Introduction
Cancer of the gastrointestinal system are a leading
cause of mortality worldwide and are more prevalent compared with
breast cancer and brain tumors. In Japan, cancer of seven
gastrointestinal system sites, including the esophagus, stomach,
colorectum, liver and pancreas, are listed among the top 10 causes
of cancer-associated mortality. Colorectal cancer (CRC) is the
fourth leading cause of mortality worldwide, and there are 1.2
million novel CRC cases and ~608,000 mortalities occurred in 2008
(1). In 2012, an estimated 1.4
million novel CRC cases and 693,900 mortalities, and the incidence
rates are increasing in numerous countries (2–4). Despite
rising incidence of CRC, mortality rates of CRC are decreasing
worldwide, likely due to screening and improved treatment (5,6). In CRC,
prognosis of patients have been drastically improving, particularly
with the combination of chemotherapeutic agents and development of
molecular target drugs, including anti-epidermal growth factor
receptor (EGFR) antibody, anti-vascular endothelial growth factor
(VEGF) antibody and multikinase inhibitor (7–11). In
previous years, screenings of cancer-associated molecules have been
eagerly performed to identify the novel molecular targets and
development of novel anticancer agents.
The present study focused on the expression of
ADAMTS5 in colorectal cancer. ADAMTS family members contain
thrombospondin motifs, cysteine-rich and spacer domains in addition
to propeptide, metalloproteinase and disintegrin domains (12). The matrix metalloproteinases (MMPs)
serve key roles for cancer cell proliferation, progression and
metastasis in numerous human cancer types via their activity of
degradation of the extracellular matrix (13). Although overexpression of ADAMTS5 has
been reported in glioblastoma (14–16), and
head and neck cancer (17), the
expression and the roles of ADAMTS5 remain to be understood in
colorectal cancer types. The present study measured the expression
of ADAMTS5, and clarified the roles of ADAMTS5 by the assessment of
mRNA expression and clinicopathological factors in colorectal
cancer.
Materials and methods
Patients and specimens
Specimens of primary colorectal cancer samples were
obtained from 143 patients with colorectal cancer who underwent
surgery between March 2003 and June 2006. All of the specimens were
obtained with approval with informed consent from the patients, and
were stored with anonymized clinicopathological data at Osaka
University (Osaka, Japan). Retrospective analysis using stored
tumor specimens was performed under the acceptance of the Research
Ethics Board of Osaka University. The present study utilized cDNAs
of colorectal cancer specimens to evaluate the expression of
ADAMTS5.
Semi-quantitative polymerase chain
reaction (PCR)
Using stored cDNAs from colorectal cancer specimens,
the present study evaluated the expression of ADAMTS5. The PCR was
performed using the Light Cycler (Roche Diagnostics Deutschland
GmbH, Mannheim, Germany). The primers used were as follows:
ADAMTS5, forward: 5′-GCTACTGCACAGGGAAGAGG-3′ and reverse:
5′-TGCATATTTGGGAACCCATT-3′; GAPDH (internal control), forward
5′-CAACTACATGGTTTACATGTTC-3′ and reverse: 5′-GCCAGTGGACTCCACGAC-3′.
The amplification protocol consisted of 55 cycles of denaturation
at 95°C for 5 sec, annealing at 60°C for 5 sec and extension at
72°C for 30 sec.
Definition of tumor stage
Tumor stages were defined according to the
tumor-node-metastasis (TNM) Classification of Malignant Tumours 7th
Edition [Union Internationale Contre le Cancer (UICC)].
Statistical analysis
The present study divided cases for analysis based
on the expression of ADAMTS5 (Low or High). The median score of
ADAMTS5 expression was used to define the higher ADAMTS5 expression
group (High group) and the lower expression group (Low group).
