Introduction
Phyllodes tumors have a low incidence (1 in 100,000
women) and account for only 0.5% of all breast neoplasms (1). The majority of these tumors arise in
women aged 35–55 years (approximately 20 years later compared to
fibroadenomas) (2). In men, phyllodes
tumors are very rare, with only few cases described to date
(3,4).
The World Health Organisation classifies phyllodes tumors into
benign, borderline and malignant, according to The
histopathological characteristics. Borderline and malignant
phyllodes tumors are distinguished from benign phyllodes tumors by
the presence of ‘Moderate or marked stromal cellularity and atypia,
stromal overgrowth, brisk mitotic activity (≥5/10 high-power
fields) and permeative margins’ (5).
Clinically, borderline and malignant phyllodes tumors are
characterized by their propensity for local and distant recurrence.
The primary treatment for borderline and malignant phyllodes tumors
is wide local excision (margins ≥1 cm), in the context of either
breast-conserving surgery (BCS) or total mastectomy (TM) (1,6–18). Local recurrence (LR) occurs in 10–65%
of The patients and distant recurrence rates range between 5 and
40% postoperatively (7,8,11,12,19–24). Due
to the high risk of LR following surgical intervention alone, the
addition of adjuvant radiotherapy (RT) to the treatment of
borderline and malignant phyllodes tumors has been previously
investigated; however, The conclusions have been inconsistent.
Furthermore, an observational study reported a trend toward
increased utilization of RT, despite its uncertain effect on
outcome (25). The current guidelines
only recommend consideration of RT for malignant phyllodes in the
setting of LR (level 2B evidence) (26).
We thus performed a systematic review and
meta-analysis to assess the efficacy of adjuvant RT for borderline
and malignant phyllodes tumors.
Materials and methods
Study selection
The focus of this systematic review and
meta-analysis was to specifically assess the postoperative outcomes
of borderline and malignant phyllodes tumors with and without RT. A
systematic search of Pubmed and Web of Science was undertaken,
using the following terms: (phyllodes tumor OR phyllodes tumour OR
phyllodes tumors OR phyllodes tumours OR cystosarcoma phyllodes OR
cystosarcoma phyllode OR phyllode tumor OR phyllode tumour OR
phyllode tumors OR phyllode tumours OR biphasic Tumors OR biphasic
Tumor OR biphasic Tumour OR biphasic Tumours OR cystosarcoma
phylloides OR cystosarcoma phylloides tumor OR cystosarcoma
phylloides tumors OR cystosarcoma phylloides tumour OR cystosarcoma
phylloides tumours OR phylloides tumor OR phylloides tumors OR
phylloides tumour OR phylloides tumours) and (breast OR mammary OR
mammory OR mammary glands OR mammary gland OR mammory gland OR
mammory glands) and (Radiation therapy OR radiotherapy OR radiation
oncology OR radiation OR radiation treatment OR radiotreatment OR
ray therapeutics OR ray treatment), up to May 1, 2014.
Inclusion and exclusion criteria
The inclusion criteria were as follows: The studies
had to be primary research articles specifically investigating the
outcomes of postoperative borderline and malignant phyllodes tumors
with and without RT; at least one subgroup analysis comprising
borderline or malignant phyllodes tumors was to be reported.
Patients with positive margins were excluded. To increase the
number of potentially interesting articles, no limits or language
restriction were applied during the search.
Reviews and case reports on the subject were
excluded. Published abstracts without complete articles were
excluded due to our inability to obtain detailed information. All
The citations were independently reviewed by two authors (SYZ and
XDZ) and categorized as relevant, not relevant, or potentially
relevant. Citations that were classified as relevant and
potentially relevant by one of the authors were selected for
abstract review. Following review of the abstract, potentially
relevant and relevant abstracts were selected for full-text
evaluation. Upon evaluation of the full text, patients were
included if they were surgically treated for borderline or
malignant phyllodes tumor and information on the use of RT was
available; women with history of breast cancer or distant
metastatic disease at presentation were excluded.
Extracted data
The following information was extracted from each
eligible study: Authors' names, source of patients, number of
patients, patient age, type of surgery, margin status, radiation
dose, follow-up period and conclusion (Table I). The numbers of events were
extracted to conduct a meta-analysis of the different outcomes
under investigation. If the numbers of events were not available,
the LR rates or survival rates were used to estimate them.
 | Table I.Characteristics of the included
studies. |
Table I.
