Introduction
The incidence of thyroid nodules has significantly
increased over the last decades (1).
Thyroid nodules may be detected in 19–67% of the cases by
high-resolution ultrasound, and thyroid cancer must be excluded in
all these nodules (2). Thyroid
nodules are mostly benign and asymptomatic and, thus, do not
require any treatment. Fine-needle aspiration (FNA) has become an
essential diagnostic modality in the evaluation of thyroid nodules
and is implicated in all three major guidelines in patient
management, namely the American Thyroid Association (ATA), the
European Thyroid Association (ETA) and the Society of Radiologists
in Ultrasound (SRU) (3); however,
there is currently no consensus regarding the exact indications of
FNA in these three main guidelines. The Bethesda System for
Reporting Thyroid Cytopathology (TBSRTC), which was created through
multidisciplinary formulation, is the most popular cytology
reporting system worldwide (4).
The primary success of TBSRTC was reducing
unnecessary thyroid surgery. The malignancy detection rate
increased from 14 to 50% prior to and following adoption of FNA as
a diagnostic modality, respectively, and was even higher after the
introduction of TBSRTC (5). However,
the effectiveness of TBSRTC in reducing unnecessary and repeat
FNAs, which was the secondary aim, appears to be limited. TBSRTC
appears to lack solid support by the main guidelines due to the
lack of standardization and clear-cut indications of FNA (3,6). US
scoring systems have been devised in an attempt to overcome this
weakness. Despite its high diagnostic ability and
cost-effectiveness, TBSRTC may be becoming a screening test, which
may be associated with high cost rates due to the significant
number of FNAs performed in daily routine practice; moreover, it
may increase false-positive results in cytological specimens and
false-negative/vanishing tumor diagnosis in pathological specimens
(6,7).
A number of different imaging modalities have been
used to evaluate thyroid nodules to avoid unnecessary FNA and
surgery. The Thyroid Imaging Reporting and Data System (TI-RADS)
was introduced in 2009 by Horvath et al (8), based on the concepts of the Breast
Imaging Reporting and Data System, which conducts a risk assessment
of malignancy in breast FNAs. Horvath et al proposed 10
characteristics, and Park et al (9) subsequently established a new system
with 12 characteristics, which were aimed at standardizing the
evaluation of thyroid nodules with US. However, the application of
those characteristics to all thyroid nodules was found to be
problematic.
Sonoelastography, first proposed in 1991 by Ophir
et al, operates on the relative hardness of the nodule
compared with the adjacent thyroid parenchyma to improve diagnostic
accuracy (7,10). There are two technically different
methods, both aimed at measuring the stiffness of the tissues:
Strain and shear-wave elastography. Strain elastography (SE)
consists of a quantitative measure (strain index) and a qualitative
color picture superimposed on the B-mode image. The proof of
elevated/increased stiffness should guide FNA, even in nodules
without suspicious findings on ultrasound (11).
Therefore, the main question is which nodules should
be referred for FNA, which was addressed by investigating 369 cases
using TI-RADS and SE with TBSRTC.
Materials and methods
Case selection
The study was designed to include prospective FNA
diagnostics in patients with nodules/focal lesions of the thyroid
gland, who were referred for biopsy to the Haydarpasa Numune
Training and Research Hospital (Istanbul, Turkey) between January
and June, 2014. All aspects of the study were reviewed and approved
by the hospital's Institutional Review Board. A total of 369 cases
were evaluated by 3 radiologists (with 17, 2 and 16 years of
experience) and FNAs were performed. Using the recorded images, a
single radiologist determined the corresponding TI-RADS category
(Horvath) (Table I).
 | Table I.US patterns in each TI-RADS (Horvath)
category and clinical recommendations based on these
categories. |
Table I.