Fisher's exact test was used to compare the differences between the
ADAMTS5 High and Low groups. The present study assessed the overall
survival (OS) and disease-free survival (DFS) of these two groups
using the Kaplan-Meier method. The log-rank test calculates the
significance of any differences. Cases of non-curative resection
were excluded in the DFS analyses. Univariate and multivariate
analyses for OS or DFS were performed to evaluate the independent
prognostic factors using Cox proportional hazards model. All
statistic analyses were performed using JMP 11.0.0 software (SAS
Institute, Cary, NC, USA). P<0.05 was considered to indicate a
statistically significant difference.
Results
Expression of ADAMTS5 in colorectal
cancer
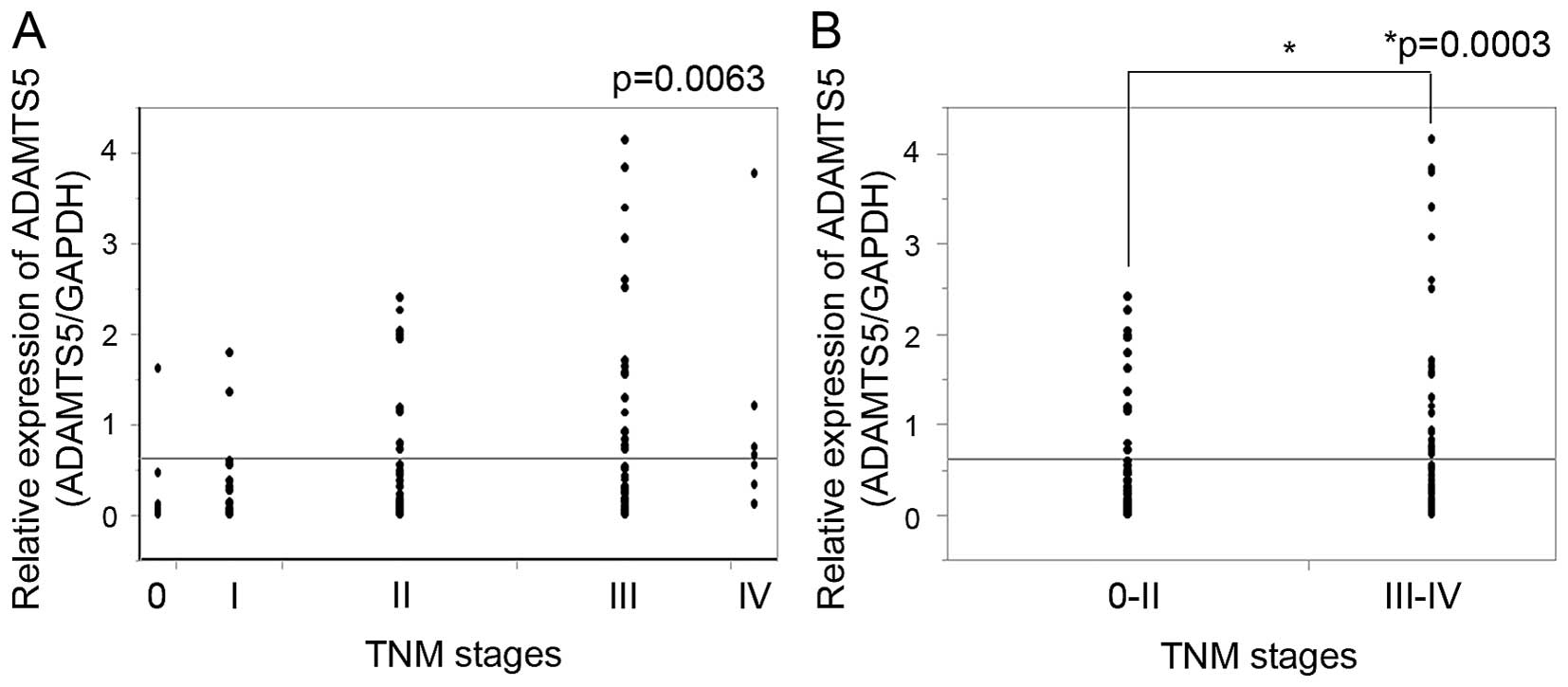
Expression of ADAMTS5 was assessed in the 143
colorectal cancer specimens. ADAMTS5 expression was relatively low;
however, was identified in all of the 143 specimens. The expression
of ADAMTS5 was increased as the TNM stage increased (P=0.0063;
Fig. 1A). When TNM stage was divided
into the two groups, stage 0-II and stage III–IV, expression of
ADAMTS5 was significantly higher in the TNM stage III–IV compared
with the TNM stage 0-II (P=0.0003; Fig.