Characteristics of the included
studies.
| Study (Refs.) | Patient source | Patient no.,
total/RT/no RT | Patient age, mean or
median mean (year) | Tumor size, mean or
median (cm) | Grade, M/B | Type of surgery,
BCS/TM/UM | Margins,
NE/PO/UN | Radiation dose, Gy
(range) | Follow-up
(months) | Conclusion |
|---|
| Haberer et
al (30) | Paris, France | 22/5/17 | 52 | 6.5 | 22/0 | 5/17/0 | 20/0/2 | 52 (45–55) | Median, 65 | Uncertain |
| Soumarova et
al (31) | Brno, Czech
Republic | 25/17/8 | 52 | 10 | 25/0 | 4/21/0 | Not provided | 46–70 | Median, 139.5 | Adjuvant RT
decresed the LR incidence |
| Pandey et al
(32) | Trivandrum,
Iidia | 36/25/11 | 39 | 10.8 | 36/0 | 6/26/4 | 17/6/13 | 45–50 | Median, 43 | Adjuvant RT
decresed the risk of LR and also improved survival |
| Kim et al
(33) | Seoul, south
korea | 42/5/37 | 40.5 | 4.0 | 13/29 | 38/4/0 | 42/0/0 | Not provided | Median, 43 | Recurrence rates
were very low for begingn PT, regardless of surgical margin of
status or RT |
| Belkacemi et
al (14) | 17 Rare Cancer
Network Instutions (Europe) | 159/39/123 | 40 | 4.6 | 79/80 | 109/50/0 | Not provided | 50 (37–60) | Median 106 | Adjuvant RT after
BCS had no effect on survial |
| Gnerlich et
al (25) | National Cancer
Data Base (USA) | 3,210 (1,774
available)/459/2,751 | 51.1 | 4.2 | 3,210/0 | 1,838/1,363/9 | 2,787/275/148 | Not provided | Median, 53 | Adjuvant reduced LR
but RT had no effect on DFS OS |
| Badar et al
(34) | Lahore,
pakisthan | 32/21/11 | 40.3 | 9.2 | 32/0 | Not provided | Not provided | Not provided | Longest, 152.8 | Uncertain |
| Macdonald et
al (13) | National Cancer
Institute's SEER program (USA) | 618/68/550 | 50 | Not provided | 618/0 | 297/321/0 | Not provided | Not provided | Median, 68.4 | Uncertain |
Statistical analysis
Stata software, Version 12.0 (StataCorp, College
Station, Texas, USA) was used to pool the different outcome
estimates. The outcomes were analyzed as hazard ratios (HRS).
Statistical heterogeneity was assessed using the I2
statistic (27). We considered
I2 <25% to represent low heterogeneity, I2
>75% high heterogeneity and 25% <I2 <75%
moderate heterogeneity. The evidence classification was performed
using GRADEprofiler software, Version 3.6 (the Cochrane
Collaboration Network). We classed outcomes as high-, moderate-,
low- or very low-quality (28,29).
Next to relative outcome measures, we calculated
pooled absolute risks (ARs). The AR difference was calculated as
the pooled estimate of the AR difference for each study, including
a 95% confidence interval (CI). Subsequently, the number needed to
treat was calculated as 1 divided by the AR difference.
Results
Study selection process
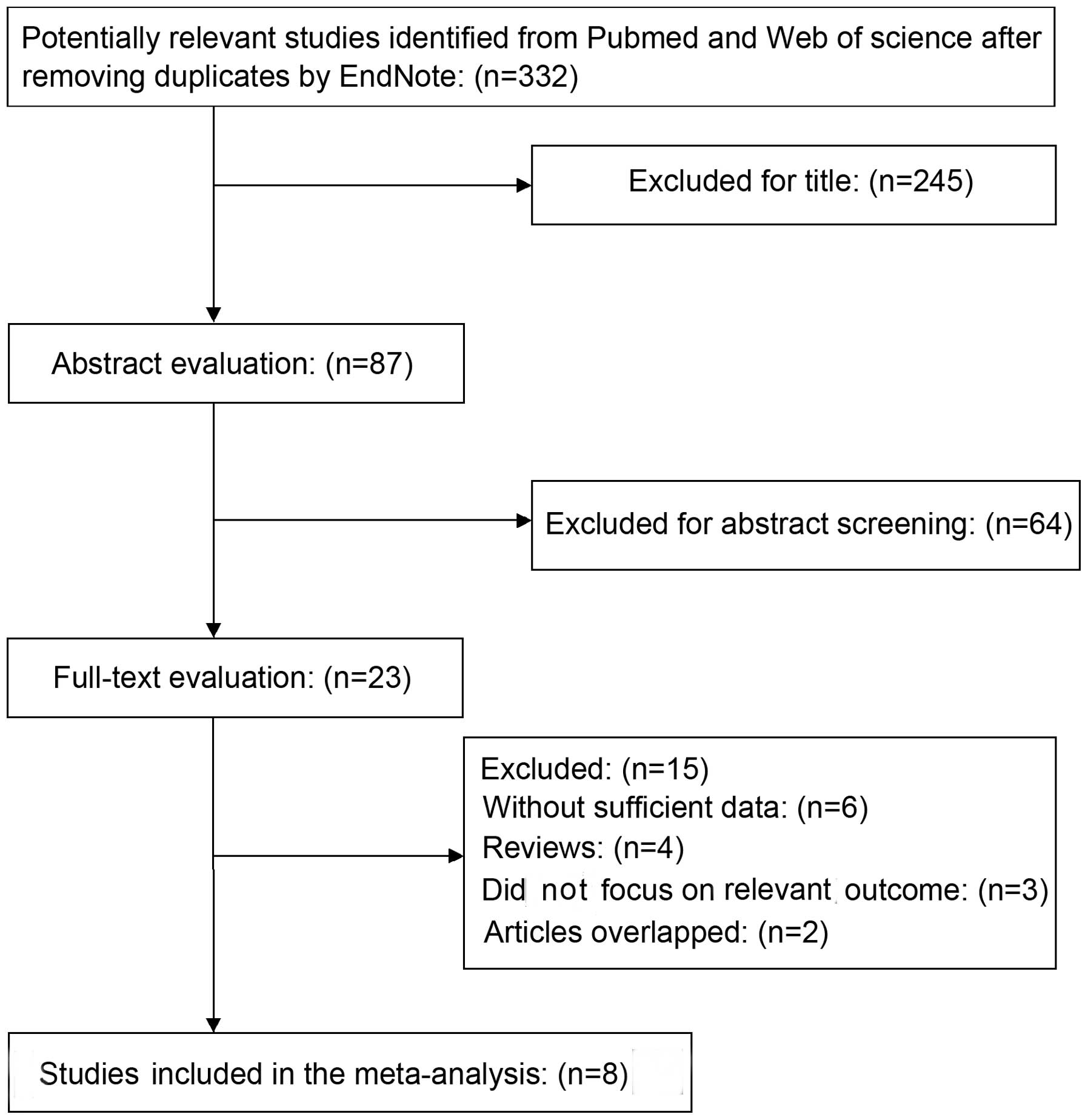
A total of 332 unique citations were identified
following a search through Pubmed and Web of science after removing
duplicates by EndNote; of the 332 articles, 87 were selected for
