Introduction
Immunoglobulin (Ig)G4-mediated disease is a systemic
condition, which may manifest as autoimmune pancreatitis type 1 or
extrapancreatic disease, such as biliary lesions, sialadenitis,
retroperitoneal fibrosis, enlarged celiac and hilar lymph nodes,
chronic thyroiditis and interstitial nephritis (1). Less frequently, IgG4-mediated disease
presents solely as sclerosing cholangitis (SC) in the intra- and/or
extrahepatic bile ducts, with high plasma levels of IgG4 and
narrowing of the common bile duct (CBD) on imaging (2). It is challenging to distinguish
IgG4-mediated SC (IgG4-SC) from cholangiocarcinoma, as IgG4-SC may
mimic cholangiocarcinoma clinically and radiologically (2–4). In
addition, carcinomas may be accompanied by significant IgG4
reactions via production of cytokines (5); thus, the presence of IgG4-positive
cells in a bile duct biopsy does not exclude cholangiocarcinoma. We
herein present such a diagnostically challenging case, in which the
patient appeared to have both IgG4-SC and cholangiocarcinoma.
Case report
Our patient was a 43-year-old female without
relevant medical history or use of any medication. The patient
presented with jaundice that was first noticed 4 weeks prior to
presentation. Physical examination revealed icteric sclerae and
skin and a palpable gallbladder without spider naevi, palmar
erythema, enlarged liver or spleen, or pain on palpation. The
initial laboratory testing revealed a total bilirubin level of 122
µmol/l (normal range, 2–20 µmol/l), direct bilirubin of 89 µmol/l
(normal range, 0–5 µmol/l), aspartate aminotransferase 56 U/l
(normal range, 0–31 U/l), alanine aminotransferase 64 U/l (normal
range, 0–34 U/l), alkaline phosphate 491 U/l (normal range, 0–120
