Introduction
A chronic expanding hematoma of the chest is a rare
condition that often occurs months to years after tuberculous
pleuritis or thoracic surgery, and rarely after a blunt chest
trauma (1–3). Chest injury due to blunt chest trauma
may result in a hemorrhage or an acute intrathoracic hematoma,
which is often naturally reabsorbed and rarely causes serious
problems. Under rare conditions, however, the mass slowly grows and
enlarges inside the chest. Surgical removal is the main treatment
for thoracic hematomas. However, complete resection is not easily
achieved, mainly due to the presence of dense fibrous adhesions to
adjacent tissues. we herein report the case of a patient with a
huge chronic expanding hematoma in the chest, which had grown over
a 25-year period following a blunt chest trauma. The patient was
successfully treated by surgical resection.
Case report
A 42-year-old man with a dull pain in the chest was
admitted to the Sichuan Cancer Hospital (Chengdu, China). Apart
from chest pain, no other symptoms or signs were found. The patient
denied any history of thoracic surgery or pulmonary diseases,
including tuberculosis, but recalled an incident of blunt chest
trauma. The patient was injured in the chest during a fight 25
years ago, but he did not seek medical help at that time. Chest
X-ray revealed a huge mass shadow in the anterior mediastinum.
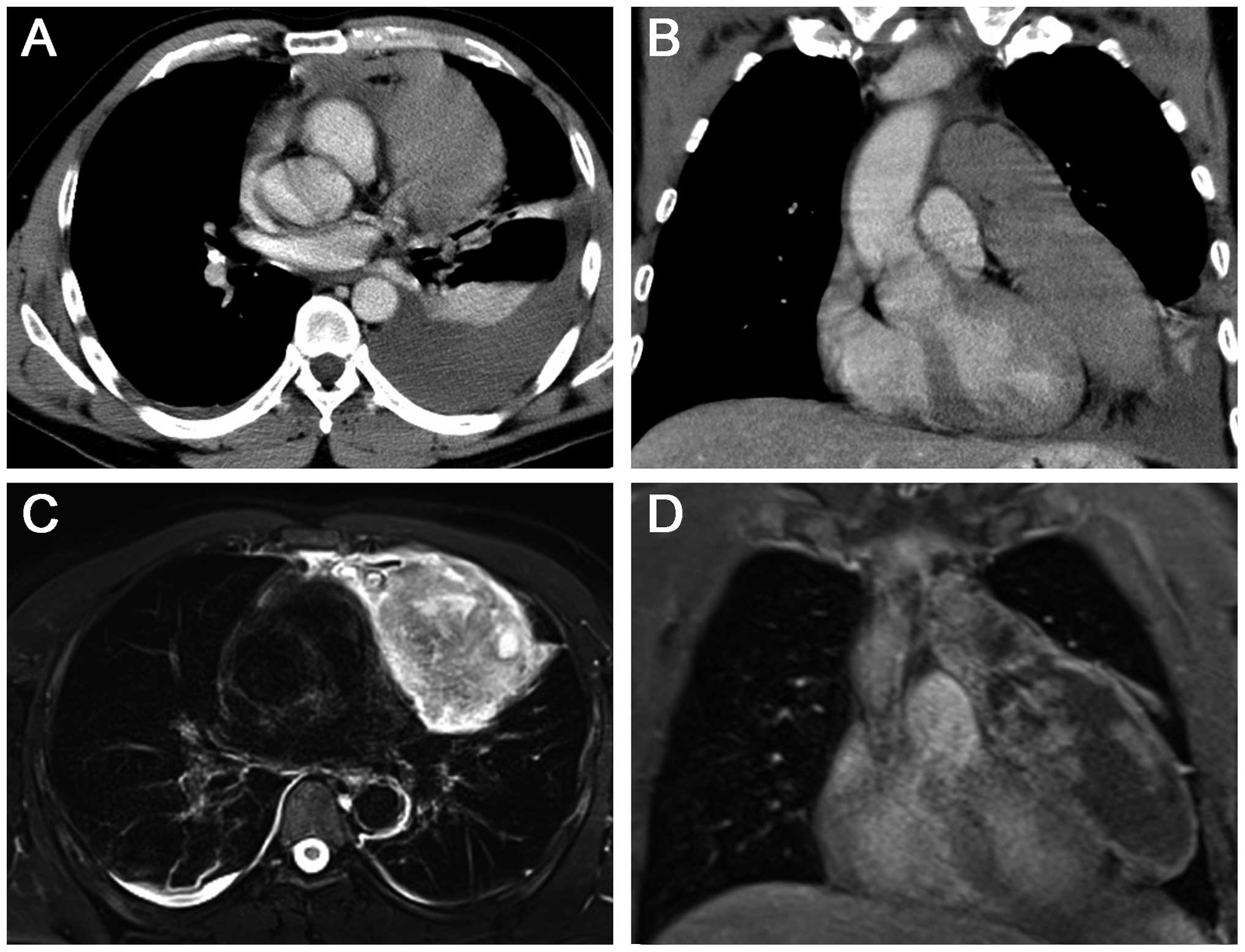
Chest computed tomography (CT) revealed an intrathoracic mass sized
10.2×13.3×17.9 cm, without calcification, which tightly adhered to
