Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most
common type of non-Hodgkin lymphoma (NHL), representing ~30–40% of
all NHL cases (1), and is
characterized by an aggressive phenotype. Although the
incorporation of the monoclonal antibody rituximab into the
treatment paradigm for DLBCL has resulted in improved complete
response (CR), progression-free survival (PFS) and overall survival
(OS) (2–6), there is a disparity in outcomes among
patients with high-risk characteristics, calling for more effective
first-line treatment strategies. Specifically, modification of
treatment strategies must be considered in patients with activated
B-cell (ABC) origin and/or secondary extranodal involvement,
entities representing different aggressive biological subsets that
manifest altered clinical behavior (7–9).
One such strategy is the use of dose-dense induction
chemotherapy, which was investigated in patients with DLBCL prior
to the design of the present study, with a reported benefit
(10). A number of trials have since
reported comparable results for cyclophosphamide, doxorubicin,
vincristine, prednisone, and rituximab every 14 days (CHOP-R-14)
vs. CHOP-R-21, suggesting the need for more effective alternative
approaches, such as consolidation therapy (11,12).
Consolidation with the radioimmunoconjugate
90Y-ibritumomab tiuxetan (90Y-ibritumomab;
Zevalin®; Biogen IDEC, Weston, MA, USA and Spectrum
Pharmaceuticals, Irvine, CA, USA) has yielded promising responses
and survival outcomes in the first-line and salvage settings
(2-year PFS and OS rates as high as 85 and 95%, respectively) in
NHL, including DLBCL (13–18). An open-label phase 2 single-center
pilot study was designed, with the objective of evaluating the
efficacy and safety of the combination of CHOP-R-14 and
90Y-ibritumomab in treatment-naive high-risk DLBCL
patients. This is the first report of our results with a long-term
follow-up.
Materials and methods
Patients
Eligible patients were aged ≥18 years, with
previously untreated, confirmed CD20+ DLBCL with
measurable disease, a World Health Organization (WHO) performance
status of 0–2, an International Prognostic Index (IPI) score of ≥2,
and a life expectancy of ≥3 months. Acceptable organ function was
required and defined as follows: Adequate hematological [absolute
neutrophil count (ANC) ≥1,500/mm3 and platelet count
≥150,000/mm3], hepatic (total bilirubin ≤2.0 mg/dl),
renal (serum creatinine ≤2.0 mg/dl), and normal cardiac function.
Patients were excluded if they had central nervous system (CNS)
lymphoma, HIV/AIDS, pleural effusion, or any serious non-malignant
disease or infection. Those who had received prior RIT,
anthracyclines, or external beam radiation therapy (involved field
or regional) to >25% of active bone marrow were also excluded.
The patients were not permitted to receive rituximab 4 weeks prior
to enrollment, or granulocyte colony-stimulating factor or
granulocyte-macrophage colony-stimulating factor within 2 weeks
prior to treatment.
Study design
Patients were enrolled between September, 2004 and
July, 2009. The treatment included 6 cycles of CHOP-R-14
chemotherapy every 2 weeks, with rituximab 375 mg/m2 IV
on day 1, cyclophosphamide 750 mg/m2 on day 1,
doxorubicin 50 mg/m2 on day 1, vincristine 1.4
mg/m2 (maximum 2 mg) on day 1, and prednisone 100 mg on
days 1–5. Pegfilgrastim was administered at a fixed dose (6 mg
subcutaneously) 24 h after each CHOP-R-14 cycle.
The patients were restaged after 4
cycles of CHOP-R-14
Those with documented response [CR or partial
response (PR)] continued therapy with an additional 2 cycles of
chemo-immunotherapy. Within 4–6 weeks after the sixth cycle of
CHOP-R-14, the patients who maintained a CR or PR with <25%
lymphoma burden in the marrow and adequate hematological reserve,
received one course of 90Y-ibritumomab; the dose was
adjusted according to the platelet count (0.4 mCi/kg for platelet
counts ≥150,000/mm3; and 0.3 mCi/kg for platelet counts
100,000–149,000/mm3; maximum dose of 32 mCi). The course
of 90Y-ibritumomab consisted of an initial infusion of
rituximab 250 mg/m2 on day 1, another infusion of
rituximab 250 mg/m2 on day 7, 8, or 9, followed by a
weight-based dose of 90Y-ibritumomab.
All the patients provided written
informed consent
The study was conducted in accordance with the
Declaration of Helsinki and approved by our Institutional Review
Board, as well as the Food and Drug Administration (IND # BB-IND
11065). Registration with ClinicalTrials.gov was not required at the time of
study initiation.
Response evaluations and outcome
measures
The baseline assessments performed within 4 weeks
prior to patient registration included medical history, physical
examination, clinical laboratory tests [complete blood count (CBC)
and serum chemistries] and computed tomography (CT) scans.
Bilateral bone marrow biopsy and aspirates were obtained within 6
weeks of patient registration to stage the patient. Lymphomas with
dominant lymph node and/or spleen involvement were considered as
primary nodal (PN). Those with disease involving nodal as well as
extranodal sites (including the bone marrow) were considered as PNs
with secondary extranodal (SEN) involvement. Lymphomas with minor
or no lymph node involvement arising in extranodal organs other
than the spleen were considered as primary extranodal (PEN).