U/l) and gamma-glutamyltransferase 132 U/l (normal range, 0–38
U/l). The cancer antigen 19–9 level was not elevated (19 kU/l).
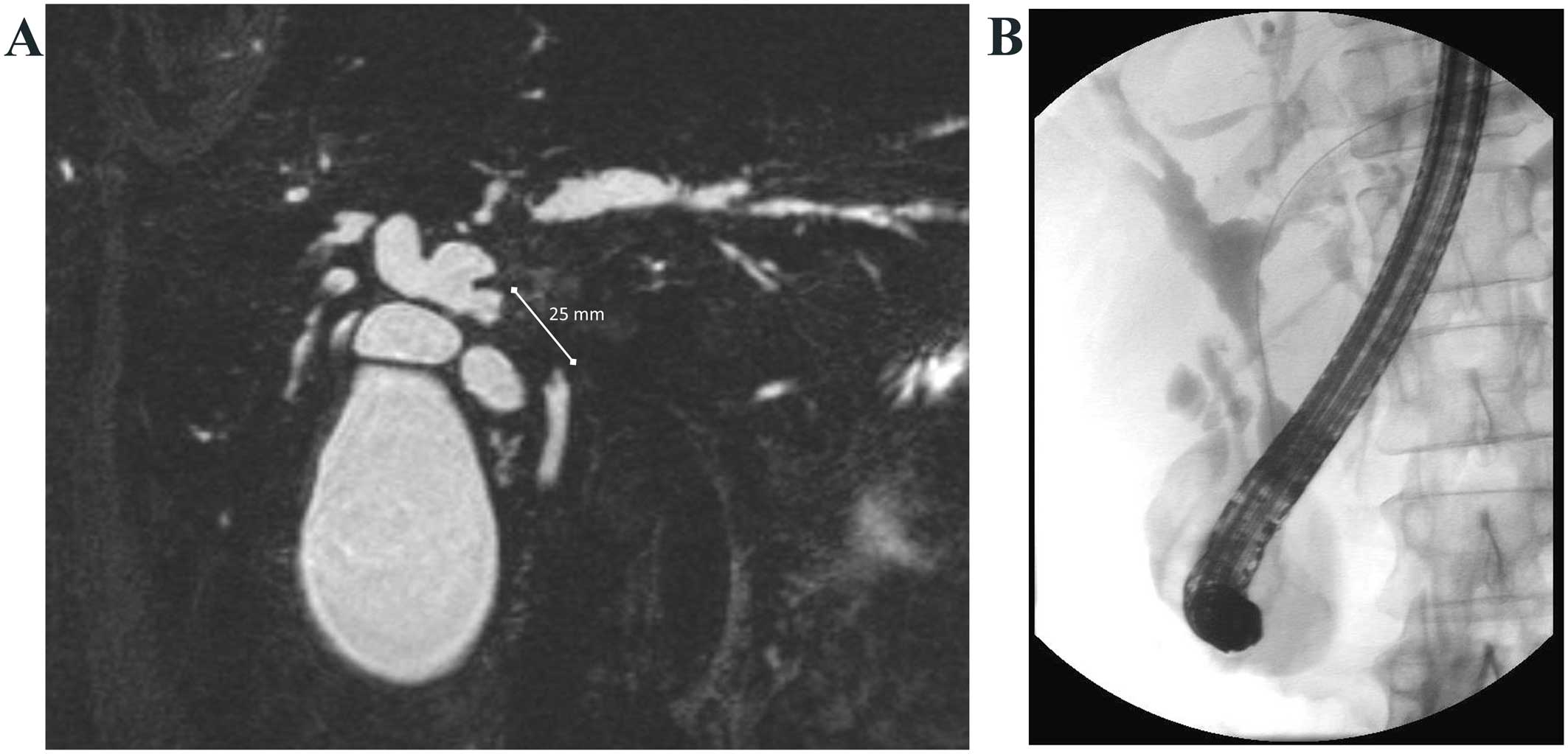
Magnetic resonance cholangiopancreatography revealed dilated
intrahepatic biliary ducts in the left and right hepatic lobes and
intraluminal wall thickening in the proximal CBD over a length of
25 mm, with a ‘shouldering’ margin (Fig.
1), a finding suspicious for cholangiocarcinoma. A computed
tomography (CT) scan indicated a diffusely thickened pancreatic
head, a characteristic that may indicate autoimmune pancreatitis,
and hypodense lesions in hepatic segments 6 and 7.
An endoscopic retrograde cholangiopancreatography
(ERCP) for placement of a CBD endoprosthesis and brush cytology
were performed, after which time cholestasis gradually diminished.
However, brush cytology was inconclusive. Additional laboratory
testing revealed elevated IgG4 levels of 2.92 g/l (normal range,
0.08–1.40 g/l). A treatment for IgG4-associated cholangitis with
prednisone 40 mg/day for 1 month was prescribed, with a repeat ERCP
after the end of treatment. The repeat ERCP revealed a similar
narrowing of the CBD and repeat brush cytology showed malignant
cells, suspicious of adenocarcinoma. As there was no response to
prednisone and malignant cells were found on repeat brush cytology,
IgG4-associated cholangitis became less likely and the patient was
referred for surgical treatment for suspicion of a Bismuth type I
cholangiocarcinoma. To characterize the lesion in hepatic segments
6 and 7 identified on CT scan (i.e., to exclude metastasis) a liver
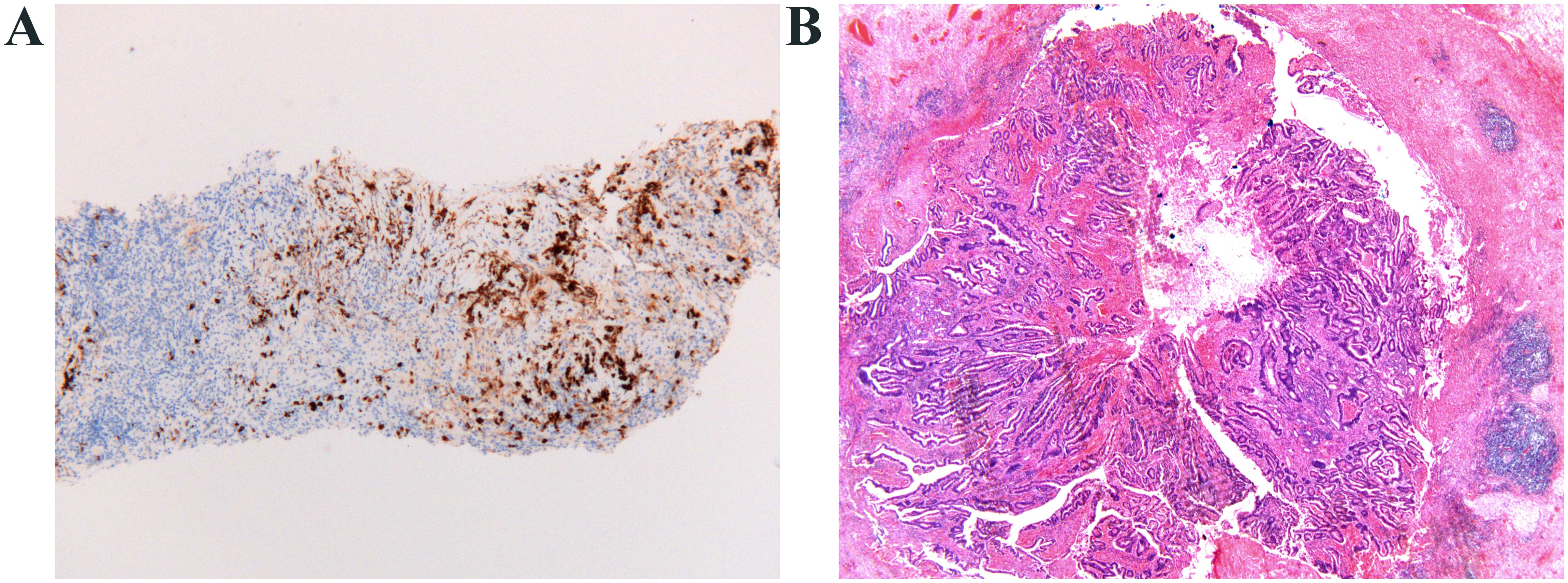
biopsy was performed. Histological analysis revealed a