US patterns in each TI-RADS (Horvath)
category and clinical recommendations based on these
categories.
| Description of US
pattern | US patterns | Malignancy | TI-RADS | Recommendation |
|---|
| Echoic with
hyperechoic spots, non-vascularized lesion | Colloid type 1 | 0% | TI-RADS 2: Benign
findings | Follow-up without
FNA |
| Non-encapsulated,
mixed, non- expansile, with hyperechoic spots, vascularized lesion,
grid aspect (spongiform nodule) | Colloid type 2 |
|
|
|
| Non-encapsulated,
mixed with solid portion, isoechogenic, expansile, vascularized
nodule with hyperechoic spots | Colloid type 3 |
|
|
|
| Hyper-, iso-, or
hypoechoic, partially encapsulated nodule with peripheral
vascularization, in Hashimoto's thyroiditis | Hashimoto
pseudonodule |
<5% | TI-RADS 3: Likely
benign | Follow-up, FNA may be
performed according to clinical suspicion |
| Solid or mixed
hyper-, iso-, or hypoechoic nodule, with a thin capsule | Simple neoplastic
pattern |
5–10% | TI-RADS 4A:
Undetermined | FNA |
| Hypoechoic lesion
with ill-defined borders, without calcifications | de Quervain
pattern |
|
|
|
| Hyper-, iso-, or
hypoechoic, hypervascularized, encapsulated nodule with a thick
capsule, containing calcifications (coarse or
microcalcifications) | Suspicious neoplastic
pattern |
|
|
|
| Hypoechoic,
non-encapsulated nodule, with irregular shape and margins,
penetrating vessels, with or without calcifications | Malignant pattern
A | 10–80% | TI-RADS 4B:
Suspicious | FNA |
| Iso- or hypoechoic,
non-encapsulated nodule with multiple peripheral
microcalcifications and hypervascularization | Malignant pattern
B |
>80% | TI-RADS 5: Consistent
with malignancy | FNA |
| Non-encapsulated,
isoechoic, mixed hypervascularized nodule with or without
calcifications, without hyperechoic spots | Malignant pattern C
cancer, confirmed by previous biopsy | 100% | TI-RADS 6:
Malignant |
|
Procedures
All the patients were ultrasonographically examined
(iU22 ultrasound device; Philips, Bothell, WA, USA), elastography
was performed and the strain ratio was recorded. Heterogeneous
thyroid parenchyma, substernal elongation of the nodule or
recurrent nodules following partial/total thyroidectomy hinder
elastographic measurement due to the lack of proper
reference/background tissue and a maximum SE value (E-max) could
not be provided for these cases.
FNAs were performed with a 22-gauge needle and two
smears were prepared for each pass. Rapid on-site evaluation was
performed by a cytopathologist using Diff-Quik stain. Cell blocks
were prepared from the excess material in the syringe. All the
cases were signed by the same cytopathologist according to
TBRSTC.
Statistical analysis
Statistical analysis was performed using the SPSS
software, version 20 (IBM SPSS, Armonk, NY, USA). The variables
were investigated using visual or analytical methods to determine
whether they were normally distributed. As the E-max value was not
normally distributed, the Mann-Whitney U test was conducted to
compare values among TBSRTC categories. The agreement between
TI-RADS and TBSRTC was tested by using Cohen's Kappa statistics. An
overall 5% type-1 error level was used to infer statistical
significance.
Results
Patient characteristics
A total number of 369 thyroid FNA cases performed
between January and June, 2014 were included in the present study.
The majority (86.7%; n=320) of the patients were female and the
mean age of the patients ± standard deviation was 56.9±11 years.
According to TBSRTC, 17.1% (n=63), 59.3% (n=219), 7.1% (n=26), 5.1%
(n=19), 2.7% (n=10) and 8.7% (n=32) of the cases were reported as
non-diagnostic (ND), benign (B), atypia of undetermined
significance/follicular lesion of unknown significance, follicular
neoplasia/suspicious for follicular neoplasia, suspicious for
malignancy (SFM) and malignant (M), respectively. The same cases
were evaluated as category 2 (39%; n=144), category 3 (4.1%; n=15),
category 4 (45%; n=166) and category 5 (1.6%; n=6) according to
TI-RADS (Table II). A total of
13.8% (n=51) of the patients underwent consequent thyroidectomy,
and the subsequent histopathological diagnosis was benign in 39.2%
(n=20) and malignant in 70.8% (n=31) of the cases. Malignant
diagnosis included 30 papillary thyroid carcinomas (6 classic, 4
encapsulated follicular, 4 aggressive, 7 follicular, 8 oncocytic
and 1 Warthin-like variants) and 1 medullary thyroid carcinoma.