1B).
Expression of ADAMTS5 and
clinicopathological factors
To assess the association between the expression of
ADAMTS5 and clinicopathological factors and prognosis, the present
study divided patients based on the median score of ADAMTS5
expression into two groups: ADAMTS5 high and low expression groups.
The ADAMTS5 low group included 72 patients and the ADAMTS5 high
group included 71 patients (P=0.1533). The ADAMTS5 low group
included 52 males and 19 females, and the ADAMTS5 high group
involved 43 males and 28 females. No significant differences in the
histological type (P=1.000), venous invasion (P=0.7348) and depth
of tumor invasion (P=0.4205) was observed between the ADAMTS5 low
group and the ADAMTS5 high group (Table
I). In the analysis of clinicopathological factors, the
proportions of lymphatic invasion (P=0.0214) and lymph node
metastasis (P=0.0289) were significantly greater in the ADAMTS5
high group compared with the ADAMTS5 low group. Although the TNM
stage was potentially greater in the ADAMTS5 high group compared
with the ADAMTS5 low group (P=0.0896), the proportion of the
distant metastasis was not significantly different between these
two groups (P=0.1675).
 | Table I.Baseline characteristics of
clinicopathological factors. |
Table I.
Baseline characteristics of
clinicopathological factors.
|
| ADAMTS5 |
|
|---|
|
|
|
|
|---|
| Characteristic | Low group (n=72) | High group
(n=71) | P-value |
|---|
| Gender |
|
| 0.1533 |
| Male, n
(%) | 52 (73.24) | 43 (60.56) |
|
| Female, n
(%) | 19 (26.76) | 28 (39.44) |
|
| Histologic type |
|
| 1.000 |
|
tub1-tub2, n (%) | 69 (95.83) | 68 (95.77) |
|
| por-sig,