pericholangiolar inflammation with fibrosis with high
concentrations of IgG4-positive cells (>20 per high-power
field), and obliterative phlebitis, morphologically matching the
diagnosis of IgG4-mediated inflammatory disease. There were no
signs of malignancy (Fig. 2A). A
laparotomy was next performed, with perioperative histopathological
analysis of the CBD stenosis, which revealed a cholangiocarcinoma
and was followed by pancreaticoduodenectomy. Postoperative
histological examination revealed a T1N0M0 cholangiocarcinoma, as
well as IgG4-mediated fibrosis of the CBD (Fig. 2B). The pancreas, duodenum and
gallbladder exhibited no abnormalities. The radiological suspicion
of autoimmune pancreatitis on an earlier CT scan was therefore not
confirmed histologically. The patient was treated with prednisone
and azathioprine for the IgG4-mediated disease and her condition
improved clinically; however, radiologically, the hypodense lesion
in the right hepatic lobe persisted. Repeat biopsy revealed cancer
cells and a right hemihepatectomy was performed. Histological
analysis of the resected specimen showed a tumor with
characteristics identical to the previously diagnosed
cholangiocarcinoma. The postoperative course was uncomplicated, but
plasma IgG4 levels remained elevated. The patient was treated with
prednisone, after which plasma IgG4 levels gradually normalized.
The patient remains in remission, as confirmed by 3-monthly
follow-up CT scans.
Discussion
We herein present a case in which histologically
proven IgG4-mediated disease was present simultaneously with
cholangiocarcinoma. It is known that IgG4-related disease is a
high-risk factor for cancer development (6–11).
