Introduction
Sirtuin1 (SIRT1), one of the seven members (SIRT1-7)
of the silent information regulator 2 (Sir2) family in mammals, has
activity as a nicotinamide adenine dinucleotide
(NAD+)-dependent histone deacetylase (HDAC) (1–3).
SIRT1 deacetylates several key proteins that regulate the cell
cycle and apoptosis, including Foxo family proteins, Ku70 and p53,
and plays important roles in cell survival (4–7).
SIRT1 was previously reported to be upregulated in
several tumor cell lines and human tumors (8–11).
Upregulation of SIRT1 may induce tumorigenesis and resistance to
certain chemotherapeutic agents (12). When normal cells undergo stress,
such as DNA damage, p53 is activated, which results in the
transcription of the hypermethylated in cancer 1 (HIC1) gene
(13). HIC1 represses
transcription of the gene encoding SIRT1, inducing pathways
leading to cell senescence or apoptosis. However, during the early
stage of tumor progression, epigenetic silencing of HIC1
leads to upregulation of SIRT1. Upregulated SIRT1
inactivates p53 by deacetylation, impairing the functions of p53
and leading to a defective apoptotic response to DNA damage. This
allows cells to reproduce in the presence of damaged DNA, resulting
in the accumulation of mutations, including p53. Upregulated mutant
p53 interferes with the functions of wild-type p53, disrupting
cell-cycle control and promoting tumor progression (14, 15).
Locally advanced uterine cervical cancer is
extremely difficult to treat. The standard treatment for patients
with International Federation of Gynecology and Obstetrics (FIGO)
stage IIIA, IIIB, and IVA uterine cervical cancer consists of
concurrent chemoradiotherapy (CCRT) (16, 17), but patient prognosis is poor
(18, 19). Successful neoadjuvant chemotherapy
(NAC), followed by hysterectomy, has been reported to be effective
in patients with locally advanced, uterine cervical cancer
(20), with a prognosis equal to
that of CCRT. However, the prognosis is worse if NAC is
unsuccessful, as hysterectomy cannot be performed, and
consequently, the treatment strategy must be changed from surgery
to radiation therapy, resulting in a crucial delay (21, 22). Thus, it is important to identify
prognostic factors in patients with locally advanced cervical
cancer that predict whether NAC is likely to be successful
(23–27).
Thus far, the expression of SIRT1 has not been
assessed in patients with locally advanced uterine cervical cancer.
Therefore, the present study was designed to examine the
correlation between SIRT1 expression and the efficacy of NAC for
locally advanced, uterine cervical cancer.
Patients and methods
Patients and samples
The retrospective study included 62 patients aged
<70 years with locally advanced uterine cervical cancer (FIGO
stages IIIA and IIIB), initially treated at the Osaka City
University Medical School Hospital (Osaka, Japan) between 1995 and
2010. Tumor samples were obtained by biopsy prior to NAC. The
patients were divided into two groups: One in which NAC was
effective, surgery was possible and radiation therapy was performed
(NAC+OP+R group; n=35), and the second in which NAC was ineffective
and, therefore, radiation therapy alone was performed (NAC+R group;
n=27). Additionally, patients were further divided into groups that
attained complete/partial remission (CR+PR) and stable/progressive
disease (SD+PD) in response to NAC. Written informed consent was
obtained from all the patients prior to immunohistochemical
examination. The study was approved by the Ethics Committee of
Osaka City University (IRB no. 2581).
Balloon-occluded arterial infusion
chemotherapy (BOAI) for NAC
Pelvic angiography was performed under local
anesthesia using Seldinger's technique (28) to localize the tumor and feeder
vessels. A balloon-wedge single-pressure catheter (5F, 80 cm in
length; Dispomedica GmbH, Hamburg, Germany) was inserted into each
femoral artery and subsequently into the internal iliac artery. The
balloon catheters were advanced until they reached the vicinity of
the feeder vessel (usually the uterine artery), where the balloon
was inflated to interrupt local blood flow.
cis-Diamminedichloroplatinum (CDDP) was slowly infused
intra-arterially through the two catheters over a period of 30 min
(28). The two ovarian arteries
were blocked following the first round of BOAI to increase the
intratumor concentration of CDDP. BOAI was performed three times in
each patient to shrink the tumor. Adequate hydration was ensured
prior to and following CDDP administration, and anti-emetics and
diuretics were administered as appropriate. CDDP was administered
at doses of 50, 75, or 100 mg/m2, depending on patient
age and renal function. The efficacy of CDDP arterial infusion
therapy was evaluated by cytology, histology, serum tumor marker
level and magnetic resonance imaging (MRI) prior to the initiation
of CDDP treatment. The results were compared with those obtained
following the completion of each arterial infusion. MRI was used to
estimate tumor regression by measuring its size in two dimensions
(29, 30). Tumor tissue was obtained from all
the patients who had undergone punch biopsy or surgery.
Immunohistochemical analysis
The expression of SIRT1 and p53 was examined in
paraffin-embedded sections using antibodies to SIRT1 and p53,
respectively, and the avidin-biotin peroxidase complex method.
