previously reported (8), namely
<20, ≥20 and ≥50%. HER2 expression was evaluated by
immunostaining (LSAB method) with the HercepTest (Dako). The
staining pattern of HER2 was divided into four groups as follows:
3+, strong and diffuse staining; 2+, moderate and diffuse staining;
1+, focal staining in >10% of the cancer cells; and negative.
All the IHC data, including the Ki-67 index value, were evaluated
by two pathologists who were blinded to the patient data.
ER-positive and HER2-negative tumors were classified as luminal
type; ER-positive and HER2-positive tumors (HER2 IHC: 3+ or 2+ and
FISH amplification ratio >2.0) as luminal/HER2 type; ER-negative
and HER2-positive tumors as HER2-enriched disease; and ER-negative,
PgR-negative and HER2-negative tumors as triple-negative (TN)
type.
Treatment
Postoperative adjuvant therapy is being performed
since 1999, based on the recommendations of the St. Gallen
International Meeting (14). The
chemotherapy regimen for the patients prior to 1999 was oral
fluorouracil agents, a combination of cyclophosphamide +
methotrexate + fluorouracil and anthracycline; from 1999 onwards,
anthracycline and taxanes have been used. Trastuzumab was added as
an adjuvant treatment in 2008; however, it has been used for
patients with recurrence since 2001.
The systemic treatment for recurrent cases was
determined based on ER and HER2 status in the primary tumor, DFI,
recurrence site and performance status (2). In certain cases with recurrent breast
cancer, local treatment, such as resection of the lesion and
radiotherapy, was performed after obtaining informed consent from
the patients.
Statistical analysis
The statistical analysis included the Chi-square
test and Fisher’s exact test to perform inter-group comparisons
(Table II). The Wilcoxon’s
(non-parametric) test was used to compare the mean or median values
for tumor size, age and Ki-67 index value. The prognosis [overall
survival (OS)] was calculated with the Kaplan-Meier method and
tested with the log-rank procedure. The OS after recurrence was
defined as the time from the diagnosis of recurrence to death from
any cause. The Cox’s proportional hazard model was used to perform
univariate and multivariate analyses of the factors associated with
OS after recurrence. A multivariate analysis was performed of only
the cases without missing values. The median follow-up period was
65.9 months in the surviving group. The model was evaluated using
the Harrell C-index (0–1.0) to determine whether the sample size
was appropriate for analysis. A higher index value indicates that
the sample size of the model is appropriate for analysis (15,16).
The sample size for this study had a C-index value of 0.68, which
means that the sample size was adequate.
| Table IIClinicopathological factors and Ki-67
index in recurrent breast cancer. |
Table II
Clinicopathological factors and Ki-67
index in recurrent breast cancer.
| Ki-67 index, no.
