Introduction
The diffuse sclerosing variant of papillary thyroid
carcinoma (DSVPTC) was firstly reported by Vickery et al
(1) in 1985. The prevalence of this
variant among all the patients with papillary thyroid carcinoma
(PTC) ranged between 0.74 and 5.3%, as reported in a larger series
(2–4).
This is characterized by high aggressiveness, a larger tumor size,
a high incidence of cervical lymph node metastasis and distant
metastasis (3,5–9). DSVPTC is
also associated with frequent local recurrence and poor prognosis
(8–11). Therefore, patients with DSVPTC must be
treated by aggressive surgical intervention, including total
thyroidectomy, central neck dissection, bilateral neck dissections
and postoperative radioiodine treatment (3,9,10,12).
Patients with DSVPTC must be monitored closely during follow-up for
any disease recurrence or metastasis (3,7,9,12).
Clinically, the diagnosis of DSVPTC is often delayed
by months or years as a result of the clinical similarities that it
shares with autoimmune lymphocytic thyroiditis (also termed
Hashimoto's thyroiditis) (3,7,9,12). Due to the early spread of DSVPTC,
early correct diagnosis and surgical treatment is crucially
important (9). Currently, ultrasound
(US) is generally considered to be the most accurate imaging
modality for the evaluation and characterization of thyroid nodules
(13). Since DSVPTC always permeates
the entire gland causing diffuse thyroid enlargement without a
dominant nodule, which is difficult to diagnose using US, it is
more commonly diagnosed as Hashimoto's thyroiditis (12,14,15). The
present study was the first, to the best of our knowledge, to
report shear wave elastography (SWE) diagnosis of DSVPTC of the
thyroid.
Patients and methods
Patient
A 20-year-old female patient presented with a
1-month history of a neck mass and sore throat. The patient did not
received non-steroidal anti-inflammatory drugs, chemotherapy,
radiotherapy or immunotherapy. A physical examination revealed a
diffuse palpable middle-neck mass protruding on both sides. The
mass was tender, well-defined, firm and movable. Clinically, this
was suggested to be thyroiditis. Serum concentrations of
triiodothyronine (T3), thyroxine (T4), free triiodothyronine (FT3),
free thyroxine (FT4), thyroid-stimulating hormone (TSH),
thyroglobulin antibody (Tg-Ab), and thyroid peroxidase antibody
(TPO-Ab) were measured using immunochemiluminescent assays and an
automated analyzer (Unicel DXI800; Beckman Coulter, Inc., Brea, CA,
USA). Conventional US and SWE were performed using an AIXPLORER
system (Supersonic Imagine, Aix en Provence, France) with 14-5 MHz
linear transducer. Written informed consent from the patient was
obtained prior to SWE examination.
Conventional US and SWE
US examination was performed in transverse and
longitudinal planes of the thyroid with the supine position. On
conventional US, thyroid gland and lesion diameters, the extent of
disease, echogenicity, microcalcifications, vascularization and
cervical metastatic lymph nodes were assessed.
Following conventional US examination, SWE was
performed during the US examination, using the same operator, US
system and probe, which was placed on the neck with light constant
pressure. The elastography image was overlaid on the B-Mode image.
It provided a real-time map of elasticity. SWE provided results in
a color box and region-of-interest (ROI), which can be positioned
over the normal thyroid parenchyma and the nodule to measure the
stiffness of each tissue. The SWE color box, in which blue and red
areas corresponded to softer and stiffer regions, respectively, was
moved to include the target lesion. When the cine loop was stable
for ~10 sec, the operator froze it and stored the corresponding
image in the machine. For each of these ROIs, the mean, minimum and
maximum stiffness, as well as the standard deviation were
automatically calculated, which increased with increasing tissue
elasticity heterogeneity.
Histological evaluation
The samples of tumor tissue and retrieved lymph
nodes were fixed in 10% formaldehyde solution, embedded in
paraffin, cut into 4 mm sections and mounted on poly-lysine-coated
slides. These tissue sections were stained using hematoxylin and
eosin to confirm their histological diagnosis and other microscopic
characteristics. Experienced pathologists were employed to ensure a
high quality of pathological diagnosis.