Briefly, 4-µm paraffin sections were deparaffinized and immersed in
3% hydrogen peroxidase in methanol to block endogenous peroxidase
activity. The antigen was retrieved by immersing the slides in 10
mM citrate buffer (pH 6.0) and heating in an autoclave at 110°C for
20 min, followed by washing in phosphate-buffered solutions (PBS).
The manufacturers' instructions were followed for the Dako LSAB 2
peroxidase kit (Dako, Kyoto, Japan). The sections were incubated
with a 1:100 dilution of polyclonal rabbit anti-human SIRT1 (Santa
Cruz Biotechnology, Inc., Santa Cruz, CA, USA) or a 1:100 dilution
of monoclonal mouse anti-human p53 (Santa Cruz Biotechnology, Inc.)
overnight at 4°C. The sections were washed with PBS for 15 min and
incubated for 10 min with biotinylated goat anti-mouse or
anti-rabbit immunoglobulin G (Dako). The sections were incubated
with the streptavidin-peroxidase complex, with
3,3′;-diaminobenzidine used as the chromogen. Finally, the sections
were counterstained with Mayer's hematoxylin. The specificity of
the immunohistochemical reactions was checked by omitting the
primary antibody. SIRT1 and p53 expression was quantitatively
analyzed as described (31). The
mean percentage of positive tumor cells was determined in five
separate areas (magnification, x400), with positivity rates of
<5, 5–25, 25–50, 50–75 and >75% scored as 0–4, respectively.
The staining intensity was scored as weak (1+), moderate (2+), or
intense (3+). For each specimen, the percentage of positive tumor
cells was multiplied by the staining intensity to yield a weighted
score.
Statistical analysis
Data are presented as mean ± standard deviation. The
Kaplan-Meier and log-rank tests were performed for prognostic
analysis. Weighted scores were compared using the Mann-Whitney U
test. Student's t-test and the χ2 test were performed as