the left pericardium. A left moderate pleural effusion was also
detected on CT imaging (Fig. 1A and
B). T2-weighted magnetic resonance imaging (MRI) revealed a
variety of signal intensities in the mass, appearing as a mosaic
pattern (Fig. 1C). Diagnostic
thoracocentesis was performed to determine the characteristics of
the left pleural effusion, and only erythrocytes and a few
inflammatory cells were detected by cytological examination.
Subsequently, a CT-guided needle biopsy was performed, but the
results were negative.
The mass was then considered to be a benign or
low-to-moderate malignant tumor, such as a teratoma, or chronic
empyema. Most of the lesion was located in the left thorax and
complete resection of the lesion appeared to be feasible, based on
the preoperative imaging evaluation. Therefore, a left
posterolateral thoracotomy through the 5th intercostal space was
performed. There were no pleural adhesions. The mass was located in
the left anterior mediastinum and had a thickened, hard capsule,
which was loosely attached to the diaphragm, but was tightly
adherent to the thymus, pericardium and upper lobe of the left
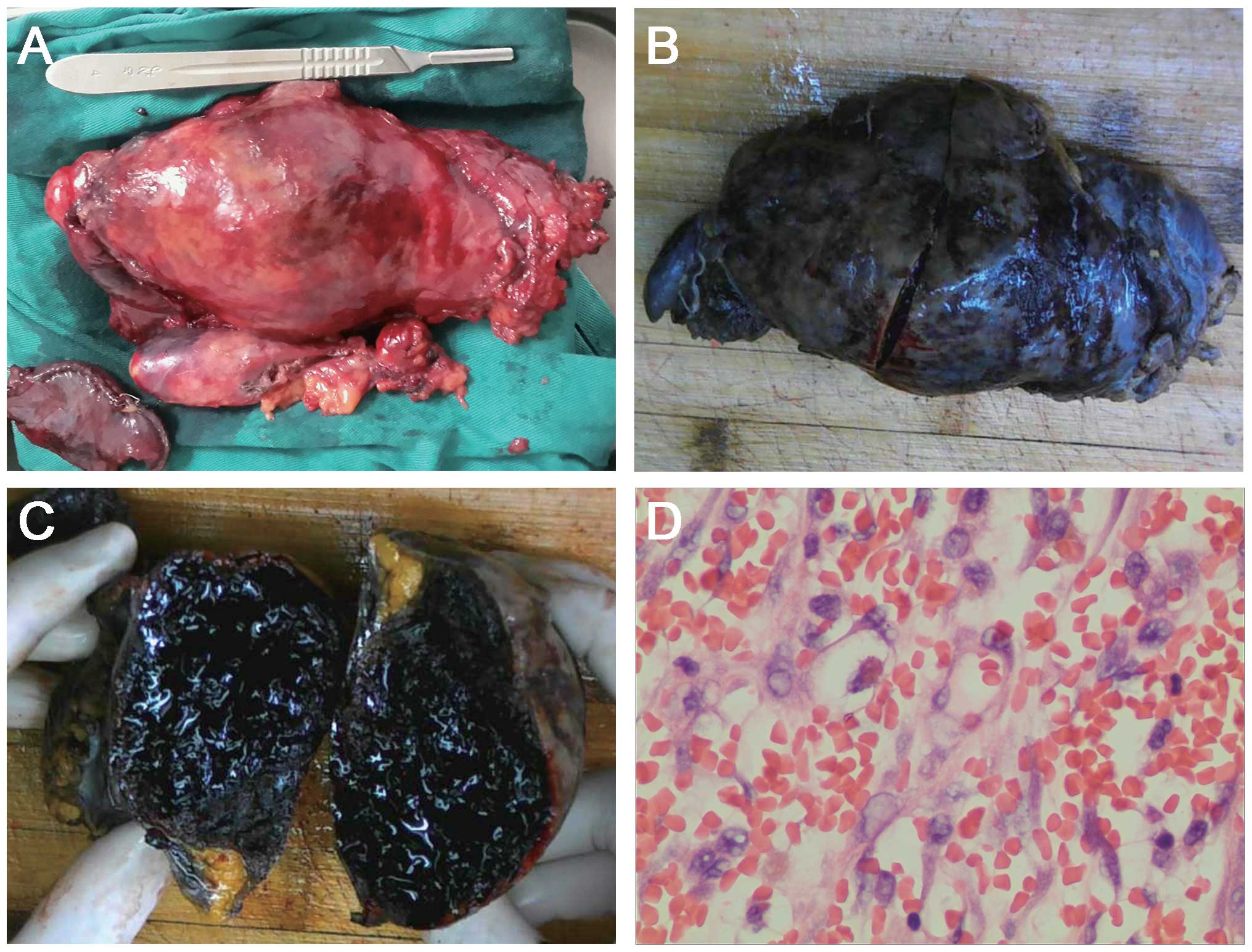
lung. The mass was completely removed, with most of the thymus and
left parietal pericardium, and part of the upper lobe of the left
lung (Fig. 2A). The operative time
was 140 min and the total intraoperative blood loss was 250 ml.
On macroscopic examination, the resected mass was
surrounded by a dense fibrous capsule, filled with hemorrhagic