Results
The patient had undergone total thyroidectomy and
bilateral neck lymph node dissection, and an intraoperative
pathological consultation to confirm the malignancy as lymph node
metastasis. The total thyroid glands and bilateral neck lymph nodes
were submitted for a pathological examination. The left lobe and
right lobe measured 6×4×3.5 and 5×3×2 cm3, respectively.
Each lobe of thyroid was tan-to-white in color and lacking any
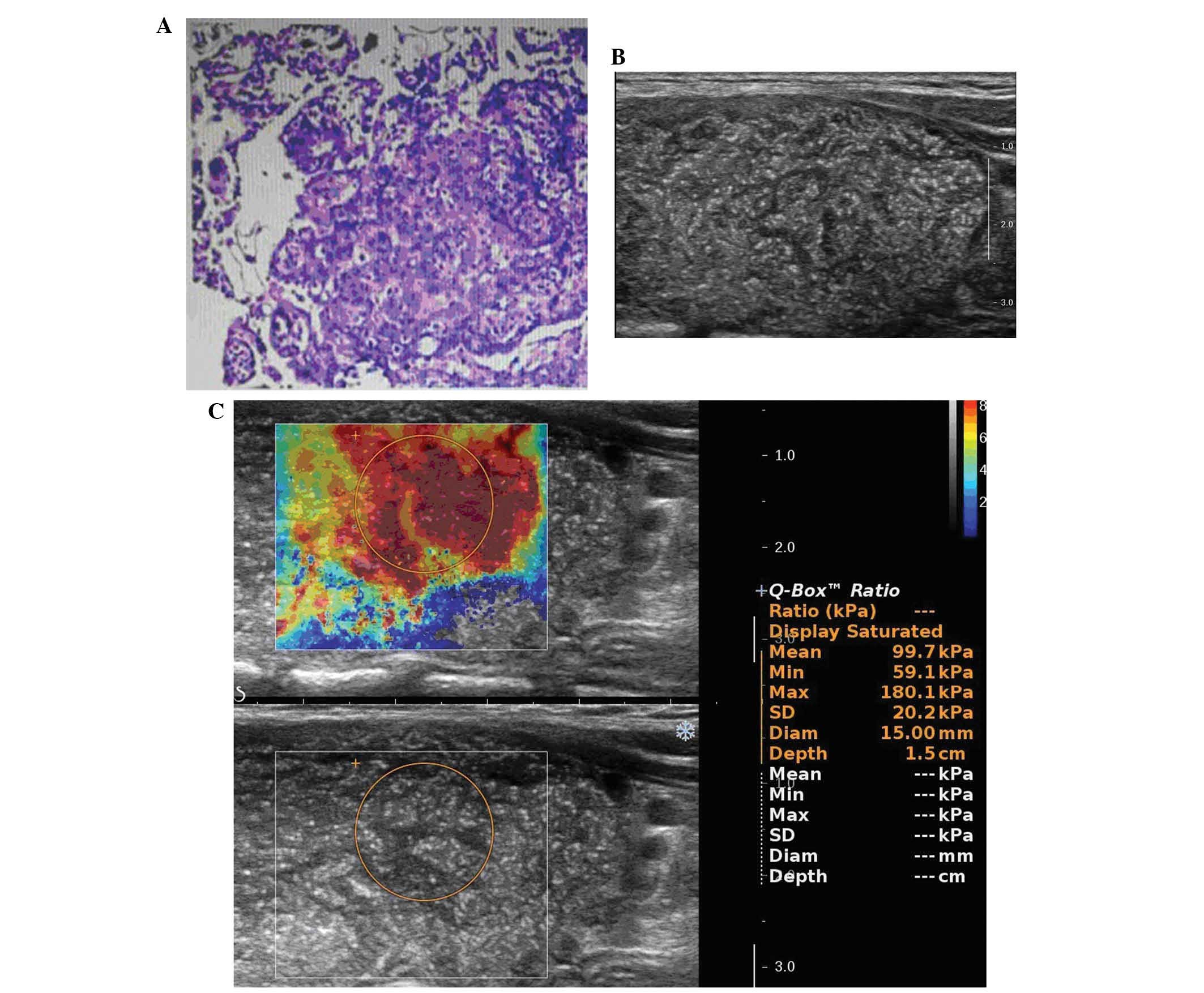
nodular masses. Pathological diagnosis was DSVPTC in each lobe
(Fig. 1A), with lymph node metastases
in the bilateral neck.