There was no discrepancy between cytopathological and
histopathological diagnosis. The distribution of the cases
according to TBRSCT in each TI-RADS category is summarized in
Table III. There was some
agreement between the TI-RADS and TBRSCT classification systems
(32.5%) and the kappa value for benign and malignant diagnosis was
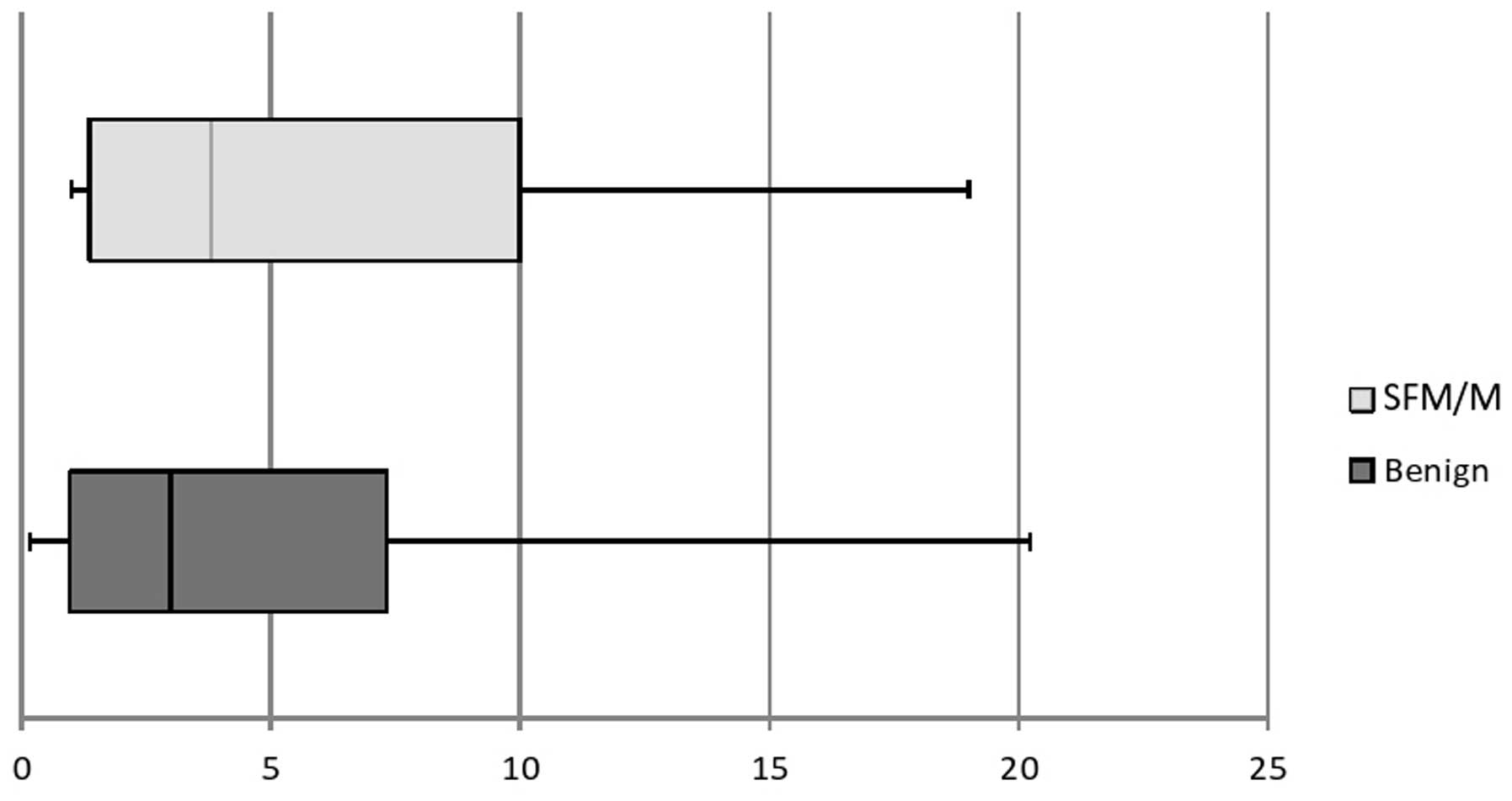
0.1. In 16% (n=59) of the cases, E-max value could not be provided
due to the lack of normal thyroid parenchyma due to multinodular
goiter and chronic lymphocytic thyroiditis. For the evaluated
cases, the median E-max value for benign nodules was 1.97
[interquartile range (IQR): 1.87], whereas in SFM and M nodules it
was 2.8 (IQR: 3.42), and the difference was found to be
statistically significant (P=0.004; Fig.