appropriate for between-group comparisons. SPSS software, version
21.0 (IBM, Armonk, NY, USA), was used for all the statistical
analyses. P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient characteristics
In total, 35 of the 62 patients with locally
advanced, uterine cervical cancer were assigned to the NAC+OP+R
group and 27 to the NAC+R group. The mean ages were 49.3 (range,
24–69 years) and 52.3 years (range, 36–68 years), respectively. Of
the 35 patients in the NAC+OP+R group, one was classified as stage
IIIA and 34 as stage IIIB, whereas all the 27 patients in the NAC+R
group were classified as stage IIIB. Histologically, 30 patients in
the NAC+OP+R group were classified as having squamous cell
carcinoma and five as having adenocarcinoma. A total of 22 patients
in the NAC+R group were classified as having squamous cell
carcinoma, three as having adenocarcinoma, and one each as having
adenosquamous carcinoma and glassy cell carcinoma. There were no
significant differences between the two groups (Table I).
 | Table ICharacteristics of patients in the
NAC+OP+R and NAC+R groups. |
Table I
Characteristics of patients in the
NAC+OP+R and NAC+R groups.
| NAC+OP+R | NAC+R | P-value |
|---|
| Patients, n | 35 | 27 | |
| Age, years |
| Mean ±
SD | 49.3±12.7 | 52.3±11.1 | 0.322a |
|
Range | 24–69 | 36–68 | |
| FIGO stage, n |
| IIIA | 1 | 0 | 0.376b |
| IIIB | 34 | 27 | |
| Histology, n |
| SCC | 30 | 22 | 0.433b |
| A | 5 | 3 | |
| AS | 0 | 1 | |
|
Others | 0 | 1 | |
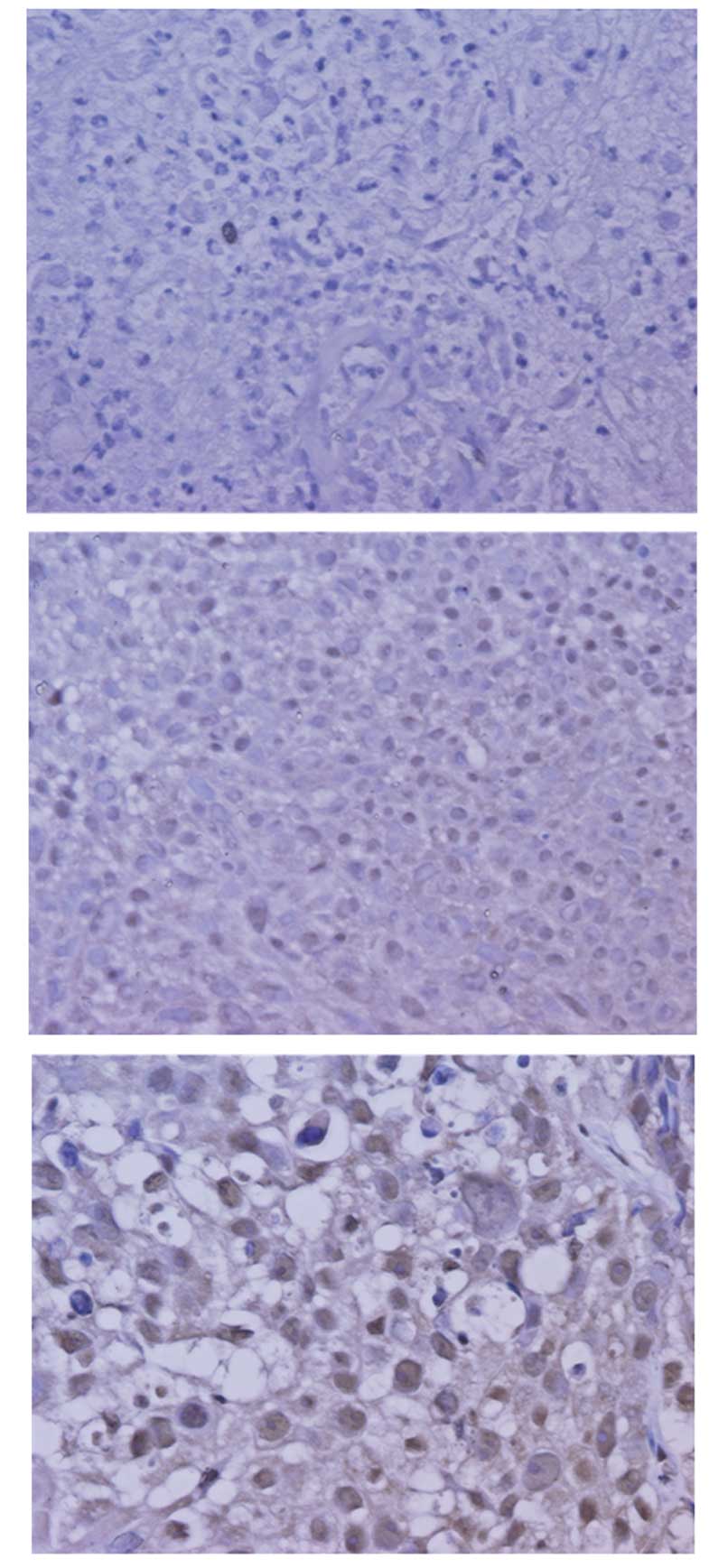
Expression of SIRT1
SIRT1 was expressed in the nuclei of the tumor cells
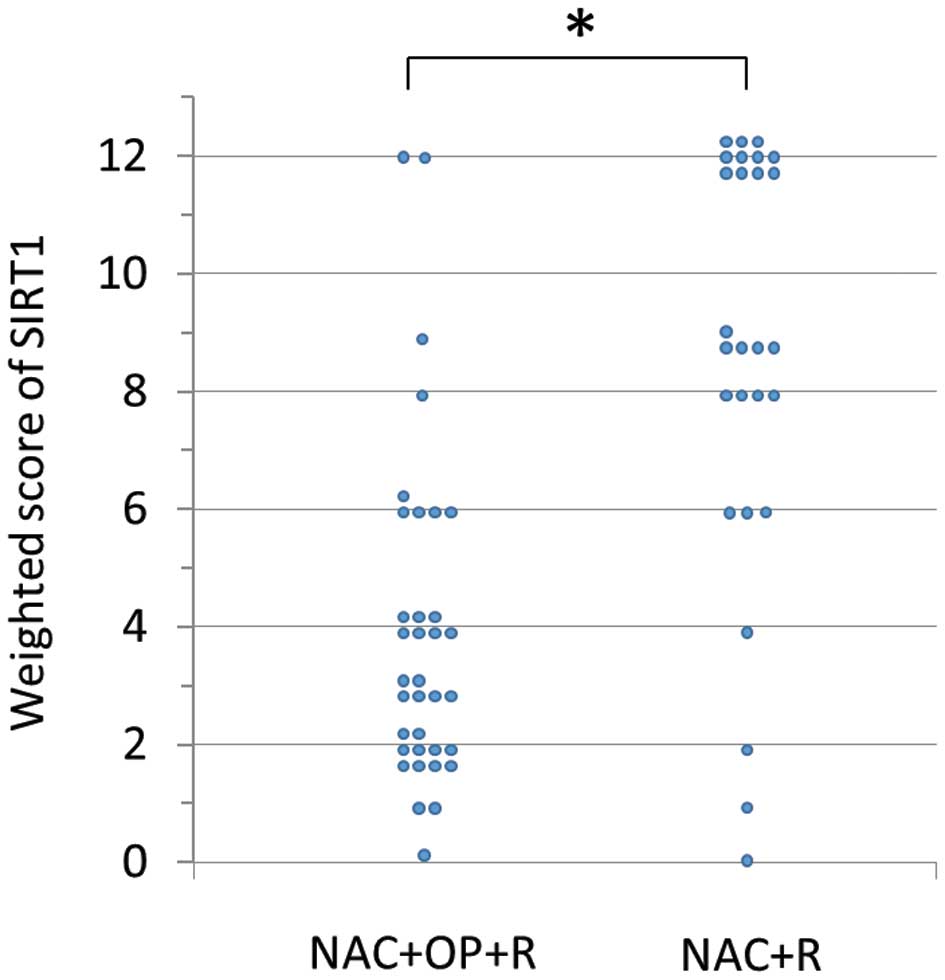
(Fig. 1). The weighted scores in
the two groups are shown in Table
II. The mean weighted score for SIRT1 expression was
significantly lower in the NAC+OP+R compared to the NAC+R group
(3.97 vs. 8.67, P<0.001; Fig.