A serological analysis revealed the following: Free
T4, 0.70 ng/dl, free T3, 3.24 pg/ml, T3, 1.04 ng/ml, T4, 8.14 µg/dl
and TSH, 7.79 IU/ml. Each antithyroid antibody was positive:
Anti-thyroglobulin, >2,380.0 IU/ml and anti-thyroid peroxidase,
254.80 IU/ml.
Thyroid ultrasonography revealed diffuse enlargement
of the both lobes, heterogenous echogenicity without mass
formation, diffuse scattered microcalcifications (Fig. 1B) and poor vascularization. It also
revealed enlarged bilateral neck lymph nodes, an absence of a
normal lymph hilum and structural disorder of the corticomedullary,
without calcification.
SWE revealed stiff values of the thyroid: The mean
stiffness was 99.7 kpa, the minimum stiffness was 59.1 kpa and the
maximum stiffness was 180.1 kpa (Fig.
1C).
Discussion
Compared with classic PTC, DSVPTC occurs most
frequently in young females and may be mistaken clinically for
Hashimoto's thyroiditis (3,7,9,12). It generally has a greater tendency for
lymph node metastasis and distant metastasis, and worse
disease-free survival compared with other PTC variants (8–11). Due to
its strong aggressiveness and early metastasis, total thyroidectomy
with lymph node dissection and postoperative radioiodine ablation
are recommended, and a close follow-up is necessary (3,7,9,10,12).
Although DSVPTC is rare (16), it is important for clinicians to
recognize and consider the possibility of this disease,
particularly because of its clinical resemblance to Hashimoto's
thyroiditis (3,9). Patients are frequently misdiagnosed and
treated for Hashimoto's thyroiditis (7,9,14). In the present case, the clinical
presentation and serological findings were all indicative of
Hashimoto's thyroiditis.
Sonography is generally considered as the most
accurate imaging modality for the evaluation and characterization
of thyroid nodules (13). However,
the diffuse nature of DSVPTC often mimics chronic thyroiditis on US
images and leads to treatment delay, particularly in the absence of
a focal solid mass (14,15). In the present case, thyroid
ultrasonography revealed diffuse enlargement of each lobe and
heterogenous echogenicity without focal solid mass formation. The
preliminary ultrasonic diagnostic impression was of Hashimoto's
thyroiditis. It is well known that microcalcifications within a
solitary thyroid mass on sonography are generally regarded as the
most reliable indicators of malignancy (17). Since the present case showed diffuse
scattered microcalcifications, it is imperative to accurately
identify the underlying papillary carcinoma. Subsequently, SWE were
performed during the US examination.
Elastography is a sonographic method of assessing
tissue stiffness. Numerous previous studies reported decreased
elasticity of malignant thyroid nodules (18–20). Since
the older variants of elastography determines tissue elasticity in
relation to surrounding tissue (20),
it may influence the diagnostic performance of diffuse disease,
including DSVPTC, coexisting subacute thyroiditis and Hashimoto's
thyroiditis. SWE is a novel, promising, user-independent and
real-time, quantitative (20–24), but not widely available technique. In
SWE (20–24), SWE is induced by a focused ultrasonic
beam. Based on the received signals, the elasticity of the tissue
is assessed in real-time and may be estimated both qualitatively
and quantitatively. It is thought to be more objective, reliable
and reproducible compared with older variants of elastography, as
it does not require any compressive maneuvers (20,22,24).