1).
| Table II.Patient characteristics. |
Table II.
Patient characteristics.
| Characteristics | No. (%) |
|---|
| Gender |
|
|
Female | 320 (86.7) |
| Male | 49 (13.3) |
| Age, years |
|
| Mean
(range) | 56.9 (40–62) |
| Lobe |
|
|
Right | 182 (49.3) |
| Left | 170 (46.0) |
|
Isthmus | 17 (4.7) |
| Nodule size, mm |
|
| Mean
(range) | 17.9 (4–50) |
| % of cases in TI-RADS
categories |
|
| 2 | 144 (39.0) |
| 3 | 15 (4.1) |
| 4a | 166 (45.0) |
| 4b | 38 (10.3) |
| 5 | 6 (1.6) |
|
Total | 369 (100.0) |
| % of cases in TBSRTC
categories |
|
| ND | 63 (17.1) |
| B | 219 (59.3) |
|
AUS/FLUS | 26 (7.1) |
|
FN/SFN | 19 (5.1) |
| SFM | 10 (2.7) |
| M | 32 (8.7) |
|
Total | 369 (100.0) |
| Table III.Distribution of cases between TI-RADS
and TBSRTC. |
Table III.
Distribution of cases between TI-RADS
and TBSRTC.
| TBCSRTC | No. of cases in each
category (%) | Malignancy ratio
according to Horvath et al (8) |
|---|
| TI-RADS 2 |
| 0% |
| ND | 21 (14.5) |
|
| B | 105 (73.0) |
|
|
AUS/FLUS/FN/SFN | 10 (7.0) |
|
|
SFM/M | 8 (5.5) |
|
| TI-RADS 3 |
|
<5% |
| ND | 3 (20.0) |
|
| B | 9 (60.0) |
|
|
AUS/FLUS/FN/SFN | 2 (13.3) |
|
|
SFM/M | 1 (6.7) |
|
| TI-RADS 4a |
|
5–10% |
| ND | 33 (19.9) |
|
| B | 91 (54.8) |
|
|
AUS/FLUS/FN/SFN | 25 (15.1) |
|
|
SFM/M | 17 (10.2) |
|
| TI-RADS 4b |
| 10–80% |
| ND | 5 (13.1) |
|
| B | 15 (39.5) |
|
|
AUS/FLUS/FN/SFN | 8 (21.0) |
|
|
SFM/M | 10 (26.4) |
|
| TI-RADS 5 |
|
>80% |
| ND | 1 (16.6) |
|
| B | 0 (0.0) |
|
|
AUS/FLUS/FN/SFN | 0 (0.0) |
|
|
SFM/M | 5 (83.4) |
|
Discussion
Walfish et al (12) first proposed ultrasonography
(US)-guided FNA in 1977; since then, US-guided FNA has
significantly accelerated daily practice. The following US
characteristics are widely used to highlight the risk of malignancy
in thyroid nodules: Vascularity, microcalcifications, composition,
echogenity, margins, presence of a peripheral halo and
calcifications. There has been a general consensus/agreement in
ATA, ETA or SRU, that suspicious US characteristics are an
indication for FNA (2,6,13,14).