(%) | | | Ki-67 index |
|---|
|
| | |
|
|---|
| Variables | <20% | <50% | ≥50% | Total | P-value | Median (%) | P-value |
|---|
| Menopausal
status | | | | | 0.10 | | 0.08 |
| Premenopausal | 102 (28.9) | 157 | 94 | 353 | | 27.0 | |
|
Postmenopausal | 105 (31.1) | 146 | 62 | 313 | | 26.0 | |
| Nodal status | | | | | 0.41 | | 0.42 |
| N0 | 75 (34.1) | 101 | 44 | 220 | | 25.0 | |
| N+ | 131 (30.8) | 191 | 104 | 426 | | 28.0 | |
| Unknown | 1 | 11 | 8 | 20 | | | |
| Nuclear grade | | | | | <0.0001 | | <0.0001 |
| 1 | 57 (47.9) | 50 | 12 | 119 | | 21.0 | |
| 2 | 91 (27.5) | 164 | 75 | 330 | | 29.5 | |
| 3 | 13 (12.1) | 50 | 44 | 107 | | 45.0 | |
| Unknown | 46 | 39 | 25 | 110 | | | |
| ER status | | | | | <0.0001 | | <0.0001 |
| (+) | 160 (40.7) | 180 | 53 | 393 | | 24.0 | |
| (−) | 47 (17.2) | 123 | 103 | 273 | | 40.0 | |
| PgR status | | | | | <0.0001 | | <0.0001 |
| (+) | 114 (41.9) | 128 | 30 | 272 | | 30.0 | |
| (−) | 70 (20.2) | 155 | 113 | 338 | | 43.0 | |
| Unknown | 23 | 20 | 13 | 56 | | | |
| HER2 status | | | | | <0.0001 | | <0.0001 |
| (−) | 96 (31.1) | 139 | 74 | 309 | | 30.0 | |
| (+) | 16 (12.8) | 88 | 21 | 125 | | 35.0 | |
| Unknown | 95 | 76 | 61 | 232 | | | |
| DFI (years) | | | | | <0.0001 | | <0.0001 |
| <2 | 50 (17.2) | 132 | 108 | 290 | | 40.5 | |
| <5 | 81 (36.2) | 106 | 37 | 224 | | 25.0 | |
| ≥5 | 76 (50.0) | 65 | 11 | 152 | | 19.5 | |
| Recurrence
site | | | | | <0.0001 | | <0.0001 |
| Soft tissue | 88 (33.8) | 110 | 62 | 260 | | 26.5 | |