abstract review and, of those, full-text evaluation was undertaken
for 23 publications (Fig. 1).
Overall, 6 publications were excluded due to lack of sufficient
data; 4 were excluded as they were reviews; 3 were excluded as they
did not focus on The outcome under investigation and 2 were
excluded due to overlapping. Finally, a total of 8 studies were
included in the present systematic review and meta-analysis
(13,14,25,30–34).
Description of studies
The characteristics of the included studies are
listed in Table I. The total number
of participants included in this systematic review and
meta-analysis was 2,708. The studies were published between 2001
and 2014. Inclusion in all The studies was restricted to patients
with primary borderline and malignant phyllodes tumors, without
identified metastasis at presentation. All the patients underwent
surgery and the majority (~90%) had negative resection margins. A
proportion of The patients consented to undergo RT. None of the
patients had a history of breast cancer or other malignant tumors
and none had priorly received adjuvant RT. In the studies, only a
small proportion of the patients (<1%) also received
chemotherapy or endocrine therapy during the treatment. Therefore,
we decided to include all these patients in the meta-analysis.
Moreover, the primary outcome of the majority of the
studies was LR, which was defined as recurrence or a secondary
phyllodes tumor in the ipsilateral breast. Frequent secondary
outcomes were overall survival (OS) and disease-free survival
(DFS). Since our meta-analysis only included 8 studies, we did not
perform formal tests for funnel plot asymmetry.
Meta-analysis
Of the 8 studies included in the meta-analysis, 6
studies described LR. Since Gnerlich et al (25) reported the HR of LR and did not report
The exact number of LR in patients with and without RT, we
calculated the 5-year risk ratio (RR) of the remaining 5 involved
studies. The pooled analysis confirmed a lower relative risk of LR
in patients who received RT (RR=0.45, 95% CI: 0.26–0.77).
Subsequently, a pooled analysis of these 6 studies also
demonstrated a lower relative risk of LR in patients with RT
(HR=0.43, 95% CI: 0.23–0.64) with an I2 of 0%,
indicating low heterogeneity (Fig.
2). A meta-analysis on the different types of surgery is likely
to be very helpful in this regard, identifying subgroups of
patients undergoing BCS and TM. The meta-analysis was repeated
without the study results of Soumarova et al (31) and Pandey et al (32), as there was no available information
for comparable subgroups (BCS vs. TM). The pooled HR of LR in The
BCS group demonstrated a lower relative risk of LR in patients with
RT compared to those not receiving RT (HR=0.31, 95% CI:
−0.10–0.72); however, the combined HR for LR in The TM group did
not indicate that adjuvant RT was superior to no RT (HR=0.68, 95%
CI: −0.28–1.64; Fig. 3).