However, those guidelines have various combinations of suggestions
in evaluating malignancy of thyroid nodules that may cause
confusion between clinicians. Recently, to establish a better
communication between radiologists and clinicians, several US
proposals and/or scoring systems have been proposed in the
literature (9,15).
TI-RADS was introduced by Horvath et al in
2009 to create a standardized reporting system, inspired by BIRADS,
based on the malignancy risk assessment of thyroid nodules
(8). At the beginning, TI-RADS
appeared to be promising through focusing not only on benign
nodules, but also on follicular lesions. The main disadvantages of
TI-RADS were difficulty in evaluating 10 US parameters for every
nodule, and its complexity that does not provide a clear
discrimination for the malignancy risk assessment, let alone
focusing on follicular lesions. Over time, TI-RADS was modified by
a number of authors in several studies. Park et al proposed
a new system based on 12 US characteristics (9). Another modified TI-RADS was introduced
by Kwak et al (15), which
appeared to have a more practical basis on 5 US characteristics
compared with the previous versions.
The present study was designed to compare the
compatibility and feasibility of the Horvath TI-RADS with TBSRTC
and its usefulness for avoiding unnecessary FNAs with the
contribution of elastography. Kwak et al reported the
increased malignancy risk in correlation with an increased number
of suspicious US characteristics (15). Friedrich-Rust et al (16) reported promising results in terms of
interobserver agreement with 3 observers for 114 thyroid nodules,
but still point out the need for further studies to create an
optimal system integrating all TI-RADS categories. The negative
predictive value (NPV) was 92–100% for TI-RADS categories 4 and 5
in the diagnosis of malignancy in the same study.
Our study also demonstrated some agreement between
every category of the TI-RADS system and TBSRTC. The suggested
malignancy risks were 5–10% and 10–80% in categories 4a and 4b of
Horvath TI-RADS, respectively, which were compatible with our
results in TI-RADS 4a and 4b (10.2–26%). Our malignancy ratio in
TI-RADS 2 was 5.5% while Horvath's was 0%. Compared with other
modified TI-RADS, Horvath's proposal appears to be quite strict
(8,9,15) Hence,
further large-scale studies are required on this topic. ND and
benign cytology results represented marked cumulation in the
TI-RADS 4a group that may have originated from external and
internal changes of the nodule: Recently, Eze et al stated
the importance of FNA-induced changes that may give rise to
false-positive results on thyroid cytology and false-negative
results/understaging of the tumor on thyroid pathology (17). Unnecessary and repeat FNAs may cause
what is referred to as ‘external factors/changes’, causing
degenerative processes in the nodule through organizing hemorrhage,
granulation tissue, fibrosis and sclerosis. The same cellular
processes may be seen as spontaneous degenerative changes of the
nodule, referred to as ‘internal factors/changes’ (18). All these external and internal
changes of the nodule may resemble suspicious imaging findings that
may easily be categorized as TI-RADS 4a (19). Overlapping US characteristics of
malignant and benign nodules is an ongoing problem, despite several
large-scale studies that were successful in discriminating
malignancy in thyroid nodules. The results of internal and external
changes of the nodule may be reflected as false-positive results in
cytopathology and vanishing tumors/understaging of the tumor in
pathology (17,18). The amount of unnecessary FNAs has
been steadily increasing due to the increased detection of nodules
by high resolution US. This may lead to transforming a successful
diagnostic test into a screening modality, which may have legal
implications and is associated with high medical costs (7). Our results demonstrated that TI-RADS 4a
must be elucidated to eliminate the overlapping characteristics of
reactive changes and malignancy in this group.
Elastography has been proposed as a new dynamic
technique to assess the elasticity of the nodule in comparison with
the adjacent parenchyma and is a well-accepted method for the
breast and prostate gland. Previously published studies suggest
certain limitations based on technical and histological factors
(7) (Table IV). However, several studies
demonstrated the usefulness of SE in avoiding unnecessary FNA and
discriminating malignant from benign nodules. The sensitivity and
specificity vary from 43.2–100% up to 70–92%, respectively, along
with wide alterations of the positive predictive value (40–60%);
however, the most common point is the high NPV results (90–99%) in
almost all studies (20–23). Despite all its limitations, we
consider SE to be a reliable method in the diagnosis of benign
nodules, taking into consideration the high NPV ratios in the
majority of the studies.
| Table IV.Limitations of strain
elastography. |
Table IV.