| Bone | 60 (38.0) | 75 | 23 | 158 | | 24.0 | |
| Viscera | 59 (23.8) | 118 | 71 | 248 | | 30.5 | |
| Lung | 39 (29.8) | 63 | 29 | 131 | | 27.0 | <0.0001 |
| Liver | 16 (19.8) | 41 | 24 | 81 | | 38.0 | |
| Brain | 2 (8.0) | 8 | 15 | 25 | | 55.0 | |
Results
Distribution of Ki-67 index values in
primary breast cancer and recurrent cases
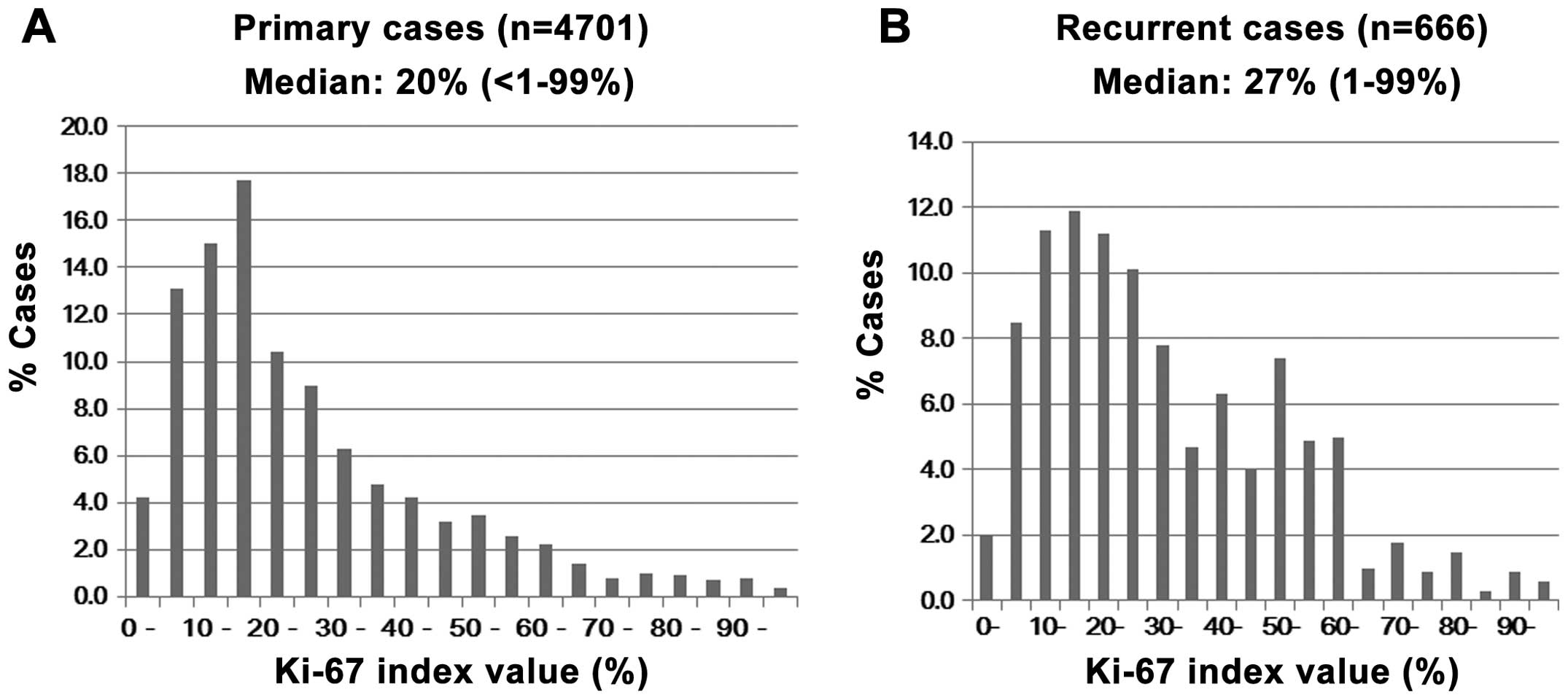
A number of patients had a Ki-67 index value of
10–19% in all the primary cases and the median value was 20%
(Fig. 1A). However, recurrent
cases did not display a clear peak and the number of high-value
cases increased. The median Ki-67 value was 27% in the recurrent
cases (Fig. 1B).
Clinicopathological factors and Ki-67
index in recurrent breast cancer
The Ki-67 index values were investigated in relation
to clinicopathological factors (Table
II). Nuclear grade, ER, PgR, HER2, DFI and recurrence site were
significantly correlated with the Ki-67 index values. Patients with
higher grade, ER-/PgR-negative, HER2-negative, with a shorter DFI
and visceral metastasis had significantly higher Ki-67 values. The
median Ki-67 index value for nuclear grade, ER/PgR, HER2, DFI and
metastatic site exhibited a similar statistical tendency as that
seen in the categorical analysis. The Ki-67 index values for the
recurrent sites were low (24%) in patients with bone metastasis and
higher in patients with liver or brain metastasis (38 and 55%,
respectively). The DFI was inversely correlated with the Ki-67
index values.