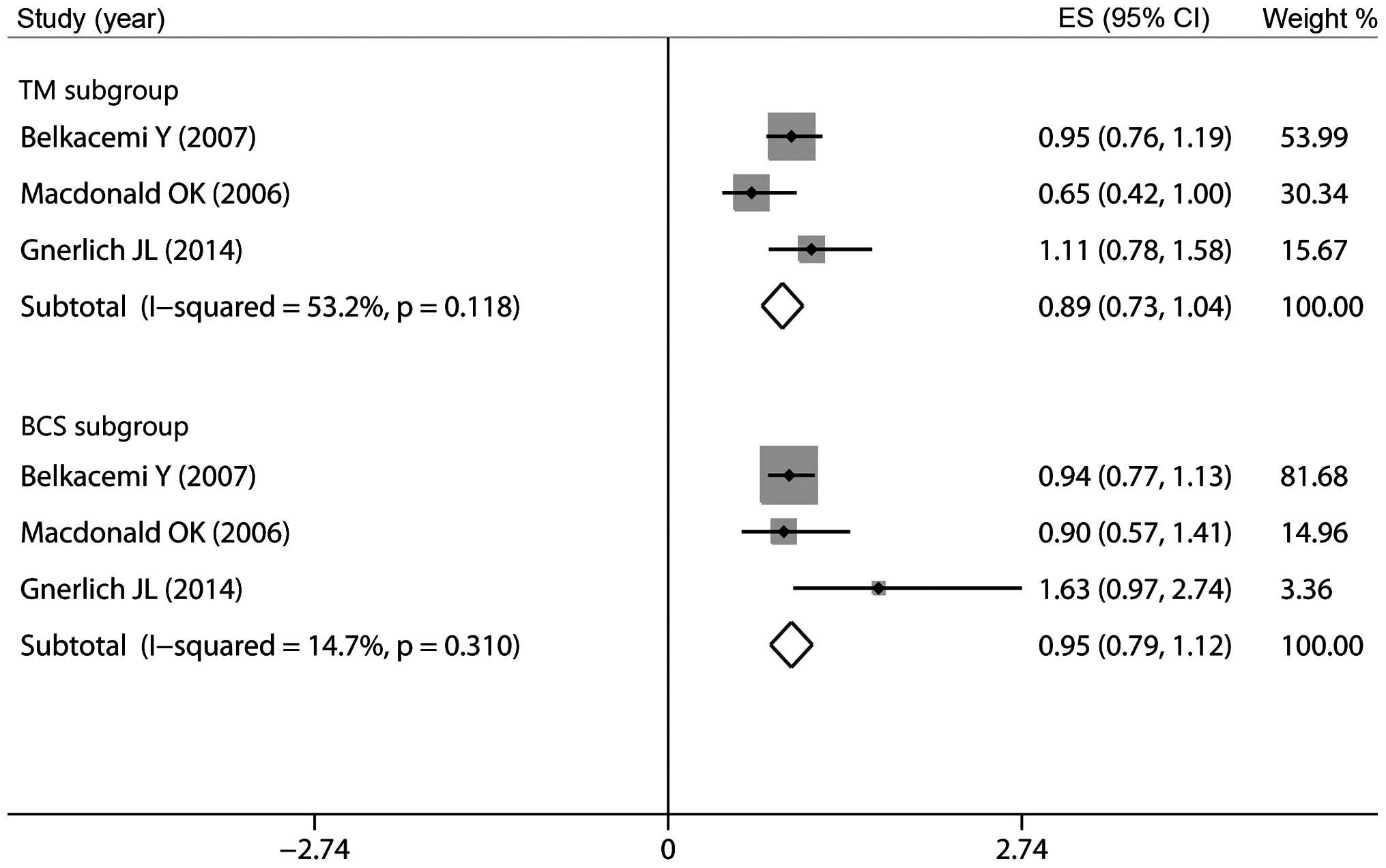
Of the included studies, 4 reported data on OS. The
results of our pooled meta-analysis demonstrated that surgery plus
RT vs. surgery alone was associated with a decreased 5-year OS
(HR=0.89, 95% CI: 0.79–0.99; Fig. 4)
with an I2 of 58.0%, indicating moderate heterogeneity.
The meta-analysis was repeated without the study results of Badar
et al (34), as there was no
available information for comparable subgroups (BCS vs. TM).
However, in the subgroups by different types of surgery, the pooled
HR of OS in The BCS group (HR=0.95, 95% CI: 0.79–1.12) and The TM
group (HR=0.89, 95% CI: 0.73–1.04; Fig.
5) revealed that adjuvant RT exerted no effect on 5-year
OS.
A total of 4 studies reported on the effect of RT on
DFS. The results of this pooled analysis demonstrated that adjuvant
RT following surgery exerted no effect on 5-year DFS (HR=0.93, 95%
CI: 0.74–1.12; Fig. 6) and the
I2 of DFS was 37.8%, indicating moderate heterogeneity.