Limitations of strain
elastography.
| Technical | Histological |
|---|
|
Intra-/interobserver variability | Thyroiditis |
| Lack of
standardization | Calcification |
| Clinical conditions
of the patient: | Cystic
degeneration |
| Arrhytmia,
aterosclerosis, hypertension |
|
| Carotid artery
pulsations | Isthmic
localization |
|
| Nodule size |
|
| Follicular
carcinoma (due to the softness of the tumor) |
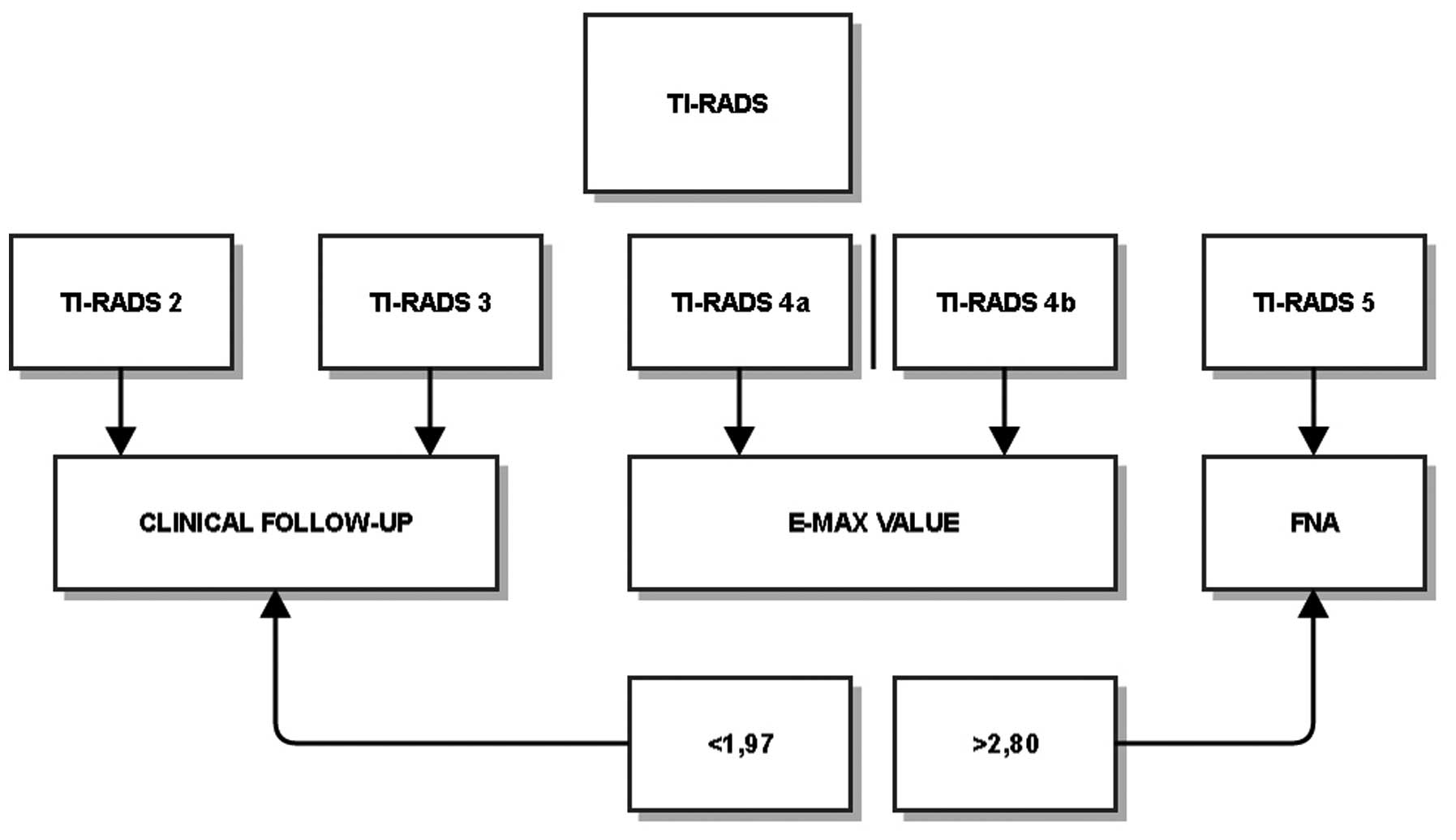
Although our results were presented as a scheme
(Fig. 2), we do not propose an
algorithm for patient management, since a group of 369 patients is
not sufficiently large to suggest one. There is some agreement
between TI-RADS and TBSRTC, but the high ratio of benign cytology
results in categories 4a (54.8%) and 4b (39.5%) demonstrate that
benign characteristics actually dominate these groups and, thus,
the unnecessary biopsy rate is increased, disguising malignancy.