2). In total, 30 of the 62 patients had weighted scores of 0–4
(low expression) and 32 had weighted scores of 6–12 (high
expression). There were no significant differences between these
two groups (Table III).
| Table IIWeighted scores of SIRT1 expression in
the NAC+OP+R and NAC+R groups. |
Table II
Weighted scores of SIRT1 expression in
the NAC+OP+R and NAC+R groups.
| Patients, n |
|---|
|
|
|---|
| Weighted score | NAC+OP+R | NAC+R |
|---|
| 0 | 1 | 1 |
| 1 | 2 | 1 |
| 2 | 10 | 1 |
| 3 | 6 | 0 |
| 4 | 7 | 1 |
| 6 | 5 | 3 |
| 8 | 1 | 4 |
| 9 | 1 | 5 |
| 12 | 2 | 11 |
| Total | 35 | 27 |
| Weighted score,
mean | 3.97 | 8.67 |
| Table IIICharacteristics of the patients in
the low and high SIRT1 expression groups. |
Table III
Characteristics of the patients in
the low and high SIRT1 expression groups.
|
Characteristics | ≤4a | ≥6a | P-value |
|---|
| Patients, n | 30 | 32 | |
| Age, years |
| Mean ±
SD | 49.8±12.4 | 51.3±11.8 | 0.633b |
|
Range | 24–69 | 24–68 | |
| FIGO stage, n |
|
IIIA | 0 | 1 | 0.329c |
|
IIIB | 30 | 31 | |
| Histology, n |
|
SCC | 26 | 26 | 0.585c |
| A | 4 | 4 | |
| AS | 0 | 1 | |
|
Others | 0 | 1 | |
Expression of p53
p53 was expressed in the nuclei of the tumor cells.
The weighted scores are shown in Table IV. The mean weighted score for p53
expression was also significantly lower in the NAC+OP+R group
compared to the NAC+R group (4.23 vs. 6.70; P<0.001).
| Table IVWeighted scores of p53 expression in
the NAC+OP+R and NAC+R groups. |