material and necrotic tissue (Fig.
2A–C), which was further confirmed by histopathological
analysis (Fig. 2D). There was no
evidence of malignancy or infection within the mass. Finally, the
patient was diagnosed with a chronic expanding hematoma. The
postoperative course was uneventful. There was no sign of
recurrence during the 6 months of follow-up.
Discussion
A chronic expanding hematoma was first described by
Reid et al as a rare clinicopathological entity,
characterized by its persistence and increasing size after the
initial hemorrhage (4). chronic
expanding hematoma may occur in various locations. Although huge
chronic expanding hematomas in the chest have been previously
reported, they were usually caused by tuberculous pleuritis or
thoracic surgery (1–3), whereas blunt chest trauma as a causative
factor is rare. It remains unclear why chronic expanding hematomas
grow continuously. Labadie et al proposed a theory that
chronic expanding hematoma formation is a complex process of
initial hemorrhage followed by repeated organization and hemorrhage
from new microvessels beneath the capsule (5). In the present case, the patient suffered
an initial hemorrhage in his chest caused by a blunt chest trauma
25 years ago. The small hematoma did not resolve naturally, and it
grew slowly, with repeated organization and rehemorrhage. Various
factors, such as heart beating, respiratory movements and coughing
under negative pleural pressure, likely promoted the growth of the
hematoma, finally resulting in the formation of a huge mass.