These categories require modifications. Further studies should be
performed concerning inter- and intraobserver variability, internal
and external histological factors, or different imaging methods. A
similar contradiction exists for ES. The E-max values demonstrate a
marginally significant difference between benign and malignant
nodules; however, the significant overlap over a wide range of
values limit its use in daily practice.
We believe that TI-RADS, as well as E-max, may be
considered for inclusion in the 3 main guidelines; however, due to
the abovementioned limitations, they must be simplified/modified.
TBSRTC must have a simple, reproducible US scoring system to
prevent unnecessary FNAs, which may be added to the main guidelines
if it proves to be a secondary success over time.
In conclusion, TI-RADS must be modified, or a new US
uniform reporting system must be created in a significantly more
practical and effective manner. The TI-RADS categories and SE must
be reviewed to eliminate the significant existing overlap between
benign and malignant cytology findings. The high rate of
unnecessary biopsy for benign thyroid nodules is a worldwide
problem; thus, our results demonstrate a certain benefit in
discrimination compared with the current system.
References
|
1
|
Faquin WC, Bongiovanni M and Sadow PM:
Update in thyroid fine needle aspiration. Endocr Pathol.
22:178–183. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
American Thyroid Association (ATA)
Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid
Cancer, . Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL,
Mandel SJ, Mazzaferri EL, McIver B, Pacini F, et al: Revised
American thyroid association management guidelines for patients
with thyroid nodules and differentiated thyroid cancer. Thyroid.
19:1167–1214. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ahn SS, Kim EK, Kang DR, Lim SK, Kwak JY
and Kim MJ: Biopsy of thyroid nodules: Comparison of three sets of
guidelines. AJR Am J Roentgenol. 194:31–37. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cibas ES and Ali SZ: The Bethesda system
for reporting thyroid cytopathology. Thyroid. 19:1159–1165. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Moon HJ, Kim EK, Yoon JH and Kwak JY:
Malignancy risk stratification in thyroid nodules with
nondiagnostic results at cytologic examination: Combination of
thyroid imaging reporting and data system and the Bethesda System.
Radiology. 274:287–295. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dhyani M, Faquin W, Lubitz CC, Daniels GH
and Samir AE: How to interpret thyroid fine-needle aspiration
biopsy reports: A guide for the busy radiologist in the era of the
Bethesda classification system. AJR Am J Roentgenol. 201:1335–1339.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cantisani V, Grazhdani H, Drakonaki E,
D'Andrea V, Di Segni M, Kaleshi E, Calliada F, Catalano C, Redler
A, Brunese L, et al: Strain US elastography for the
characterization of thyroid nodules: Advantages and limitation. Int
J Endocrinol. 2015:9085752015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Horvath E, Majlis S, Rossi R, Franco C,
Niedmann JP, Castro A and Dominguez M: An ultrasonogram reporting
system for thyroid nodules stratifying cancer risk for clinical
management. J Clin Endocrinol Metab. 94:1748–1751. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Park JY, Lee HJ, Jang HW, Kim HK, Yi JH,
Lee W and Kim SH: A proposal for a thyroid imaging reporting and
data system for ultrasound features of thyroid carcinoma. Thyroid.