n (%) | 3 (4.17) | 3 (4.23) |
|
| Lymphatic
invasion |
|
| 0.0214 |
| Positive,
n (%) | 47 (65.28) | 59 (83.10) |
|
| Negative,
n (%) | 25 (34.72) | 12 (16.90) |
|
| Venous invasion |
|
| 0.7348 |
| Positive,
n (%) | 41 (56.94) | 43 (60.56) |
|
| Negative,
n (%) | 31 (43.06) | 28 (39.44) |
|
| Depth of tumor
invasion |
|
| 0.4205 |
|
T0/T1/T2 | 6/5/7 | 2/1/10 |
|
| T3 | 25 | 28 |
|
| T4a | 22 | 25 |
|
| T4b | 7 | 3 |
|
|
T0-2/T3-4 | 18/54 | 13/56 |
|
| Lymph node
metastasis |
|
| 0.0289 |
| Positive,
n (%) | 25 (34.72) | 38 (53.52) |
|
| Negative,
n (%) | 47 (65.28) | 33 (46.48) |
|
| UICC stage |
|
| 0.0896 |
|
0/I/II/III/IV | 5/12/29/17/9 | 2/9/18/27/15 |
|
| Distant
metastasis |
|
| 0.1675 |
|
Positive | 9 | 15 |
|
|
Negative | 63 | 56 |
|
Expression of ADAMTS5 and clinical
outcome
Correlation of the expression of ADAMTS5 with
clinical outcome was assessed by the comparison of the ADAMTS5 high
group and the ADAMTS5 low group. Univariate and multivariate
analyses indicated that lymphatic invasion, venous invasion and
lymph node metastasis were independent prognostic factors for OS
(Table II). The expression of
ADAMTS5 was not characterized as an independent prognostic factor
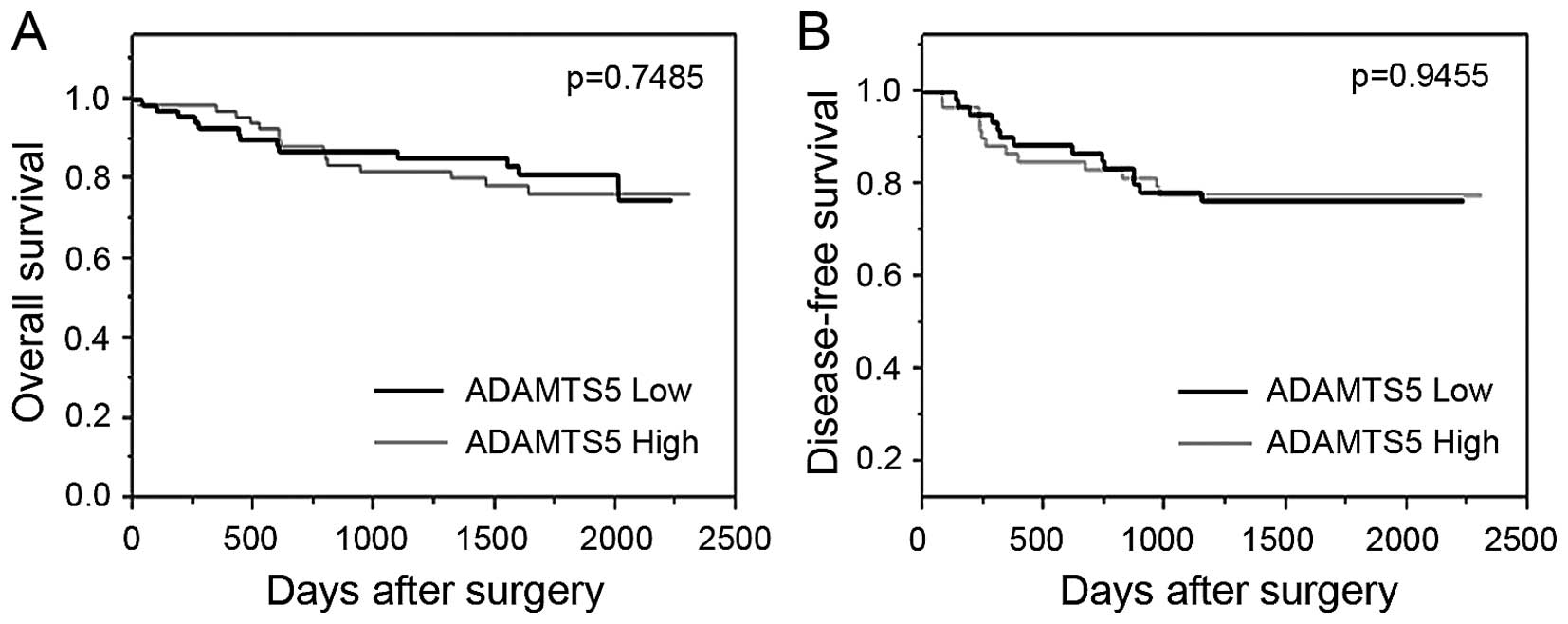
for OS (P=0.7490). The OS and DFS were assessed by the Kaplan-Meier
method, using the log-rank test. The Kaplan-Meier curves revealed
no significant differences in the OS between the ADAMTS5 low group
and the ADAMTS5 high group (P=0.7485; Fig. 2A).
| Table II.Univariate and multivariate analysis
associated with overall survival. |
Table II.
Univariate and multivariate analysis
associated with overall survival.