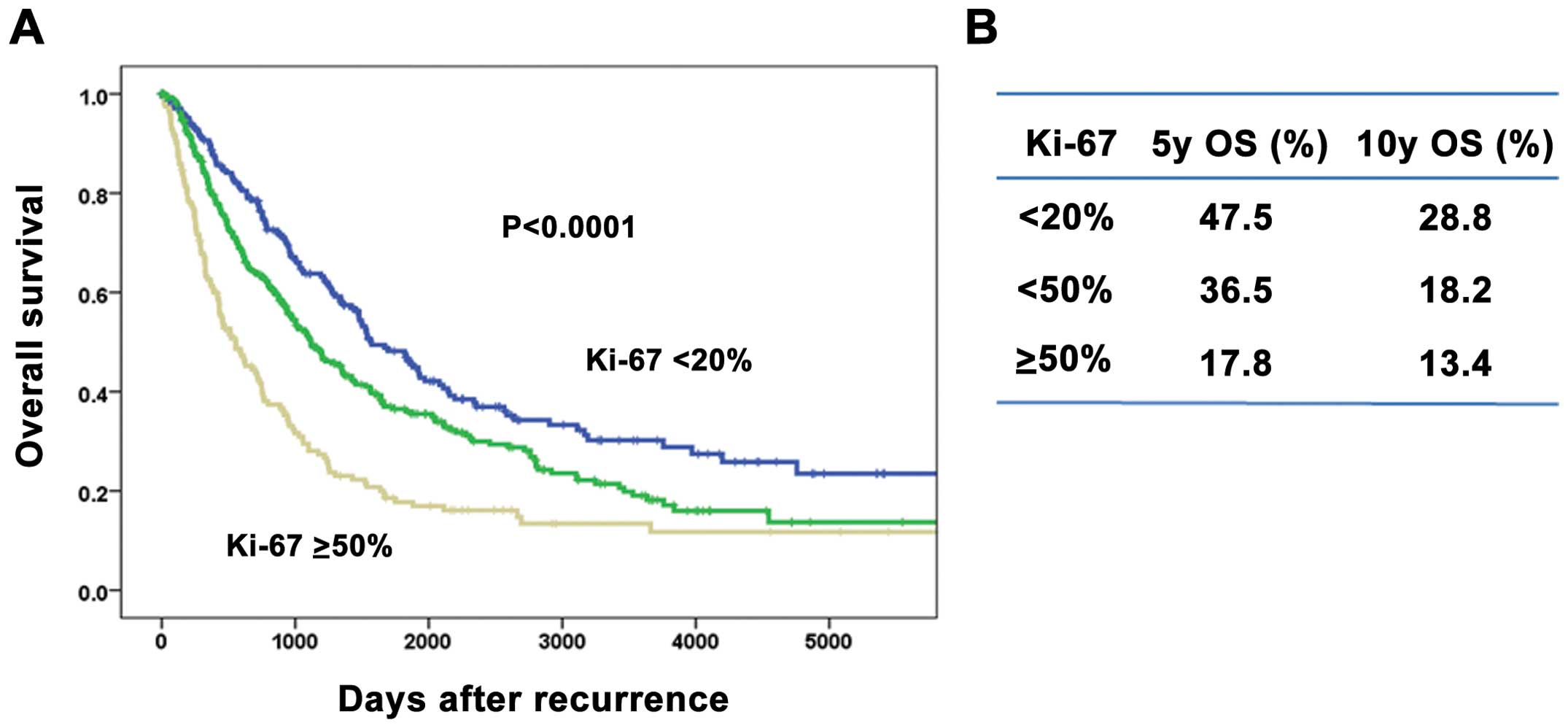
Overall survival after recurrence
according to Ki-67 index values
The association between Ki-67 index values and
prognosis was investigated (Fig.
2). Patients with a higher Ki-67 index value had significantly
lower OS rates after recurrence compared to those with a lower
index value (Fig. 2A). The
5-/10-year OS rates after recurrence were 47.5/28.8%, 36.5/18.2%
and 17.8/13.4% in each of the Ki-67 index groups, respectively
(Fig. 2B).
Uni- and multivariate analysis of factors
for overall survival after recurrence
Univariate and multivariate analyses were performed
to identify the prognostic factors for OS after recurrence
(Table III). The significant
factors included tumor size, lymph node status, hormone dependency,
Ki-67 index values, DFI and recurrence sites in the univariate
analysis. The multivariate analysis revealed that lymph node
status, Ki-67 index values, DFI and recurrence sites were
significant factors for OS. Moreover, a multivariate analysis was
performed in order to determine the prognostic factors according to
each subtype. The analysis revealed that the Ki-67 index value was
an independent factor only in the luminal type. An unexpected
result of this analysis revealed that there were a number of other
factors present in each of the subtypes (Table IV).
| Table IIIUni- and multivariate analysis of
factors for overall survival after recurrence. |
Table III
Uni- and multivariate analysis of
factors for overall survival after recurrence.