Moreover, primary SC, a disease that clinicopathologically
resembles IgG4-SC, is associated with cancer development (12). There is a limited number of case
reports of cholangiocarcinoma coexisting with IgG4-SC (13–15) and
one case report demonstrated the presence of biliary
intraepithelial neoplasia (precursor lesion of bile duct
adenocarcinoma) in the postoperative specimen of a patient with
IgG4-SC (5); however, a causal
association between cholangiocarcinoma and IgG4-SC has not been
proven. In our case, the first liver biopsy provided histological
proof of IgG4-SC without malignancy, whereas on a later biopsy
cancer cells were detected. Similarly, the first endoscopic brush
cytology of the CBD showed no signs of malignancy, whereas a later
brush cytology and the postoperative specimen showed
cholangiocarcinoma. Although a sampling error cannot be excluded in
both cases, the findings indicate that carcinoma may have developed
in an IgG4 lesion. A potential mechanism underlying the
contributing role of IgG4-SC to cholangiocarcinoma development is
via cytokines: An interleukin-10 (IL-10)-related cytokine milieu
initiates the IgG4 reaction and also suppresses tumor-reactive T
cells, suggesting that IgG4-SC may accelerate the development of
cholangiocarcinoma (5). However, the
production mechanism of IgG4 in IgG4-related disease has not been
fully elucidated; another possibility is that mechanisms
contributing to IgG4 production also contribute to carcinogenesis,
rather than IgG4 per se being a causal factor of
carcinogenesis (16). However, the
simultaneous presence of IgG4-SC and cholangiocarcinoma in two
different extrapancreatic lesions in our patient, in addition to
previous reports of IgG4-related disease associated with
malignancy, is a remarkable finding and suggests at least a
pathophysiological association between the two entities.
Extrahepatic cholangiocarcinomas, including
gallbladder cancer, are often accompanied by significant IgG4
reactions. The cholangiocarcinoma cells may function as
non-professional antigen-presenting cells that indirectly induce
IgG4 reactions via the IL-10-producing cells, and/or these may be
FOXP3-positive and IL-10-producing cells that directly induce IgG4
reactions (5). However, there are
several histomorphological characteristics found in IgG4-related SC
that distinguish this condition from malignancy, including a marked
degree of bile duct injury, a higher percentage of lymphoid
follicle formation, a higher percentage of perineuritis, and a more
diffuse and dense lymphoplasmacytic infiltrate (17). These characteristics were present in
the liver biopsy of our patient and, therefore, it is unlikely that
the IgG4 reaction was induced by carcinoma.
In conclusion, we herein report a case in which two
lesions, first characterized as IgG4-SC without signs of
malignancy, were later diagnosed as cholangiocarcinoma. This
phenomenon has been previously reported in IgG4-SC, and
IgG4-related disease in general is closely associated with the
development of malignancies. We therefore suggest that IgG4-SC is a
risk factor for the development of cholangiocarcinoma. This
hypothesis is speculative, since supporting histopathological
evidence is not yet available; however, if confirmed, our
hypothesis has serious clinical implications. Longitudinal
follow-up studies of patients with IgG4-SC, as well as histological
examination of IgG4-SC biopsies for carcinoma precursor lesions,
cytokine expression and lymphocyte subtyping, may strengthen our
hypothesis and it is crucial that such studies are performed in the
near future. Moreover, patients with IgG4-SC must be closely
monitored and when they no longer respond to immunosuppressive
therapy, cholangiocarcinoma should be suspected.
Glossary
Abbreviations
Abbreviations:
|
CBD
|
common bile duct
|
|
ERCP
|
endoscopic retrograde
cholangiopancreaticography
|
|
IgG4
|
immunoglobulin G4
|
|
IgG4-SC
|
immunoglobulin G4-mediated sclerosing
cholangitis
|
|
IL-10
|
interleukin 10
|
References
|
1
|
Detlefsen S: IgG4-related disease: A
systemic condition with characteristic microscopic features. Histol
Histopathol. 28:565–584. 2013.PubMed/NCBI
|
|
2
|
Lin J, Cummings OW, Greenson JK, House MG,
Liu X, Nalbantoglu I, Pai R, Davidson DD and Reuss SA: IgG4-related
sclerosing cholangitis in the absence of autoimmune pancreatitis
mimicking extrahepatic cholangiocarcinoma. Scand J Gastroenterol.