Previous studies on SWE demonstrated very significant differences
in elasticity between benign and malignant lesions (20,21,23–25).
To the best of our knowledge, SWE diagnosis of DSVPTC of the
thyroid remains to be described.
Numerous previous studies of SWE have demonstrated
that a cut-off value of maximum stiffness >65 kPa for diagnosing
the malignant thyroid nodules had a sensitivity of 85.2% and
specificity of 93.9% (24). The mean
stiffness of Hashimoto's thyroiditis was 24.0±10.5 kpa (21). In the present case, SWE showed stiff
values of the thyroid: The mean stiffness was 99.7 kpa, the minimum
stiffness was 59.1 kpa and the maximum stiffness was 180.1 kpa. The
maximum stiffness of the DSVPTC (180.1 kpa) was higher compared
with the diagnostic criteria of malignant thyroid nodules (65 kPa).
This may suggest the benefit of diagnosing DSVPTC by SWE.
The present study was limited in terms of the study
population. Since only 1 patient was assessed, the population was
too small to draw any definite conclusions. Therefore, multi-center
prospective studies with larger numbers of sample are required in
future investigations.
In conclusion, SWE is an important imaging tool in
the diagnosis of DSVPTC. Since patients with DSVPTC may present
with typical clinicopathological features and initially appear to
have Hashimoto's thyroiditis, a thorough clinical evaluation and an
early diagnosis are important. DSVPTC requires more aggressive
surgical intervention and it is therefore important to diagnose
this as quickly as possible to ensure the correct treatment is
provided.
References
|
1
|
Vickery AL Jr, Carcangiu ML, Johannessen
JV and Sobrinho-Simoes M: Papillary carcinoma. Semin Diagn Pathol.
2:90–100. 1985.PubMed/NCBI
|
|
2
|
Lam AK, Lo CY and Lam KS: Papillary
carcinoma of thyroid: A 30-yr clinicopathological review of the
histological variants. Endocr Pathol. 16:323–330. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Thompson LD, Wieneke JA and Heffess CS:
Diffuse sclerosing variant of papillary thyroid carcinoma: A
clinicopathologic and immunophenotypic analysis of 22 cases. Endocr
Pathol. 16:331–348. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chow SM, Chan JK, Law SC, Tang DL, Ho CM,
Cheung WY, Wong IS and Lau WH: Diffuse sclerosing variant of
papillary thyroid carcinoma-clinical features and outcome. Eur J
Surg Oncol. 29:446–449. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Carcangiu ML and Bianchi S: Diffuse
sclerosing variant of papillary thyroid carcinoma.
Clinicopathologic study of 15 cases. Am J Surg Pathol.
13:1041–1049. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Imamura Y, Kasahara Y and Fukuda M:
Multiple brain metastases from a diffuse sclerosing variant of
papillary carcinoma of the thyroid. Endocr Pathol. 11:97–108. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Akaishi J, Sugino K, Kameyama K, Masaki C,
Matsuzu K, Suzuki A, Uruno T, Ohkuwa K, Shibuya H, Kitagawa W, et
al: Clinicopathologic features and outcomes in patients with
diffuse sclerosing variant of papillary thyroid carcinoma. World J
Surg. 39:1728–1735. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Falvo L, Giacomelli L, D'Andrea V,
Marzullo A, Guerriero G and de Antoni E: Prognostic importance of
sclerosing variant in papillary thyroid carcinoma. Am Surg.
72:438–444. 2006.PubMed/NCBI
|
|
9
|
Chen CC, Chen WC, Peng SL and Huang SM:
Diffuse sclerosing variant of thyroid papillary carcinoma:
Diagnostic challenges occur with Hashimoto's thyroiditis. J Formos
Med Assoc. 112:358–362. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fukushima M, Ito Y, Hirokawa M, Akasu H,
Shimizu K and Miyauchi A: Clinicopathologic characteristics and
prognosis of diffuse sclerosing variant of papillary thyroid
carcinoma in Japan: An 18-year experience at a single institution.