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|---|
| Factor | HR (95% CI) | P-value | HR | P-value |
|---|
| Menopausal
status |
| Premenopausal | 1.00 | 0.057 | 1.00 | 0.29 |
|
Postmenopausal | 0.84
(0.69–1.005) | | 0.88 | |
| Tumor size
(cm) |
| <2.0 | 0.64
(0.53–0.78) | <0.0001 | 1.06 | 0.69 |
| ≥2.0 | 1.00 | | 1.00 | |
| Nodal status |
| (−) | 0.53
(0.43–0.65) | <0.0001 | 0.61 | 0.001 |
| (+) | 1.00 | | 1.00 | |
| Nuclear grade |
| 1 | 0.56
(0.40–0.78) | 0.001 | 0.92 | 0.68 |
| 2 | 0.73
(0.56–0.93) | 0.013 | 1.14 | 0.39 |
| 3 | 1.00 | | 1.00 | |
| Ki-67 index |
| <20% | 0.44
(0.34–0.56) | <0.0001 | 0.65 | 0.01 |
| <50% | 0.60
(0.48–0.75) | <0.0001 | 0.70 | 0.009 |
| ≥50% | 1.00 | | 1.00 | |
| ER status |
| (−) | 1.79
(1.49–2.16) | <0.0001 | 1.20 | 0.23 |
| (+) | 1.00 | | 1.00 | |
| PgR status |
| (−) | 1.88
(1.54–2.30) | <0.0001 | 1.26 | 0.12 |
| (+) | 1.00 | | 1.00 | |
| HER2 status |
| (−) | 1.24
(0.95–1.62) | 0.12 | | |
| (+) | 1.00 | | | |
| DFI (years) |
| <2 | 1.00 | | 1.00 | |
| <5 | 1.54
(1.16–2.06) | <0.0001 | 1.27 | 0.21 |
| ≥5 | 2.86
(2.19–3.74) | 0.003 | 2.15 | <0.0001 |
| Recurrence
site |
| Soft tissue | 0.57
(0.46–0.71) | <0.0001 | 0.56 | <0.0001 |
| Bone | 0.77
(0.61–0.97) | 0.028 | 0.94 | 0.67 |
| Viscera | 1.00 | | 1.00 | |
| Table IVMultivariate analysis of factors for
overall survival after disease recurrence according to breast
cancer subtypes. |
Table IV
Multivariate analysis of factors for
overall survival after disease recurrence according to breast
cancer subtypes.
| Factors | Category | Luminal
P-value | Luminal/HER2
P-value | HER2 P-value | Triple-negative
P-value |
|---|
| Menopausal
status |
Pre-/postmenopausal | 0.046 | 0.10 | 0.35 | 0.70 |
| Tumor size
(cm) | <2.0/≥2.0 | 0.52 | 0.17 | 0.007 | 0.21 |
| Nodal status | (−)/(+) | 0.37 | 0.98 | 0.034 | 0.93 |
| Nuclear grade | 1/2/3 | 0.30 | 0.19 | 0.64 | 0.91 |
| Ki-67 value
(%) |
<20/<50/≥50 | 0.037 | 0.69 | 0.36 | 0.73 |
| DFI (years) | <2/<5/≥5 | <0.0001 | 0.36 | 0.11 | 0.067 |
| Recurrence
site | Soft
tissue/bone/viscera | 0.004 | 0.57 | 0.08 | 0.008 |
Discussion
This study included 4,701 cases of primary breast
cancer, with 666 recurrent breast cancer patients at a single
institution and the clinical significance of the Ki-67 index value
as a prognostic marker after recurrence was evaluated. Moreover,
the association between the Ki-67 index value and the
clinicopathological factors that reflect prognosis was
investigated.
There are several limitations that affect the
standardization of the Ki-67 index biomarker. First, there is a
difference in opinion among researchers with regards to which part
of the field to assess. In this study, the hot spot (relatively
dense concentration of cancer nuclei) was the main area evaluated.