Table IV
Weighted scores of p53 expression in
the NAC+OP+R and NAC+R groups.
| Patients, n |
|---|
|
|
|---|
| Weighted score | NAC+OP+R | NAC+R |
|---|
| 0 | 0 | 1 |
| 1 | 2 | 0 |
| 2 | 10 | 0 |
| 3 | 1 | 3 |
| 4 | 12 | 4 |
| 6 | 5 | 7 |
| 8 | 3 | 6 |
| 9 | 1 | 2 |
| 12 | 1 | 4 |
| Total | 35 | 27 |
| Weighted score,
mean | 4.23 | 6.70 |
Correlation between expression of
SIRT1 and p53
In total, 19 of the 62 patients showed low
expression of SIRT1 and p53, and 18 showed high expression. There
was a weak correlation between expression of SIRT1 and p53
(|r|=0.247).
Correlation between expression of
SIRT1 and effects of NAC
Of the 35 patients in the NAC+OP+R group, 26 (74%)
showed low SIRT1 expression, whereas nine (26%) showed high SIRT1
expression. The group with low SIRT1 expression was significantly
more sensitive to NAC (P=0.001; Table
V).
| Table VNumbers of patients with low and high
SIRT1 expression in the NAC+OP+R and NAC+R groups. |
Table V
Numbers of patients with low and high
SIRT1 expression in the NAC+OP+R and NAC+R groups.
| Expression | NAC+OP+R, n
(%) | NAC+R, n (%) | P-value |
|---|
| Low, ≤4 | 26 (87) | 4 (13) |
<0.001a |
| High, ≥6 | 9 (28) | 23 (72) | |
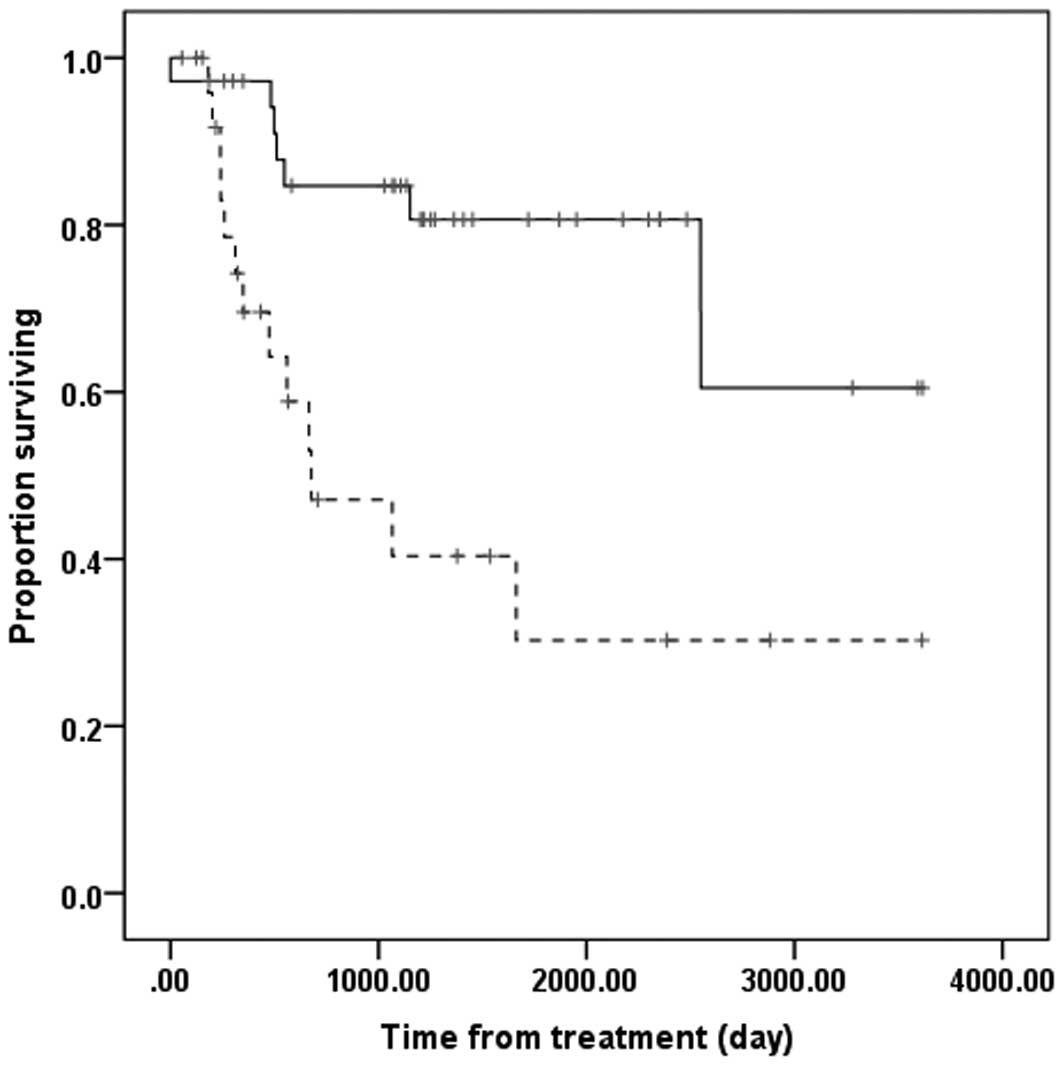
Survival
The overall survival time was significantly longer
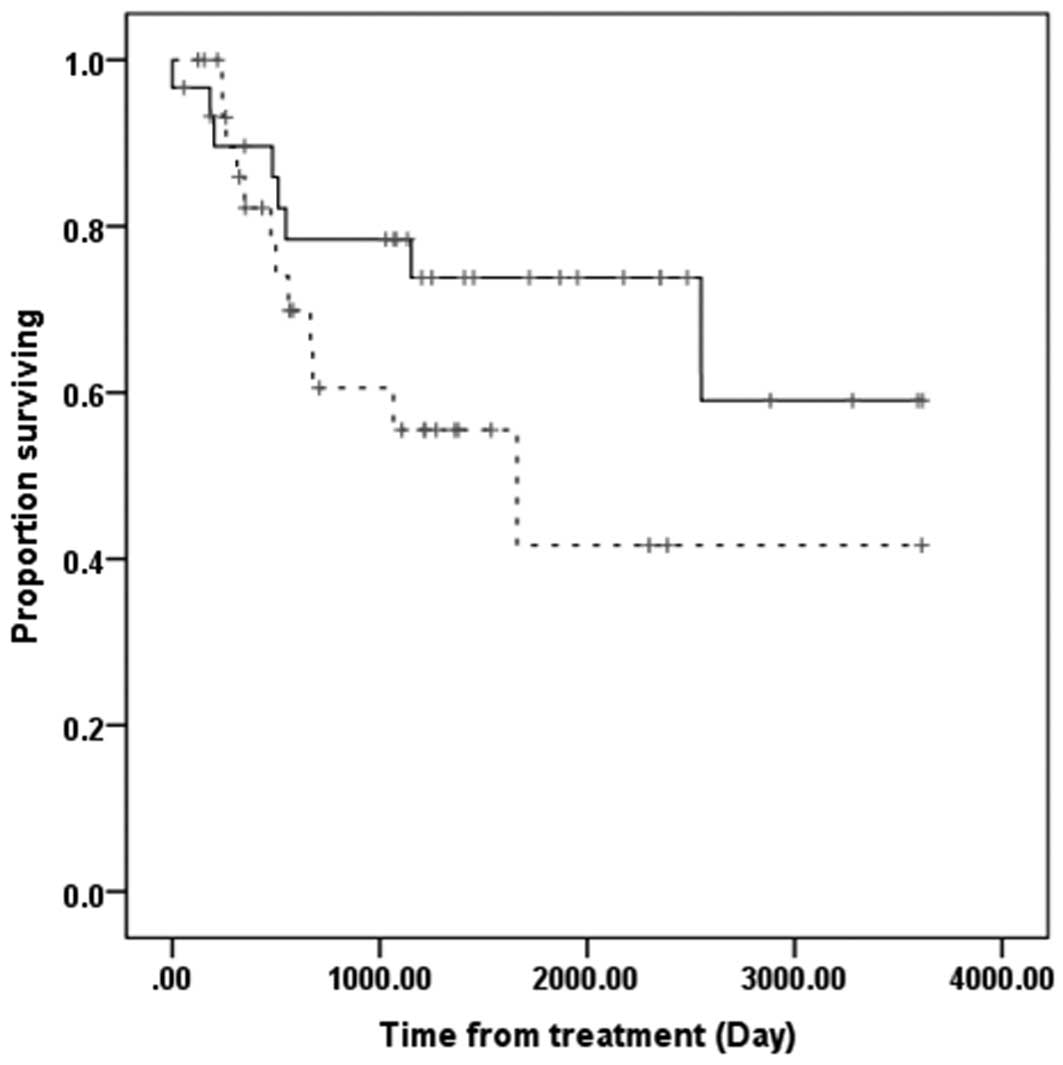
in the NAC+OP+R compared to the NAC+R group (Fig. 3). However, overall survival was
similar in patients with low and high SIRT1 expression (Fig. 4).