50:447–453. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cheung MT and Lo IL: IgG4-related
sclerosing lymphoplasmacytic pancreatitis and cholangitis mimicking
carcinoma of pancreas and Klatskin tumour. ANZ J Surg. 78:252–256.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Miki A, Sakuma Y, Ohzawa H, Sanada Y,
Sasanuma H, Lefor AT, Sata N and Yasuda Y: Immunoglobulin
G4-related sclerosing cholangitis mimicking hilar
cholangiocarcinoma diagnosed with following bile duct resection:
Report of a case. Int Surg. 100:480–485. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Harada K and Nakanuma Y:
Cholangiocarcinoma with respect to IgG4 Reaction. Int J Hepatol.
2014:8038762014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fukui T, Mitsuyama T, Takaoka M, Uchida K,
Matsushita M and Okazaki K: Pancreatic cancer associated with
autoimmune pancreatitis in remission. Intern Med. 47:151–155. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ghazale A and Chari S: Is autoimmune
pancreatitis a risk factor for pancreatic cancer? Pancreas.
35:3762007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Inoue H, Miyatani H, Sawada Y and Yoshida
Y: A case of pancreas cancer with autoimmune pancreatitis.
Pancreas. 33:208–209. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Loos M, Esposito I, Hedderich DM, Ludwig
L, Fingerle A, Friess H, Klöppel G and Büchler P: Autoimmune
pancreatitis complicated by carcinoma of the pancreatobiliary
system: A case report and review of the literature. Pancreas.
40:151–154. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pezzilli R, Vecchiarelli S, Di Marco MC,
Serra C, Santini D, Calculli L, Fabbri D, Mena B Rojas and Imbrogno
A: Pancreatic ductal adenocarcinoma associated with autoimmune
pancreatitis. Case Rep Gastroenterol. 5:378–385. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Huggett MT, Culver EL, Kumar M, Hurst JM,
Rodriguez-Justo M, Chapman MH, Johnson GJ, Pereira SP, Chapman RW,
Webster GJ and Barnes E: Type 1 autoimmune pancreatitis and
IgG4-related sclerosing cholangitis is associated with
extrapancreatic organ failure, malignancy, and mortality in a
prospective UK cohort. Am J Gastroenterol. 109:1675–1683. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mendes F and Lindor KD: Primary sclerosing
cholangitis: Overview and update. Nat Rev Gastroenterol Hepatol.
7:611–619. 2010.PubMed/NCBI
|
|
13
|
Douhara A, Mitoro A, Otani E, Furukawa M,
Kaji K, Uejima M, Sawai M, Yoshida M, Yoshiji H, Yamao J and Fukui
H: Cholangiocarcinoma developed in a patient with IgG4-related
disease. World J Gastrointest Oncol. 5:181–185. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Oh HC, Kim JG, Kim JW, Lee KS, Kim MK, Chi
KC, Kim YS and Kim KH: Early bile duct cancer in a background of
sclerosing cholangitis and autoimmune pancreatitis. Intern Med.
47:2025–2028. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Straub BK, Esposito I, Gotthardt D,
Radeleff B, Antolovic D, Flechtenmacher C and Schirmacher P:
IgG4-associated cholangitis with cholangiocarcinoma. Virchows Arch.
458:761–765. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kusuda T, Uchida K, Miyoshi H, Koyabu M,
Satoi S, Takaoka M, Shikata N, Uemura Y and Okazaki K: Involvement
of inducible costimulator- and interleukin 10-positive regulatory T
cells in the development of IgG4-related autoimmune pancreatitis.
Pancreas. 40:1120–1130. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Deshpande V, Zen Y, Chan JK, Yi EE, Sato
Y, Yoshino T, Klöppel G, Heathcote JG, Khosroshahi A, Ferry JA, et
al: Consensus statement on the pathology of IgG4-related disease.
Mod Pathol. 25:1181–1192. 2012. View Article : Google Scholar : PubMed/NCBI
|