An overall average score was recommended by the International Ki67
in Breast Cancer Working Group (17). According to several studies
(18,19), the Ki-67 index value at the hot
spot was significantly correlated with survival. The selection of
hot spots is considered indispensable for the Ki-67 index value
assessment of breast cancer patients in a clinical setting. Second,
there is a wide range of various Ki-67 cut-off points among studies
and researchers. The difficulty in defining a cut-off point does
not mean that the Ki-67 biomarker is not effective for prognosis.
The variability of the Ki-67 cut-off point is dependent on the
clinical end points, the type of therapy, the distribution of cases
and the molecular subtypes. In our institute, we adopted the
cut-off points 20% and 50%, as previous studies revealed that they
were instrumental as reliable points. Moreover, the median value
was 20% in all the primary cases and 50% in the cases with the TN
type (8,20,21).
The Ki-67 index values ranged from 1 to 99%. The
Ki-67 index value for the majority of the primary breast cancer
tumors was 10–19% and the median value was 20%. In the recurrent
cases, there was no peak in the Ki-67 index value and the median
value was 27% in the primary tumor. These findings indicate that
highly proliferative tumors tend to recur. Previous studies
(8,9) reported that the Ki-67 index value in
the primary tumor was a prognostic factor for DFS and OS after
initial treatment. However, the number of studies on the prognostic
significance of the Ki-67 index value in recurrent breast cancer is
currently limited. Delpech et al (12) reported that low Ki-67 expression in
the primary tumor is associated with higher clinical benefit and
longer time-to-progression on first-line endocrine therapy and
longer survival after metastatic recurrence. In this study, we
investigated whether the baseline Ki-67 index value in the primary
tumor is a useful prognostic factor after recurrence.
The findings also demonstrated that a higher Ki-67
index value was significantly correlated with a higher grade of
malignancy for clinicopathological factors such as negative ER/PgR,
higher grade and positive HER2. Moreover, patients with a higher
Ki-67 index value exhibited a significantly shorter DFI and
visceral metastasis, particularly liver and brain metastasis.
Pathmanathan et al (22)
reported a statistically significant difference in breast
cancer-specific survival in the groups using Ki-67 and receptor
status, whereas histological grading was not a significant
predictor of survival in systemically untreated patients with
node-negative breast cancer. The Ki-67 index value provides useful
prognostic information beyond the traditionally assessed
clinicopathological variables. It was reported that the Ki-67 index
value was an independent prognostic factor in early breast cancer,
particularly luminal type tumors (8,23). A
multivariate analysis by Reyal et al (18) revealed that the Ki-67 index value
remained the only significant prognostic factor in the subgroups of
ER-positive and HER2-negative tumors. In addition, a multivariate
analysis by Nishimura et al (20) revealed that the Ki-67 index value
increased significantly from a mean of 29.1% in the primary tumor
to 36.3% at relapse, indicating that the Ki-67 level in the primary
tumor is a significant factor for OS after recurrence. Ibrahim
et al (24) reported that
patients with a Ki-67 index value of <20% exhibited a
significantly higher post-recurrence survival compared to patients
with a Ki-67 index value of ≥20%. Moreover, the bone, lung/pleura
and chest wall were common sites of recurrence in the early
recurrence group with highly proliferative tumors and liver
metastasis was identified in 13.6% of the patients (21). In the late recurrence group
exhibiting low proliferation, recurrence was more common in the
lung/pleura and bone; however, liver and brain metastases were
rarely encountered.
In the present study, the Ki-67 index value in the
primary tumor was an independent significant prognostic factor in
ER-positive and HER2-negative tumors in recurrent breast cancer.
The Ki-67 index value was found to be correlated with DFI and
recurrence site. Furthermore, the values were low (24%) in patients
with bone metastasis, whereas patients with liver or brain
metastasis exhibited higher values (38 and 55%, respectively).
These findings suggest that the Ki-67 index value is correlated
with survival after breast cancer recurrence as well as the
recurrence sites.