Discussion
The results of the present study show the
association between the expression of SIRT1 and the efficacy of
NAC. NAC was ineffective in the majority of patients with high
SIRT1 expression, who were unable to undergo surgery. Overall
survival time was significantly longer in the NAC+OP+R compared to
the NAC+R group. These results are in agreement with findings
showing that prognosis is worse when NAC is unsuccessful (21, 22). By contrast, overall survival time
did not differ significantly in the groups of patients with high
and low SIRT1 expression.
In general, CCRT is considered the standard
treatment for patients with locally advanced, uterine cervical
cancer. However, limited clinical studies have assessed CCRT in
Japanese patients with locally advanced, uterine cervical cancer.
Although surgery following NAC has been reported effective
(20), NAC is not currently
recommended, as if NAC is not effective, surgery is difficult to
perform and radiation therapy is required. Radiation therapy
following chemotherapy has shown poorer prognosis compared to
radiation alone (21, 22). Thus, identifying factors prognostic
of the efficacy of NAC is important in patients with locally
advanced uterine cervical cancer.
SIRT1 is a member of the silent information
regulator 2 (Sir2) family in mammals, with activity as an
NAD+-dependent HDAC (1–3).
SIRT1 deacetylates several key cell-cycle and apoptosis regulating
proteins (4–7). SIRT1 expression has been reported to
increase in various human malignant tumors. SIRT1 is considered a
tumor promoter, as it inhibits tumor suppressor genes such as p53
(14, 15). SIRT1 overexpression has been
associated with primary tumorigenesis, metastasis, chemoresistance
and patient prognosis. However, other studies have reported that
SIRT1 may act as a tumor suppressor (32, 33).
The present study is the first to report a
correlation between SIRT1 expression and locally advanced, uterine
cervical cancer. These findings indicate that NAC may be more
effective in patients with low compared to high SIRT1 expression,
suggesting that SIRT1 expression may predict the efficacy of NAC in
patients with locally advanced, uterine cervical cancer. As
overexpression of SIRT1 has been associated with chemoresistance,
lower SIRT1 expression may result in tumor susceptibility to
treatment. When the correlation between p53 expression and NAC was
assessed in patients with locally advanced, uterine cervical
cancer, the observed results were similar to those for SIRT1 and
NAC (P=0.001; data not shown). A weak correlation was also observed
between SIRT1 and p53 expression. Human papillomavirus (HPV)
infection causes the majority of uterine cervical cancers, with the
viral E6 and E7 proteins playing important roles in tumor
progression (34). The E6 protein
targets p53, inducing a loss of p53 tumor suppressor activity, such
as apoptosis (35, 36). By contrast, HPV E7 protein has been
reported to activate SIRT1 expression, leading to a defective
apoptotic response (37). Thus,
HPV infection enhances SIRT1 and p53 expression, providing further
evidence for the significant role of SIRT1 in cervical cancer.
If NAC is not successful in patients with locally
advanced, uterine cervical cancer, their prognosis becomes worse.
Therefore, it is important to identify factors prognostic of the
success of NAC in these patients. SIRT1 expression may predict the
efficacy of NAC as a treatment for locally advanced, uterine
cervical cancer. Our previous study reported that the expression of
bax, bcl-xL, and MAD2 (mitotic arrest deficiency 2) proteins may
predict the efficacy of NAC in patients with locally advanced,
uterine cervical cancer (25,
38). Taken together, a
combination of these factors may more effectively predict the
efficacy of NAC in these patients.
References
|
1
|
Blander G and Guarente L: The Sir2 family
of protein deacetylases. Annu Rev Biochem. 73:417–435. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Imai S, Armstrong CM, Kaeberlein M and
Guarente L: Transcriptional silencing and longevity protein Sir2 is
an NAD-dependent histone deacetylase. Nature. 403:795–800. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Voelter-Mahlknecht S and Mahlknecht U:
Cloning, chromosomal characterization and mapping of the
NAD-dependent histone deacetylases gene sirtuin 1. Int J Mol Med.