A meta-analysis of specific subgroups was not possible, as
information from half of The studies were available for
incomparable subgroups alone. Based on the grading of
recommendations assessment, development and evaluation (grade)
system, the level of evidence of the involved studies was very low
(Table II).
| Table II.Quality assessment of the included
studies based on the GRADE system. |
Table II.
Quality assessment of the included
studies based on the GRADE system.
| Quality
assessment | No. of
patients | Effect |
|
|---|
|
|
|
|
|---|
| No. of studies | Studies design | Risk of bais | Inconsistency | Indirectness | Imprecision | Other
considerations | Surgergy+RT | Surgergy alone | Relative (95%
CI) | Absolute | Quality | Importance |
|---|
| LRa 5 | Observational | Highd | Not
significant | Highe | Highf | Increased effect
for RR~1g | 17/88 (19.3%) | 58/197 (29.4%) | HR=0.45
(0.26–0.77) | 149 fewer per 1,000
(59–208 fewer) | Very low | Critical |
|
|
|
|
|
|
|
|
| 28.4% |
| 144 fewer per 1,000
(57–207 fewer) |
| OSb 3 | Observational | Highd | Not
significant | Highe | Highf | Increased effect
for RR~1h | 65/125 (52%) | 405/684
(59.2%) | RR=0.804
(0.679−0.952) | 116 fewer 1,000
(28–190 fewer) | Very low | Critical |
| DFSc 3 | Observational | Highd |
Significanti | Highe | Highf | Reduced effect for
RR>>1 or RR<<1h | 49/82 (59.8%) | 92/144 (63.9%) | RR=1.033 (63.9%)
(0.828–1.288) | 21 more per 1,000
(100 fewer–184 more) | Very low | Critical |
|
|
|
|
|
|
|
|
| 62.9% |
| 21 more per 1,000
(108 fewer–181 more) |
|
|
AR
The pooled AR of LR, OS and DFS were calculated for
patients in both study arms. Since ARs are dependent on the
duration of follow-up, we calculated the 5-year AR of these
outcomes. The 5-year AR of a LR among patients who received RT was
19.3% (17 of 88, 95% CI: 11.6–29.1) compared to 29.4% (58 of 197,
95% CI: 23.1–36.3) among patients who did not receive RT. The AR
difference was 10.1% (95% CI: 4.9–17.6). The results were in favor
of those who received RT in addition to surgery, corresponding to a
number needed to treat of 10 to prevent one LR in 5 years.
The 5-year AR of OS was 52% (65 of 125, 95% CI:
42.9–61.0) in patients who received RT compared to 59.2% (405 of
684, 95% CI: 55.4–62.9) in those who did not. For DFS, the 5-year
ARs were 59.8% (49 of 82, 95% CI: 48.3–70.4) among patients who
received RT compared to 63.9% (92 of 144, 95% CI: 55.5–71.7) among
those who did not.
Discussion
To the best of our knowledge, this is the first
systematic review and meta-analysis to investigate the effects of
adjuvant RT on borderline and malignant phyllodes tumors. Our
pooled meta-analysis clearly demonstrated a decreased risk of LR in
patients with borderline and malignant phyllodes tumors who
received RT following BCS. The results of this pooled analysis
revealed that adjuvant RT exerts no effect on OS or DFS.
The standard treatment for borderline and malignant
phyllodes tumors is wide local excision (margins ≥1 cm), in the
context of either BCS or TM. However, the risk of LR following
margin-negative resection of borderline or malignant phyllodes
tumors is significant. Although the addition of adjuvant RT to the
treatment of borderline and malignant phyllodes tumors has been
investigated no consensus has been reached. Gnerlich et al
(25) reported a significant increase
in RT use for BCS as well as TM patients, despite its uncertain
efficacy. Therefore, we performed this systematic review and
meta-analysis to integrate the results from recent studies that
investigated the effect of adjuvant RT on borderline and malignant
phyllodes tumors.
Our pooled analysis confirmed a lower relative risk
of LR in patients receiving adjuvant RT following surgical
resection compared to surgery alone. The AR difference was 10.1%
(95% CI: 4.9–17.6). The results were in favor of patients who
received RT in addition to surgery, corresponding to a number
needed to treat of 10 to prevent one LR in 5 years. This number is
expected to be relatively higher in a non-trial population. To
decrease the number needed to treat and to personalize treatment,
we attempted to identify subgroups of patients (BCS vs. TM) in
which RT may be safely omitted on the basis of the risk of LR. The
pooled HR of LR in The BCS group revealed a lower relative risk of
LR (HR=0.31, 95% CI: −0.10–0.72); however, the combined HR for LR
in The TM group did not demonstrate that adjuvant RT was superior
to no RT (HR=0.68, 95% CI: −0.28–1.64). Thus, omission of RT in
patients following TM may be reasonable. However, these results
must be interpreted with caution, considering that we only
calculated The 5-year LR rate in TM patients. Belkacémi et
al (14) observed similar 5-year
local control rates in irradiated patients following TM compared to
those who did not receive RT (92 vs. 91%, respectively); however,
adjuvant RT improved the 10-year local control for borderline and
malignant tumors (92 vs. 78%, respectively). Thus, following TM,
adjuvant RT should be discussed taking into account The surgical
margins, size and pathological criteria of the tumor. Pezner et
al (22) recommend adjuvant RT
following TM for large tumors (>10 cm).