Chronic expanding hematoma in the chest is difficult
to diagnose due to its rarity and slow growth, particularly for
patients without any history of surgery, tuberculosis or trauma
(6). Although a definitive diagnosis
of a chronic expanding hematoma mainly depends on histopathology,
MRI plays an important role in the differential diagnosis from
other common mediastinal tumors, such as thymoma, teratoma and
lymphoma. In the present case, the hematoma displayed various
signal intensities on T2-weighted images and exhibited a mosaic
pattern, which was previously reported as a characteristic feature
of chronic expanding hematomas (6,7). The
various intensities on the MRI images corresponded to fresh and old
blood, which was the result of repeated hemorrhages over time.
Based on this case report and the currently available literature,
the characteristics of chronic expanding hematomas in the chest are
summarized as follows: i) the patient has a mass over a relatively
long time period; ii) a history of tuberculous pleuritis, chest
surgery or trauma; iii) a mosaic pattern of various signal
intensities on T2-weighted MRI images is observed; and iv) no
positive results are found by preoperative biopsy examination.
Thus, a chronic expanding hematoma of the chest should be taken
into consideration if the case is consistent with the
abovementioned characteristics.
Surgical resection is the main treatment for
patients with a chronic expanding hematoma to relieve the pressure
on adjacent organs. However, as reported previously, surgical
resection of these hematomas may be challenging, including a long
operative time, failure of complete resection due to the strong
adhesion of the hematoma to the surrounding tissues, and massive
intraoperative blood loss. Patients have been reported to
experience a blood loss of >1,000 ml in the majority of the
cases (1–3,6), and
massive bleeding of >10,000 ml in occasional cases (3). In the present case, the intrathoracic
lesion was completely removed with a total operative time of 140
min and a total blood loss of only 250 ml, possibly because the
patient had no history of a thoracic surgery or tuberculosis, which
often cause severe pleural adhesions and abundant neovascular
proliferation. Therefore, surgical resection is the first choice of
treatment for a chronic expanding hematoma caused by a blunt chest
trauma.
For patients who present with slowly growing
intrathoracic masses, particularly those with a history of chest
trauma and a mosaic pattern of various signal intensities on
T2-weighted MRI images, the diagnosis of a chronic expanding
hematoma should be taken into consideration and surgical resection
is the first choice of treatment.
References
|
1
|
Hanagiri T, Muranaka H, Hashimoto M,
Nishio T, Sakai S, Ono M, Toyoshima S and Nagashima A: Chronic
expanding hematoma in the chest. Ann Thorac Surg. 64:559–561. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Muramatsu T, Shimamura M, Furuichi M,
Ishimoto S, Ohmori K and Shiono M: Treatment strategies for chronic
expanding hematomas of the thorax. Surg Today. 41:1207–1210. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ogata J, Minami K, Nakamura M, Horishita T
and Sata T: The management of extirpation of chronic expanding
hematoma after thoracoplasty in the chest. Masui. 53:1286–1289.
2004.(In Japanese). PubMed/NCBI
|
|
4
|
Reid JD, Kommareddi S, Lankerani M and
Park MC: Chronic expanding hematomas. A clinicopathologic entity.
JAMA. 244:2441–2442. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Labadie EL and Glover D:
Physiopathogenesis of subdural hematomas. Part 1: Histological and
biochemical comparisons of subcutaneous hematoma in rats with
subdural hematoma in man. J Neurosurg. 45:382–392. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kuronuma K, Ootake S, Ikeda K, Taniguchi
M, Takezawa C and Takahashi H: Chronic expanding hematoma in the
chest. Intern Med. 47:1411–1414. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Akata S, Ohkubo Y, Jinho P, Saito K,
Yamagishi T, Yoshimura M, Kotake F, Kakizaki D and Abe K: MR
features of a case of chronic expanding hematoma. Clin Imaging.
24:44–46. 2000. View Article : Google Scholar : PubMed/NCBI
|