19:1257–1264. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ophir J, Céspedes I, Ponnekanti H, Yazdi Y
and Li X: Elastography: A quantitative method for imaging the
elasticity of biological tissues. Ultrasoun Imaging. 13:111–134.
1991. View Article : Google Scholar
|
|
11
|
Kwak JY and Kim EK: Ultrasound
elastography for thyroid nodules: Recent advances. Ultrasonography.
33:75–82. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Walfish PG, Miskin M, Rosen IB and
Strawbridge HT: Application of diagnostic techniques in the
management of nodular goiter. Can Med Assoc J. 115:35–40.
1976.PubMed/NCBI
|
|
13
|
Gharib H, Papini E, Paschke R, Duick DS,
Valcavi R, Hegedüs L and Vitti P: AACE/AME/ETA Task Force on
Thyroid Nodules: American Association of Clinical Endocrinologists,
Associazione Medici Endocrinologi and European thyroid association
medical guidelines for clinical practice for the diagnosis and
management of thyroid nodules: Executive summary of
recommendations. J Endocrinol Invest. 33:287–291. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Frates MC, Benson CB, Charboneau JW, Cibas
ES, Clark OH, Coleman BG, Cronan JJ, Doubilet PM, Evans DB,
Goellner JR, et al: Management of thyroid nodules detected at US:
Society of radiologists in ultrasound consensus conference
statement. Ultrasound Q. 22:231–238; discussion 239–240. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kwak JY, Han KH, Yoon JH, Moon HJ, Son EJ,
Park SH, Jung HK, Choi JS, Kim BM and Kim EK: Thyroid imaging
reporting and data system for US features of nodules: A step in
establishing better stratification of cancer risk. Radiology.
260:892–899. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Friedrich-Rust M, Meyer G, Dauth N, Berner
C, Bogdanou D, Herrmann E, Zeuzem S and Bojunga J: Interobserver
agreement of Thyroid Imaging Reporting and Data System (TI-RADS)
and strain elastography for the assessment of thyroid nodules. PLoS
One. 8:e779272013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Eze OP, Cai G, Baloch ZW, Khan A, Virk R,
Hammers LW, Udelsman R, Roman SA, Sosa JA, Carling T, et al:
Vanishing thyroid tumors: A diagnostic dilemma after
ultrasonography-guided fine-needle aspiration. Thyroid. 23:194–200.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Canberk Ş, Firat P and Schmitt F: Pitfalls
in the cytological assessment of thyroid nodules. Turk Patoloji
Derg. 31:(Suppl 1). S18–S33. 2015.
|
|
19
|
Lacout A, Thariat J, Chevenet C and Marcy
PY: Management of thyroid nodules on US with benign or atypical
cytological features. Diagn Interv Imaging. 96:507–509. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Nell S, Kist JW, Debray TP, de Keizer B,
van Oostenbrugge TJ, Borel Rinkes IH, Valk GD and Vriens MR:
Qualitative elastography can replace thyroid nodule fine-needle
aspiration in patients with soft thyroid nodules. A systematic
review and meta-analysis. Eur J Radiol. 84:652–661. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Guazzaroni M, Spinelli A, Coco I, Del
Giudice C, Girardi V and Simonetti G: Value of strain-ratio on
thyroid real-time sonoelastography. Radiol Med. 119:149–155. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Refaat R, Kamel A, Elganzory M and Awad
NM: Can real-time ultrasound elastography using the color score and
strain ratio differentiate between benign and malignant solitary
nodules? The Egyptian Society of Radiology and Nuclear Medicine.
45:75–87. 2014. View Article : Google Scholar
|
|
23
|
Wang H, Zhang S, Xin X, Zhao LH, Li CX, Mu
JL and Wei XQ: Application of real-time ultrasound elastography in
diagnosing benign and malignant thyroid solid nodules. Cancer Biol
Med. 9:124–127. 2012.PubMed/NCBI
|