In conclusion, we demonstrated that the baseline
Ki-67 index value in the primary tumor was a useful prognostic
factor after breast cancer recurrence. The median Ki-67 index value
at baseline was 20% in all the primary cases and 27% in the
recurrent cases. The Ki-67 index values for the recurrent sites
were low (24%) in patients with bone metastasis and higher in
patients with liver or brain metastasis (38 and 55%, respectively).
The DFI was found to be inversely correlated with the Ki-67 index
values. Moreover, a multivariate analysis for OS after recurrence
revealed that the Ki-67 index value in the primary tumor was an
independent significant factor only in luminal type tumors. The
Ki-67 index value provides important data associated with
recurrence time and recurrence site that are crucial for designing
a suitable treatment plan for patients and for an accurate
prediction of prognosis. Therefore, the Ki-67 index value should be
taken into consideration in the treatment and follow-up of breast
cancer patients.
Acknowledgements
We would like to express our gratitude to the staff
of the Department of Pathology at Kumamoto City Hospital for their
technical assistance and for the collection of cancer tissue
samples.
References
|
1
|
Goldhirsch A, Ingle JN, Gelber RD, Coates
AS, Thürlimann B and Senn HJ; Panel members. Thresholds for
therapies: highlights of the St Gallen International Expert
Consensus on the primary therapy of early breast cancer 2009. Ann
Oncol. 20:1319–1329. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hortobagyi GN: Treatment of breast cancer.
N Engl J Med. 339:974–984. 1998. View Article : Google Scholar
|
|
3
|
Colozza M, Azambuja E, Cardoso F, Sotiriou
C, Larsimont D and Piccart MJ: Proliferative markers as prognostic
and predictive tools in early breast cancer: where are we now? Ann
Oncol. 16:1723–1739. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Stuart-Harris R, Caldas C, Pinder SE and
Pharoah P: Proliferation markers and survival in early breast
cancer: a systematic review and meta-analysis of 85 studies in
32,825 patients. Breast. 17:323–334. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Elston CW and Ellis IO: Pathological
prognostic factors in breast cancer. I. The value of histological
grade in breast cancer: experience from a large study with
long-term follow-up. Histopathology. 19:403–410. 1991. View Article : Google Scholar
|
|
6
|
Harris L, Fritsche H, Mennel R, et al:
American Society of Clinical Oncology 2007 update of
recommendations for the use of tumor markers in breast cancer. J
Clin Oncol. 25:5287–5312. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Polley MY, Leung SC, McShane LM, Gao D,
Hugh JC, Mastropasqua MG, Viale G, Zabaglo LA, Penault-Llorca F,
Bartlett JM, Gown AM, Symmans WF, Piper T, Mehl E, Enos RA, Hayes
DF, Dowsett M and Nielsen TO; International Ki67 in Breast Cancer
Working Group of the Breast International Group and North American
Breast Cancer Group. An international Ki67 reproducibility study. J
Natl Cancer Inst. 105:1897–1906. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Nishimura R, Osako T, Okumura Y, Hayashi
M, Toyozumi Y and Arima N: Ki-67 as a prognostic marker according
to breast cancer subtype and a predictor of recurrence time in
primary breast cancer. Exp Ther Med. 1:747–754. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
de Azambuja E, Cardoso F, de Castro G Jr,
et al: Ki-67 as prognostic marker in early breast cancer: a
meta-analysis of published studies involving 12155 patients. Br J
Cancer. 96:1504–1513. 2007.PubMed/NCBI
|
|
10
|
Jonat W and Arnold N: Is the Ki-67
labelling index ready for clinical use? Ann Oncol. 22:500–502.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yerushalmi R, Woods R, Ravdin PM, Hayes MM
and Gelmon KA: Ki67 in breast cancer: prognostic and predictive
potential. Lancet Oncol. 11:174–183. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Delpech Y, Wu Y, Hess KR, Hsu L, Ayers M,
Natowicz R, Coutant C, Rouzier R, Barranger E, Hortobagyi GN, Mauro
D and Pusztai L: Ki67 expression in the primary tumor predicts for
clinical benefit and time to progression on first-line endocrine
therapy in estrogen receptor-positive metastatic breast cancer.