World J Surg. 33:958–962. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Regalbuto C, Malandrino P, Tumminia A, Le
Moli R, Vigneri R and Pezzino V: A diffuse sclerosing variant of
papillary thyroid carcinoma: Clinical and pathologic features and
outcomes of 34 consecutive cases. Thyroid. 21:383–389. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Marshall CB: Diffuse sclerosing variant of
papillary thyroid carcinoma preoperative diagnosis through imaging
and cytology allows for optimal patient care. Pathology Case
Reviews. 20:125–128. 2015. View Article : Google Scholar
|
|
13
|
Pacini F, Schlumberger M, Dralle H, Elisei
R, Smit JW and Wiersinga W: European Thyroid Cancer Taskforce:
European consensus for the management of patients with
differentiated thyroid carcinoma of the follicular epithelium. Eur
J Endocrinol. 154:787–803. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kim HS, Han BK, Shin JH, Ko EY, Sung CO,
Oh YL and Song SY: Papillary thyroid carcinoma of a diffuse
sclerosing variant: Ultrasonographic monitoring from a normal
thyroid gland to mass formation. Korean J Radiol. 11:579–582. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Martín-Pérez E, Larrañaga E and Serrano P:
Diffuse sclerosing variant of papillary carcinoma of the thyroid.
Eur J Surg. 164:713–715. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sheu SY, Schwertheim S, Worm K, Grabellus
F and Schmid KW: Diffuse sclerosing variant of papillary thyroid
carcinoma: Lack of BRAF mutation but occurrence of RET/PTC
rearrangements. Mod Pathol. 20:779–787. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zhang Y, Xia D, Lin P, Gao L, Li G and
Zhang W: Sonographic findings of the diffuse sclerosing variant of
papillary carcinoma of the thyroid. J Ultrasound Med. 29:1223–1226.
2010.PubMed/NCBI
|
|
18
|
Shuzhen C: Comparison analysis between
conventional ultrasonography and ultrasound elastography of thyroid
nodules. Eur J Radiol. 81:1806–1811. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wang Y, Dan HJ, Dan HY, Li T and Hu B:
Differential diagnosis of small single solid thyroid nodules using
real-time ultrasound elastography. J Int Med Res. 38:466–472. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Liu BX, Xie XY, Liang JY, Zheng YL, Huang
GL, Zhou LY, Wang Z, Xu M and Lu MD: Shear wave elastography versus
real-time elastography on evaluation thyroid nodules: A preliminary
study. Eur J Radiol. 83:1135–1143. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Magri F, Chytiris S, Capelli V, Alessi S,
Nalon E, Rotondi M, Cassibba S, Calliada F and Chiovato L: Shear
wave elastography in the diagnosis of thyroid nodules: Feasibility
in the case of coexistent chronic autoimmune Hashimoto's
thyroiditis. Clin Endocrinol (Oxf). 76:137–141. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lee EJ, Jung HK, Ko KH, Lee JT and Yoon
JH: Diagnostic performances of shear wave elastography: Which
parameter to use in differential diagnosis of solid breast masses?
Eur Radiol. 23:1803–1811. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Liu B, Liang J, Zheng Y, Xie X, Huang G,
Zhou L, Wang W and Lu M: Two-dimensional shear wave elastography as
promising diagnostic tool for predicting malignant thyroid nodules:
A prospective single-centre experience. Eur Radiol. 25:624–634.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Veyrieres JB, Albarel F, Lombard JV,
Berbis J, Sebag F, Oliver C and Petit P: A threshold value in Shear
Wave elastography to rule out malignant thyroid nodules: A reality?
Eur J Radiol. 81:3965–3972. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sebag F, Vaillant-Lombard J, Berbis J,
Griset V, Henry JF, Petit P and Oliver C: Shear wave elastography:
A new ultrasound imaging mode for the differential diagnosis of
benign and malignant thyroid nodules. J Clin Endocrinol Metab.
95:5281–5288. 2010. View Article : Google Scholar : PubMed/NCBI
|