17:59–67. 2006.PubMed/NCBI
|
|
4
|
Brunet A, Sweeney LB, Sturgill JF, Chua
KF, Greer PL, Lin Y, Tran H, Ross SE, Mostoslavsky R, Cohen HY, Hu
LS, Cheng HL, Jedrychowski MP, Gygi SP, Sinclair DA, Alt FW and
Greenberg ME: Stress-dependent regulation of FOXO transcription
factors by the SIRT1 deacetylase. Science. 303:2011–2015. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cohen HY, Lavu S, Bitterman KJ, Hekking B,
Imahiyerobo TA, Miller C, Frye R, Ploegh H, Kessler BM and Sinclair
DA: Acetylation of the C terminus of Ku70 by CBP and PCAF controls
Bax-mediated apoptosis. Mol Cell. 13:627–638. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Luo J, Nikolaev AY, Imai S, Chen D, Su F,
Shiloh A, Guarente L and Gu W: Negative control of p53 by Sir2alpha
promotes cell survival under stress. Cell. 107:137–148. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Vaziri H, Dessain SK, Ng Eaton E, Imai SI,
Frye RA, Pandita TK, Guarente L and Weinberg RA: hSIR2(SIRT1)
functions as an NAD-dependent p53 deacetylase. Cell. 107:149–159.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hida Y, Kubo Y, Murao K and Arase S:
Strong expression of a longevity-related protein, SIRT1, in Bowen's
disease. Arch Dermatol Res. 299:103–106. 2007.PubMed/NCBI
|
|
9
|
Huffman DM, Grizzle WE, Bamman MM, Kim JS,
Eltoum IA, Elgavish A and Nagy TR: SIRT1 is significantly elevated
in mouse and human prostate cancer. Cancer Res. 67:6612–6618. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kuzmichev A, Margueron R, Vaquero A,
Preissner TS, Scher M, Kirmizis A, Ouyang X, Brockdorff N,
Abate-Shen C, Farnham P and Reinberg D: Composition and histone
substrates of polycomb repressive group complexes change during
cellular differentiation. Proc Natl Acad Sci USA. 102:1859–1864.
2005. View Article : Google Scholar
|
|
11
|
Jang KY, Kim KS, Hwang SH, Kwon KS, Kim
KR, Park HS, Park BH, Chung MJ, Kang MJ, Lee DG and Moon WS:
Expression and prognostic significance prognostic of SIRT1 in
ovarian epithelial tumours. Pathology. 41:366–371. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chen HC, Jeng YM, Yuan RH, Hsu HC and Chen
YL: SIRT1 promotes tumorigenesis and resistance to chemotherapy in
hepatocellular carcinoma and its expression predicts poor
prognosis. Ann Surg Oncol. 19:2011–2019. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chen WY, Wang DH, Yen RC, Luo J, Gu W and
Baylin SB: Tumor suppressor HIC1 directly regulates SIRT1 to
modulate p53-dependent DNA-damage responses. Cell. 123:437–448.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Baylin SB and Ohm JE: Epigenetic gene
silencing in cancer - a mechanism for early oncogenic pathway
addiction? Nat Rev Cancer. 6:107–116. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lim CS: Human SIRT1: a potential biomarker
for tumorigenesis? Cell Biol Int. 31:636–637. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Japan Society of Gynecologic Oncology
(eds), . Formulation Committee of the Treatment Guidelines for
Cervical Cancer. Kanehara & Co.; Tokyo: 2011, (In
Japanese).
|
|
17
|
National Comprehensive Cancer Network, .
NCCN Clinical Practice Guidelines in Oncology - Cervical Cancer -
Version II. 2013
|
|
18
|
Morris M, Eifel PJ, Lu J, Grigsby PW,
Levenback C, Stevens RE, Rotman M, Gershenson DM and Mutch DG:
Pelvic radiation with concurrent chemotherapy compared with pelvic
and para-aortic radiation for high-risk cervical cancer. N Engl J
Med. 340:1137–1143. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Eifel PJ, Winter K, Morris M, Levenback C,
Grigsby PW, Cooper J, Rotman M, Gershenson D and Mutch DG: Pelvic
irradiation with concurrent chemotherapy versus pelvic and
para-aortic irradiation for high-risk cervical cancer: an update of
radiation therapy oncology group trial (RTOG) 90–01. J Clin Oncol.
22:872–880. 2004.PubMed/NCBI
|
|
20
|
Ishiko O, Sumi T, Yasui T, Matsumoto Y,
Kawamura N, Ogita S, Kamino T, Nakamura K and Yamada R:
Balloon-occluded arterial infusion chemotherapy, simple total
hysterectomy, and radiotherapy as a useful combination-therapy for
advanced cancer of the uterine cervix. Oncol Rep. 7:141–144.
2000.
|
|
21
|
Souhami L, Gil RA, Allan SE, Canary PC,
Araújo CM, Pinto LH and Silveira TR: A randomized trial of
chemotherapy followed by pelvic radiation therapy in stage IIIB
carcinoma of the cervix. J Clin Oncol. 9:970–977. 1991.PubMed/NCBI
|
|
22
|
Tattersall MH, Lorvidhaya V, Vootiprux V,
Cheirsilpa A, Wong F, Azhar T, Lee HP, Kang SB, Manalo A and Yen
MS: Randomized trial of epirubicin and cisplatin chemotherapy
followed by pelvic radiation in locally advanced cervical cancer.