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|---|
| Characteristic | n | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Gender
(male/female) | 95/47 | 1.1 | 0.516–2.542 | 0.8101 | – | – | – |
| ADAMTS5 expression
(high/low) | 71/72 | 0.887 | 0.422–1.852 | 0.749 | – | – | – |
| Pathological type
(por-sig/tub1-2) | 6/137 | 5.301 | 1.252–15.34 | 0.0273 | 1.79 | 0.418–5.314 | 0.3851 |
| Lymphatic invasion
(+/−) | 106/37 | – | – | 0.0001 | – | – | 0.0158 |
| Venous invasion
(+/−) | 84/59 | 10.97 | 3.290–68.04 | 0.0001 | 5.996 | 1.770–37.40 | 0.0019 |
| pT (T3-4/T0-2) | 110/31 | 9.084 | 1.939–161.9 | 0.0017 | 2.895 | 0.592–52.31 | 0.2262 |
| pN (+/−) | 63/80 | 6.371 | 2.750–17.31 | 0.0001 | 2.548 | 1.066–7.089 | 0.0347 |
Next, the present study assessed the correlation
between ADAMTS5 expression and DFS in the 125 patients; 18 patients
from the 143 patients were excluded from this analysis due to
non-curative surgery. Adjuvant chemotherapy was performed on the 16
patients (25.4%) of the ADAMTS5 low group and on the 24 patients
(38.71%) of the ADAMTS5 high group. Relapse was observed in the 27
patients; 4 patients (22.2%) in the ADAMTS5 low group and 13
patients (21.0%) in the ADAMTS5 high group, respectively. No
significant correlation was observed between the expression of
ADAMTS5 and the proportion of recurrence (Table III; P=1.000). No significant
correlation was observed between ADAMTS5 expression and DFS, based
on the Kaplan-Meier curve with log-rank test (P=0.9455; Fig. 2B). Univariate analyses revealed no
significance of the ADAMTS5 expression on DFS (hazard risk=1.026;
95% confidence interval=0.4799–2.211; P=0.9455).
| Table III.Expression of ADMATS5 and
recurrence. |
Table III.
Expression of ADMATS5 and
recurrence.
|
| ADAMTS5 |
|
|---|
|
|
|
|
|---|
| Characteristic | Low group
(n=63) | High group
(n=62) | P-value |
|---|
| Adjuvant
chemotherapy |
|
| 0.1277 |
|
Yes | 16 (25.40%) | 24 (38.71%) |
|
| No | 47 (74.60%) | 38 (61.29%) |
|
| Recurrence |
|
| 1.000 |
|
Yes | 14 (22.22%) | 13 (20.97%) |
|
| No | 49 (77.78%) | 49 (79.03%) |
|
Discussion
ADAMTS5, also termed aggrecanase-2 due to aggrecan-
degrading activity, is a member of the ADAM superfamily (18,19). The
proteoglycanase activity of ADAMTS5, known as an member of
extracellular matrix (ECM) degrading enzymes, shows proteolytic
activity toward the hyalectan group of chondroitin sulphate
proteoglycans (CSPGs), which comprise aggrecan, versican, brevican
and neurocan (20). Although ADAMTS5
have been implicated in various cellular events, including cleavage
of proteoglycans, ECM degradation, inhibition of angiogenesis and
embryonic morphogenesis (21), their
roles in cancer remain to be established. Upregulated expression of
ADAMTS5 has been reported in proliferating glioblastoma cells
(14), and ADAMTS5 cleaves brevican
and serves an important role in glioma cell invasion (15). In head and neck cancer, mRNA
expression of ADAMTS5 has been reported to overexpress in
metastatic foci (17). By contrast,
downregulation of ADAMTS5 expression has been reported in prostate
cancer and TGF-β exposed prostatic stromal cells (22). In a previous study of the breast,
while ADAMTS5 was expressed predominantly in myoepithelial cells,
ADAMTS5 gene expression was downregulated in cancer tissues
(23). In the present study, ADAMTS5
expression in colorectal cancer was significantly correlated with
the lymphatic invasion and lymph node metastasis. Expression of
ADAMTS5 increased according to TNM stage; stage III–IV colorectal
cancer specimens expressed higher level of ADAMTS5 compared with
stage 0-II. Considering that lymph node metastasis status divides
stage III from stage 0-II, and that ADAMTS5 expression increase
markedly in stage III, ADAMTS5 expression is potentially available
as a marker of lymph node metastasis in colorectal cancer.