Our results were consistent with those of the
individual studies. We also identified 1 study that reported
marginally different results. Reinfuss et al (35) reported on patients who were treated
with the Halsted operation followed by postoperative RT, which
proved to be inefficient. In their study, patients who received
postoperative irradiation exhibited infiltration of The pectoralis
major muscle and limited mobility of the chest wall; in addition,
The surgical margin was not microscopically tumor-free. After 5
years of follow-up, all The patients exhibited LRs along with
pulmonary metastases. Only few of The patients involved in our
study exhibited infiltration of The pectoralis major muscle and the
majority of the patients (~90%) had negative resection margins. The
difference between their results and ours may be explained by the
worse overall condition of the patients in the study of reinfuss
et al (35). The study of
Barth et al (20) yielded
similar conclusions to ours. In their prospective study, 46 women
(30 with malignant and 16 with borderline phyllodes tumors) were
treated with margin-negative breast-conserving resection followed
by adjuvant RT. The patients were treated in 30 different
institutions; after a minimum follow-up of 5 years, none of the
patients exhibited LR. A retrospective study by Chaney et al
(36) that involved 6 patients
treated with adjuvant RT for non-metastatic phyllodes tumor of the
breast yielded similar results. There was no reported local or
distant failure after a median follow-up of 36.5 months. Therefore,
adjuvant RT should be considered to minimize LRs following
breast-conserving resection of borderline and malignant phyllodes
tumors.
To our surprise, our pooled meta-analysis
demonstrated that surgery plus RT was associated with decreased
5-year OS compared to surgery alone (HR=0.89, 95% CI: 0.79–0.99).
To The best of our knowledge, there is no study reporting that
postoperative RT decreases OS. None of our included individual
studies indicated that adjuvant RT exerted a detrimental effect on
OS. Moreover, the study by Pandey et al (32) demonstrated that adjuvant RT not only
decreased the risk of LR, but also improved survival. We performed
a subgroup analysis by exclusion of the study by Badar et al
(34), as it lacks information on
comparable subgroups (BCS vs. TM). The pooled HRs of OS in The BCS
group (HR=0.95, 95% CI: 0.79–1.12) and The TM group (HR=0.89, 95%
CI: 0.73–1.04) revealed that adjuvant RT exerted no effect on OS.
This may be due to the small sample size in each group.
Furthermore, RT is often administered to patients of poor
prognosis. The wide CI may be due to variations in the survival
data. Additional randomized controlled studies (RCTS) are required
to further elucidate this issue.
Our pooled analysis proved that RT following surgery
exerted no effect on 5-year DFS. The 4 included individual studies
did not report that adjuvant RT exerted a detrimental effect on
DFS. Thus far, we have not identified any studies reporting
different results. The 5-year AR of LR among patients who received
RT was 19.3% (17 of 88, 95% CI: 11.6–29.1), vs. 29.4% (58 of 197,
95% CI: 23.1–36.3) among patients who did not receive RT. The data
of Kim et al (33) and Barth
et al (20) demonstrated that
the AR of LR following margin-negative breast-conserving resection
of borderline and malignant phyllodes tumors was 16/73 (22%) and
30/134 (22%), respectively. However, our pooled AR data were
higher. This may be explained as follows: although we tried to
eliminate patients with positive resection margins, such patients
could not be eliminated in 2 of the included studies, whereas the
other 2 included studies did not provide data on margin status. An
estimated 10% of those patients had positive margins. In this case,
our study indicates that adjuvant RT may be effective for patients
with positive tumor resection margins.
The goal of adjuvant RT is to reduce disease
recurrence and improve The quality of life of the patients. From
the time adjuvant RT was first introduced as part of breast cancer
treatment, this procedure has gained in popularity and it has been
shown to reduce disease recurrence and improve The quality of life.
A number of studies have supported the oncological effectiveness
and safety of this procedure in phyllodes tumors (20,32,36).