Cervical Cancer Study Group of the Asian Oceanian Clinical Oncology
Association. J Clin Oncol. 13:444–451. 1995.
|
|
23
|
Ishiko O, Sumi T, Yasui T, Matsumoto Y,
Ogita S, Kaminou T, Nakamura K and Yamada R: Tumor marker and MR
imaging criteria for evaluating the efficacy of cyclic
balloon-occluded arterial infusion for advanced cancer of the
uterine cervix. Oncol Rep. 7:827–830. 2000.PubMed/NCBI
|
|
24
|
Ishiko O, Sumi T, Yoshida H, Ogita S and
Yamada R: Expression of apoptosis regulatory proteins in advanced
cancer of the uterine cervix after cyclic balloon-occluded arterial
infusion chemotherapy. Int J Oncol. 18:1151–1155. 2001.
|
|
25
|
Okamoto E, Sumi T, Misugi F, Nobeyama H,
Hattori K, Yoshida H, Matsumoto Y, Yasui T, Honda K and Ishiko O:
Expression of apoptosis-related proteins in advanced uterine
cervical cancer after balloon-occluded arterial infusion
chemotherapy as an indicator of the efficiency of this therapy. Int
J Mol Med. 15:41–47. 2005.
|
|
26
|
Nobeyama H, Sumi T, Misugi F, Okamoto E,
Hattori K, Matsumoto Y, Yasui T, Honda K, Iwai K and Ishiko O:
Association of HPV infection with prognosis after neoadjuvant
chemotherapy in advanced uterine cervical cancer. Int J Mol Med.
14:101–105. 2004.PubMed/NCBI
|
|
27
|
Benedetti Panici P, Bellati F, Manci N,
Pernice M, Plotti F, Di Donato V, Calcagno M, Zullo MA, Muzii L and
Angioli R: Neoadjuvant chemotherapy followed by radical surgery in
patients affected by FIGO stage IVA cervical cancer. Ann Surg
Oncol. 14:2643–2648. 2007.
|
|
28
|
Tsuji K, Yamada R, Kawabata M, Mitsuzane
K, Sato M, Iwahashi M, Kitayama S and Nakano R: Effect of balloon
occluded arterial infusion of anticancer drugs on the prognosis of
cervical cancer treated with radiation therapy. Int J Radiat Oncol
Biol Phys. 32:1337–1345. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sironi S, Belloni C, Taccagni G and
DelMaschio A: Invasive cervical carcinoma: MR imaging after
preoperative chemotherapy. Radiology. 180:719–722. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kim KH, Lee BH, Do YS, Chin SY, Park SY,
Kim BG and Jang JJ: Stage IIb cervical carcinoma: MR evaluation of
effect of intraarterial chemotherapy. Radiology. 192:61–65. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Sinicrope FA, Ruan SB, Cleary KR, Stephens
LC, Lee JJ and Levin B: bcl-2 and p53 oncoprotein expression during
colorectal tumorigenesis. Cancer Res. 55:237–241. 1995.PubMed/NCBI
|
|
32
|
Firestein R, Blander G, Michan S,
Oberdoerffer P, Ogino S, Campbell J, Bhimavarapu A, Luikenhuis S,
de Cabo R, Fuchs C, Hahn WC, Guarente LP and Sinclair DA: The SIRT1
deacetylase suppresses intestinal tumorigenesis and colon cancer
growth. PLoS One. 3:e20202008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wang RH, Zheng Y, Kim HS, Xu X, Cao L,
Luhasen T, Lee MH, Xiao C, Vassilopoulos A, Chen W, Gardner K, Man
YG, Hung MC, Finkel T and Deng CX: Interplay among BRCA1, SIRT1,
and Survivin during BRCA1-associated tumorigenesis. Mol Cell.
32:11–20. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
zur Hausen H: Papillomaviruses causing
cancer: evasion from host-cell control in early events in
carcinogenesis. J Natl Cancer Inst. 92:690–698. 2000.PubMed/NCBI
|
|
35
|
Werness BA, Levine AJ and Howley PM:
Association of human papillomavirus types 16 and 18 E6 proteins
with p53. Science. 248:76–79. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Bremer GL, Tieboschb AT, van der Putten
HW, de Haan J and Arends JW: p53 tumor suppressor gene protein
expression in cervical cancer: relationship to prognosis. Eur J
Obstet Gynecol Reprod Biol. 63:55–59. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Allison SJ, Jiang M and Milner J:
Oncogenic viral protein HPV E7 up-regulates the SIRT1 longevity
protein in human cervical cancer cells. Aging (Albany NY).
1:316–327. 2009.PubMed/NCBI
|
|
38
|
Morishita M, Sumi T, Nakano Y, Teramae M,
Fukuda T, Nobeyama H, Yoshida H, Matsumoto Y, Yasui T and Ishiko O:
Expression of mitotic-arrest deficiency 2 predicts the efficacy of
neoadjuvant chemotherapy for locally advanced uterine cervical
cancer. Exp Ther Med. 3:341–346. 2011.
|