The present study failed to identify ADAMTS5 as an
independent prognostic factor of colorectal cancer. Univariate
analysis and the Kaplan-Meier curves revealed no significant impact
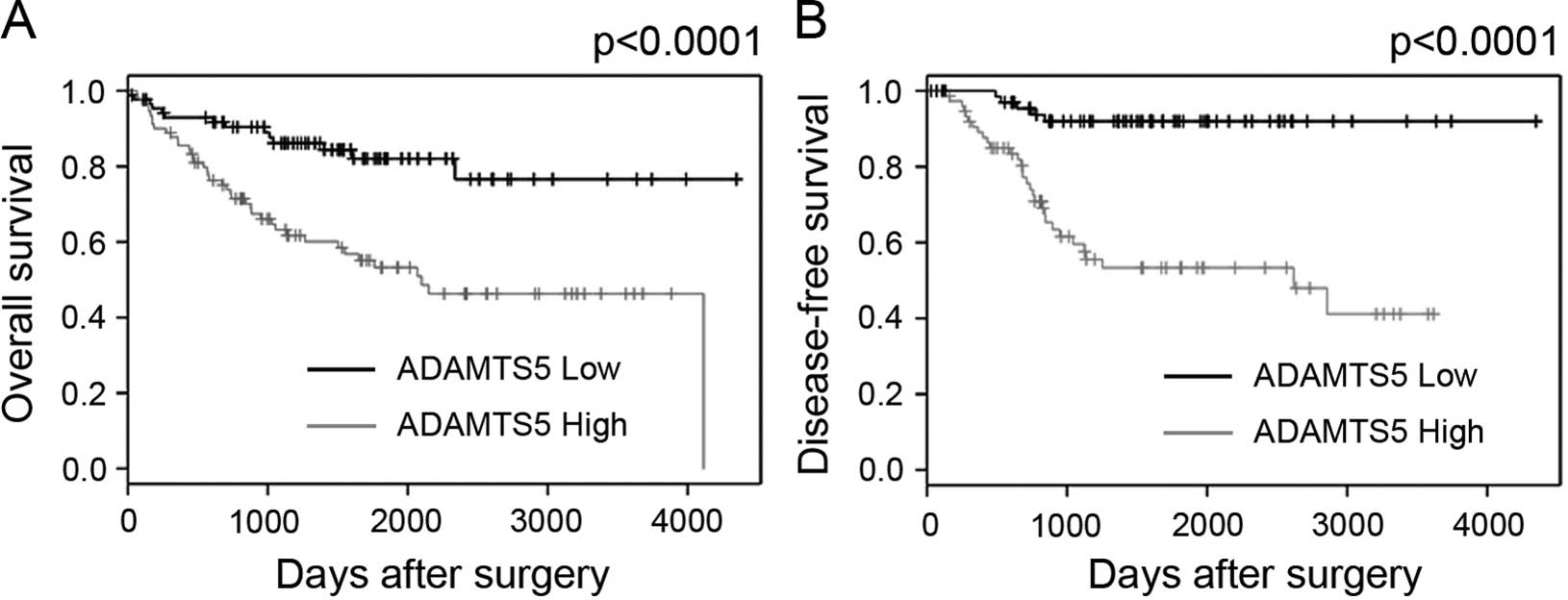
of ADAMTS5 as a prognostic factor. To confirm these results,
microarray data of colorectal cancer specimens listed on PrognoScan
(http://www.abren.net/PrognoScan/) were
used (24). The microarray data sets
(http://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE17536)
used in the previous report of gene expression profile analysis
(25) was used for analysis. The
median value of intensity of microarray probes of ADAMTS5 was used
for the ADAMTS5 low expressing group and the ADAMTS5 high
expressing group. OS and DSF of the ADAMTS5 high expressing
patients were significantly poorer compared with those of the
ADAMTS5 low expressing patients (P<0.0001 in OS and DSF)
(Fig. 3). Although the factor that
causes such large differences cannot be fully clarified, difference
of sequence between microarray probe and PCR probe can be listed as
one of the reasons. Difference of post-operative treatment and/or
difference of concept of lymphadenectomy may potentially affect
these differences. Expression and roles of ADAMTS5 remain to be
determined in colorectal cancer (26). Further studies, including molecular
based analysis and protein analysis, are required.