Breast Cancer Res Treat. 135:619–627. 2012. View Article : Google Scholar
|
|
13
|
Kai K, Nishimura R, Arima N, Miyayama H
and Iwase H: p53 expression status is a significant molecular
marker in predicting the time to endocrine therapy failure in
recurrent breast cancer: a cohort study. Int J Clin Oncol.
11:426–433. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Goldhirsch A, Glick JH, Gelber RD and Senn
HJ: Meeting highlights: International Consensus Panel on the
Treatment of Primary Breast Cancer. J Natl Cancer Inst.
90:1601–1608. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Taktak AF, Eleuteri A, Lake SP and Fisher
AC: A web-based tool for the assessment of discrimination and
calibration properties of prognostic models. Comput Biol Med.
38:785–791. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Harrell FE Jr, Califf RM, Pryor DB, et al:
Evaluating the yield of medical tests. JAMA. 247:2543–2546. 1982.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dowsett M, Nielsen TO, A’Hern R, Bartlett
J, Coombes RC, Cuzick J, Ellis M, Henry NL, Hugh JC, Lively T,
McShane L, Paik S, Penault-Llorca F, Prudkin L, Regan M, Salter J,
Sotiriou C, Smith IE, Viale G, Zujewski JA and Hayes DF;
International Ki-67 in Breast Cancer Working Group. Assessment of
Ki67 in breast cancer: recommendations from the International Ki67
in Breast Cancer Working Group. J Natl Cancer Inst. 103:1656–1664.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Reyal F, Hajage D, Savignoni A, et al:
Long-term prognostic performance of Ki67 rate in early stage,
pT1-pT2, pN0, invasive breast carcinoma. PLoS One. 8:e559012013.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Honma N, Horii R, Iwase T, Saji S, Younes
M, Ito Y and Akiyama F: Ki-67 evaluation at the hottest spot
predicts clinical outcome of patients with hormone
receptor-positive/HER2-negative breast cancer treated with adjuvant
tamoxifen monotherapy. Breast Cancer. Mar 12–2013.(Epub ahead of
print).
|
|
20
|
Nishimura R, Osako T, Okumura Y, Tashima
R, Toyozumi Y and Arima N: Changes in the ER, PgR, HER2, p53 and
Ki-67 biological markers between primary and recurrent breast
cancer: discordance rates and prognosis. World J Surg Oncol.
9:131–137. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Nishimura R, Osako T, Nishiyama Y, Tashima
R, Nakano M, Fujisue M, Toyozumi Y and Arima N: Evaluation of
factors related to late recurrence - later than 10 years after the
initial treatment - in primary breast cancer. Oncology. 85:100–110.
2013.
|
|
22
|
Pathmanathan N, Balleine RL, Jayasinghe
UW, Bilinski KL, Provan PJ, Byth K, Bilous AM, Salisbury EL and
Boyages J: The prognostic value of Ki67 in systemically untreated
patients with node-negative breast cancer. J Clin Pathol.
67:222–228. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ribelles N, Perez-Villa L, Jerez JM,
Pajares B, Vicioso L, Jimenez B, de Luque V, Franco L, Gallego E,
Marquez A, Alvarez M, Sanchez-Muñoz A, Perez-Rivas L and Alba E:
Pattern of recurrence of early breast cancer is different according
to intrinsic subtype and proliferation index. Breast Cancer Res.
15:R982013. View
Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ibrahim T, Farolfi A, Scarpi E, Mercatali
L, Medri L, Ricci M, Nanni O, Serra L and Amadori D: Hormonal
receptor, human epidermal growth factor receptor-2, and Ki67
discordance between primary breast cancer and paired metastases:
clinical impact. Oncology. 84:150–157. 2013. View Article : Google Scholar
|