Certain clinical practitioners remain cautious regarding adjuvant
RT in phyllodes tumors. Our analysis supports the conclusion that
postoperative RT for borderline and malignant phyllodes tumors
decreases the LR rate for patients undergoing BCS. However,
adjuvant RT is not the only factor determining whether patients
will develop a relapse; other factors, including age, surgical
approach, mitotic activity and surgical margins are significantly
correlated with recurrence (P=0.029, 0.020, 0.048 and 0.00018,
respectively) (15). Local excision,
wide excision, or TM with negative surgical margins yielded high
local control rates, but local excision was associated with a
relatively high percentage of positive surgical margins (18.3%)
(15). Pezner et al (22) retrospectively analysed 478 patients
with malignant phyllodes tumors of the breast and found that The
5-year local control rates were 100% for 0–2-cm tumors, 95% for
2–5-cm tumors, 88% for 5–10-cm tumors and 85% for 10–20-cm tumors.
A multivariate analysis of OS found several factors to be
significant, including advancing age with each decade after 50
years, appearance of distant metastases, larger tumor size and
local control vs. LR (HR=2.5, P<0.05) (22). Surgical management must be tailored to
the clinical situation, with more aggressive management reserved
for higher-grade or recurrent tumors (19). In the latter case, if wide local
excision is possible while allowing satisfactory cosmesis, BCS
could also be considered. Pezner et al (22) recommend adjuvant RT following BCS for
tumor sizes >2 cm.
There were certain limitations to this analysis.
First, we did not consider certain confounding factors, such as
chemotherapy and endocrine therapy, as the original data were
unavailable, although these patients accounted for an estimated
<1%. However, these factors may affect the rate of recurrence.
Second, selection bias, particularly the tendency to administer
adjuvant RT to patients with later-stage tumors, was a problem in
the majority of the studies. Third, the different follow-up
duration may also limit the interpretation of the results. Fourth,
all the studies in our analysis were non-RCTs, the results of which
are not as convincing as those of RCTs. Finally, according to the
grade system, the level of the included studies' evidence was very
low. Therefore, further investigation may alter our
conclusions.
In conclusion, this meta-analysis suggests that
adjuvant RT for borderline and malignant phyllodes tumors decreases
the LR rate for patients undergoing BCS. However, adjuvant RT
exerts no effect on OS or DFS. The majority of The studies were
performed via retrospective analysis to investigate small numbers
of patients. Therefore, we believe that a multicenter prospective
RCT with a longer follow-up period and more clearly defined
parameters may be the best way to further elucidate this issue in
the future.
References
|
1
|
Moffat CJ, Pinder SE, Dixon AR, Elston CW,
Blamey RW and Ellis IO: Phyllodes tumours of the breast: a
clinicopathological review of thirty-two cases. Histopathology.
27:205–218. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bernstein L, Deapen D and Ross RK: The
descriptive epidemiology of malignant cystosarcoma phyllodes tumors
of the breast. Cancer. 71:3020–3024. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bartoli C, Zurrida SM and Clemente C:
Phyllodes tumor in a male patient with bilateral gynaecomastia
induced by oestrogen therapy for prostatic carcinoma. Eur J Surg
Oncol. 17:215–217. 1991.PubMed/NCBI
|
|
4
|
Keelan PA, Myers JL, Wold LE, Katzmann JA
and Gibney DJ: Phyllodes tumor: clinicopathologic review of 60
patients and flow cytometric analysis in 30 patients. Hum Pathol.
23:1048–1054. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tan PH, Jayabaskar T, Chuah KL, et al:
Phyllodes tumors of the breast: the role of pathologic parameters.
Am J Clin Pathol. 123:529–540. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rowell MD, Perry RR, Hsiu JG and Barranco
SC: Phyllodes tumors. Am J Surg. 165:376–379. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Reinfuss M, Mitus J, Duda K, Stelmach A,
Rys J and Smolak K: The treatment and prognosis of patients with
phyllodes tumor of the breast: an analysis of 170 cases. Cancer.
77:910–916. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Barth RJ Jr: Histologic features predict
local recurrence after breast conserving therapy of phyllodes
tumors. Breast Cancer Res Treat. 57:291–295. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tan PH, Thike AA, Tan WJ, et al: Phyllodes
Tumour Network Singapore: Predicting clinical behaviour of breast
phyllodes tumours: a nomogram based on histological criteria and
surgical margins. J Clin Pathol. 65:69–76. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Abdalla HM and Sakr MA: Predictive factors
of local recurrence and survival following primary surgical
treatment of phyllodes tumors of the breast. J Egypt Natl Canc
Inst. 18:125–133. 2006.PubMed/NCBI
|
|
11
|
Chaney AW, Pollack A, McNeese MD, et al:
Primary treatment of cystosarcoma phyllodes of the breast. Cancer.
89:1502–1511. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Asoglu O, Ugurlu MM, Blanchard K, et al:
Risk factors for recurrence and death after primary surgical
treatment of malignant phyllodes tumors. Ann Surg Oncol.
11:1011–1017. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Macdonald OK, Lee CM, Tward JD, Chappel CD
and Gaffney DK: Malignant phyllodes tumor of the female breast:
association of primary therapy with cause-specific survival from
the Surveillance, Epidemiology, and End Results (SEER) program.