Acknowledgements
The authors would like to thank Ms. Yurika Nakamura
at Departments of Gastroenterological Surgery, Graduate School of
Medicine, Osaka University for excellent technical assistance.
References
|
1
|
Ferlay J, Shin HR, Bray F, Forman D,
Mathers C and Parkin DM: Estimates of worldwide burden of cancer in
2008: GLOBOCAN 2008. Int J Cancer. 127:2893–2917. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Torre LA, Siegel RL, Ward EM and Jemal A:
Global cancer incidence and mortality rates and trends-an update.
Cancer Epidemiol Biomarkers Prev. 25:16–27. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bray F: The evolving scale and profile of
cancer worldwide: Much ado about everything. Cancer Epidemiol
Biomarkers Prev. 25:3–5. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cunningham D, Atkin W, Lenz HJ, Lynch HT,
Minsky B, Nordlinger B and Starling N: Colorectal cancer. Lancet.
375:1030–1047. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bosetti C, Levi F, Rosato V, Bertuccio P,
Lucchini F, Negri E and La Vecchia C: Recent trends in colorectal
cancer mortality in Europe. Int J Cancer. 129:180–191. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Edwards BK, Ward E, Kohler BA, Eheman C,
Zauber AG, Anderson RN, Jemal A, Schymura MJ, Lansdorp-Vogelaar I,
Seeff LC, et al: Annual report to the nation on the status of
cancer, 1975–2006, featuring colorectal cancer trends and impact of
interventions (risk factors, screening, and treatment) to reduce
future rates. Cancer. 116:544–573. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Jonker DJ, O'Callaghan CJ, Karapetis CS,
Zalcberg JR, Tu D, Au HJ, Berry SR, Krahn M, Price T, Simes RJ, et
al: Cetuximab for the treatment of colorectal cancer. N Engl J Med.
357:2040–2048. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Karapetis CS, Khambata-Ford S, Jonker DJ,
O'Callaghan CJ, Tu D, Tebbutt NC, Simes RJ, Chalchal H, Shapiro JD,
Robitaille S, et al: K-ras mutations and benefit from cetuximab in
advanced colorectal cancer. N Engl J Med. 359:1757–1765. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Van Cutsem E, Peeters M, Siena S, Humblet
Y, Hendlisz A, Neyns B, Canon JL, Van Laethem JL, Maurel J,
Richardson G, et al: Open-label phase III trial of panitumumab plus
best supportive care compared with best supportive care alone in
patients with chemotherapy-refractory metastatic colorectal cancer.
J Clin Oncol. 25:1658–1664. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hurwitz H, Fehrenbacher L, Novotny W,
Cartwright T, Hainsworth J, Heim W, Berlin J, Baron A, Griffing S,
Holmgren E, et al: Bevacizumab plus irinotecan, fluorouracil, and
leucovorin for metastatic colorectal cancer. N Engl J Med.
350:2335–2342. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Grothey A, Van Cutsem E, Sobrero A, Siena
S, Falcone A, Ychou M, Humblet Y, Bouché O, Mineur L, Barone C, et
al: Regorafenib monotherapy for previously treated metastatic
colorectal cancer (CORRECT): An international, multicentre,
randomised, placebo-controlled, phase 3 trial. Lancet. 381:303–312.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mochizuki S and Okada Y: ADAMs in cancer
cell proliferation and progression. Cancer Sci. 98:621–628. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Egeblad M and Werb Z: New functions for
the matrix metalloproteinases in cancer progression. Nat Rev
Cancer. 2:161–174. 2002. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Held-Feindt J, Paredes EB, Blömer U,
Seidenbecher C, Stark AM, Mehdorn HM and Mentlein R:
Matrix-degrading proteases ADAMTS4 and ADAMTS5 (disintegrins and
metalloproteinases with thrombospondin motifs 4 and 5) are
expressed in human glioblastomas. Int J Cancer. 118:55–61. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Nakada M, Miyamori H, Kita D, Takahashi T,
Yamashita J, Sato H, Miura R, Yamaguchi Y and Okada Y: Human
glioblastomas overexpress ADAMTS-5 that degrades brevican. Acta
Neuropathol. 110:239–246. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Viapiano MS, Hockfield S and Matthews RT:
BEHAB/brevican requires ADAMTS-mediated proteolytic cleavage to
promote glioma invasion. J Neurooncol. 88:261–272. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Demircan K, Gunduz E, Gunduz M, Beder LB,
Hirohata S, Nagatsuka H, Cengiz B, Cilek MZ, Yamanaka N, Shimizu K
and Ninomiya Y: Increased mRNA expression of ADAMTS
metalloproteinases in metastatic foci of head and neck cancer. Head
Neck. 31:793–801. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hurskainen TL, Hirohata S, Seldin MF and
Apte SS: ADAM-TS5, ADAM-TS6 and ADAM-TS7, novel members of a new
family of zinc metalloproteases. General features and genomic
distribution of the ADAM-TS family. J Biol Chem. 274:25555–25563.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Apte SS: A disintegrin-like and
metalloprotease (reprolysin-type) with thrombospondin type 1 motif
(ADAMTS) superfamily: Functions and mechanisms. J Biol Chem.
284:31493–31497. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Schaefer L and Schaefer RM: Proteoglycans:
From structural compounds to signaling molecules. Cell Tissue Res.
339:237–246. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kintakas C and McCulloch DR: Emerging
roles for ADAMTS5 during development and disease. Matrix Biol.
30:311–317. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Cross NA, Chandrasekharan S, Jokonya N,
Fowles A, Hamdy FC, Buttle DJ and Eaton CL: The expression and
regulation of ADAMTS-1, −4, −5, −9 and −15 and TIMP-3 by TGFbeta1
in prostate cells: Relevance to the accumulation of versican.
Prostate. 63:269–275. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Porter S, Scott SD, Sassoon EM, Williams
MR, Jones JL, Girling AC, Ball RY and Edwards DR: Dysregulated
expression of adamalysin-thrombospondin genes in human breast
carcinoma. Clin Cancer Res. 10:2429–2440. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Mizuno H, Kitada K, Nakai K and Sarai A:
PrognoScan: A new database for meta-analysis of the prognostic
value of genes. BMC Med Genomics. 2:182009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Smith JJ, Deane NG, Wu F, Merchant NB,
Zhang B, Jiang A, Lu P, Johnson JC, Schmidt C, Bailey CE, et al:
Experimentally derived metastasis gene expression profile predicts
recurrence and death in patients with colon cancer.
Gastroenterology. 138:958–968. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kim YH, Lee HC, Kim SY, Yeom YI, Ryu KJ,
Min BH, Kim DH, Son HJ, Rhee PL, Kim JJ, et al: Epigenomic analysis
of aberrantly methylated genes in colorectal cancer identifies
genes commonly affected by epigenetic alterations. Ann Surg Oncol.
18:2338–2347. 2011. View Article : Google Scholar : PubMed/NCBI
|