Cancer. 107:2127–2133. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Belkacémi Y, Bousquet G, Marsiglia H, et
al: Phyllodes tumor of the breast. Int J Radiat Oncol Biol Phys.
70:492–500. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chen WH, Cheng SP, Tzen CY, et al:
Surgical treatment of phyllodes tumors of the breast: retrospective
review of 172 cases. J Surg Oncol. 91:185–194. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mangi AA, Smith BL, Gadd MA, Tanabe KK,
Ott MJ and Souba WW: Surgical management of phyllodes tumors. Arch
Surg. 134:487–492. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kapiris I, Nasiri N, A'Hern R, Healy V and
Gui GP: Outcome and predictive factors of local recurrence and
distant metastases following primary surgical treatment of
high-grade malignant phyllodes tumours of the breast. Eur J Surg
Oncol. 27:723–730. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Barrio AV, Clark BD, Goldberg JI, et al:
Clinicopathologic features and long-term outcomes of 293 phyllodes
tumors of the breast. Ann Surg Oncol. 14:2961–2970. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Guillot E, Couturaud B, Reyal F, et al:
Management of phyllodes breast tumors. Breast J. 17:129–137. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Barth RJ Jr, Wells WA, Mitchell SE and
Cole BF: A prospective, multi-institutional study of adjuvant
radiotherapy after resection of malignant phyllodes tumors. Ann
Surg Oncol. 16:2288–2294. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ellis I, Sawyer EJ, Rampaul R and Pineda
CG: Phyllodes tumor of the breastTextbook of Uncommon Cancer.
Raghavan D, Brecher ML, Johnson DH, MerOpol NJ, Moots PL and Rose
PG: 3rd. Wiley; Chichester: pp. 209–217. 2006, View Article : Google Scholar
|
|
22
|
Pezner RD, Schultheiss TE and Paz IB:
Malignant phyllodes tumor of the breast: local control rates with
surgery alone. Int J Radiat Oncol Biol Phys. 71:710–713. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Parker SJ and Harries SA: Phyllodes
tumours. Postgrad Med J. 77:428–435. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Barth R J Jr: Margin negative, breast
conserving resection: adequate for benign phyllodes tumors, but
inadequate therapy for borderline and malignant phyllodes tumors.
Breast Cancer Res Treat. 142:463–464. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Gnerlich JL, Williams RT, Yao K, Jaskowiak
N and Kulkarni SA: Utilization of radiotherapy for malignant
phyllodes tumors: analysis of the National Cancer Data Base,
1998–2009. Ann Surg Oncol. 21:1222–1230. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Carlson RW, Allred DC, Anderson BO, et al:
Metastatic breast cancer, version 1.2012: featured updates to the
NCCN guidelines. J Natl Compr Canc Netw. 10:821–829.
2012.PubMed/NCBI
|
|
27
|
Higgins JP and Thompson SG: Quantifying
heterogeneity in a meta-analysis. Stat Med. 21:1539–1558. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Atkins D, Best D, Briss PA, et al: Grade
Working Group: Grading quality of evidence and strength of
recommendations. BMJ. 328:14902004. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Jaeschke R, Guyatt GH, Dellinger P, et al:
Use of grade grid to reach decisions on clinical practice
guidelines when consensus is elusive. BMJ. 337:a7442008.(In
French). View
Article : Google Scholar : PubMed/NCBI
|
|
30
|
Haberer S, Laé M, Seegers V, et al:
Management of malignant phyllodes tumors of the breast: the
experience of the Institut Curie. Cancer Radiother. 13:305–312.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Soumarová R, Seneklová Z, Horová H, et al:
Retrospective analysis of 25 women with malignant cystosarcoma
phyllodes - treatment results. Arch Gynecol Obstet. 269:278–281.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Pandey M, Mathew A, Kattoor J, et al:
Malignant phyllodes tumor. Breast J. 7:411–416. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kim S, Kim JY, do H Kim, Jung WH and Koo
JS: Analysis of phyllodes tumor recurrence according to the
histologic grade. Breast Cancer Res Treat. 141:353–363. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Badar F, Mahmood S, Syed AA and Siddiqui
N: Malignant phyllodes tumour of the breast. J Ayub Med Coll
Abbottabad. 24:47–49. 2012.PubMed/NCBI
|
|
35
|
Reinfuss M, Mituś J, Smolak K and Stelmach
A: Malignant phyllodes tumours of the breast. A clinical and
pathological analysis of 55 cases. Eur J Cancer. 29A:1252–1256.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Chaney AW, Pollack A, McNeese MD and
Zagars GK: Adjuvant radiotherapy for phyllodes tumor of breast.
Radiat Oncol Investig. 6:264–267. 1998. View Article : Google Scholar : PubMed/NCBI
|