Baseline assessments were repeated for restaging at the end of the
CHOP-R-14 treatment period and at 1 month after treatment with
90Y-ibritumomab. Tumor response was based on
International Workshop Criteria (19) and did not require positron emission
tomography (PET) scans. Disease status was monitored in the
follow-up period every 3 months for the first year and every 6
months thereafter, for a total of 4 years on study. The primary
endpoints of the study included response [CR, PR and overall
response rate (ORR)] and safety of administering CHOP-R-14 and
90Y-ibritumomab to patients with previously untreated
DLBCL. Using the Hans criteria, germinal center (GC) vs. ABC origin
was defined retrospectively based on immunohistochemical staining
for CD10, B-cell lymphoma-6 and multiple myeloma oncogene-1
(20).
Toxicity evaluations
During active treatment, hematological toxicities
were assessed weekly. Dose-limiting hematological values included
an ANC <1,500/mm3 and/or hemoglobin level <10 g/dl
and/or platelet count <100/mm3. Hematological and
non-hematological toxicities were graded using the National Cancer
Institute (NCI) Toxicity Criteria. A CBC was obtained weekly for
the first 12 weeks following administration of
90Y-ibritumomab and at 6-month intervals thereafter for
the duration of the patient's life. During this time, serious
adverse events (AEs) and any new or worsening drug-related AEs were
reported. AEs occurring after the initiation of subsequent
anticancer therapy were not reported, unless the AE occurred within
30 days of 90Y-ibritumomab administration, or the event
was likely to be related to RIT.
Statistical analysis
This study was powered to ensure the safety of the
combined CHOP-R-14 and 90Y-ibritumomab regimen based on
the most likely dose toxicity, which was estimated to be
hematological. Using a Simon 2-stage design (21), 60% (p0) was set as the proportion of
expected hematological toxicity. Patients with clinically
significant grade 3/4 hematological toxicity with CHOP-R-14
(requiring dose delay, dose reduction, or resulting in any severe
AEs) and/or with any grade 3/4 hematological toxicity after RIT
counted toward the threshold of 80%, defined as an unacceptable
proportion of toxicity (p1). Using these parameters with α=0.09 and
β=0.2, accrual of 11 patients during stage 1 was required, with
plans to terminate the study at the first stage should ≥7 patients
experience grade 3 or 4 hematological toxicity, as defined above.
With this model, the expected sample size was 18, with a 62%
probability of terminating the study at the first stage.
Response rates (CR, PR, and ORR) were calculated for
all the patients after treatment with CHOP-R-14, and again after
treatment with 90Y-ibritumomab. The ORR included
patients with a PR or CR after treatment. Survival data were
estimated using the Kaplan-Meier method with median estimates and
95% confidence intervals generated up to the time of the last event
(22). PFS was calculated from the
date of initiation of cycle 1 of CHOP-R-14 therapy to the date of
documented relapse, disease progression, or death from any cause.
OS was calculated from the date of initiation of cycle 1 of
CHOP-R-14 therapy to the date of death from any cause. Survival
outcomes in patients with GCB vs. ABC origin and PN/PEN vs. SEN
disease were compared using t-tests, with statistical
significance defined by a P-value of <0.05.
Results
Patient disposition
A total of 20 patients were enrolled at the Rush
University Medical Center (Chicago, USA). The patient baseline
characteristics are summarized in Table
I. The majority of the patients exhibited characteristics
conferring increased risk of relapse, with bulky disease in 14
(70%), an intermediate-high IPI score in 11 (55%), secondary
extranodal disease in 9 (45%) and ABC origin in 9 (45%) patients. A
total of 18 patients completed 6 cycles of CHOP-R-14 (1 patient
withdrew consent after 5 cycles, and 1 patient with extranodal lung
masses discontinued treatment after 5 cycles due to AEs). Of these
18 patients, 16 proceeded with RIT. One patient was excluded from
receiving RIT due to bronchiolitis obliterans with organizing
pneumonia (BOOP), and the other due to abnormal
111Y-ibritumomab lung biodistribution without clinical
or radiographical evidence of pathology. The median follow-up time
for all patients (n=20) was 89.7 months (range, 22.9–128.2
months).
 | Table I.Patient demographics and baseline
characteristics. |
Table I.
Patient demographics and baseline
characteristics.
| Parameters | Patients (n=20) |
|---|
| Male, n
(%) | 8 (40) |
| Age, years |
|
|
Median | 60 |
|
Range | 33–81 |
| Race, n (%) |
|
|
Caucasian | 12 (60) |
|
Hispanic | 4 (20) |
|
Unknown | 4 (20) |
| B symptoms, n
(%) |
|
|
Yes | 5 (25) |
| No | 15 (75) |
| Performance status
at diagnosis, n (%) |
|
| 0 | 18 (90) |
| 1 | 2 (10) |
| LDH at diagnosis, n
(%) |
|
| ≤240
IU/l | 3 (15) |
| >240
IU/l | 17 (85) |
| Stage at diagnosis,
n (%) |
|
| 2 | 2 (10) |
| 3 | 10 (50) |
| 4 | 8 (40)a |
| Bone marrow
involvement, n (%) |
|
|
Yes | 4 (20) |
| No | 16 (80) |
| Sites of disease, n
(%) |
|
| Primary
nodal | 14 (70) |
| Primary
extranodal | 6 (30) |
|
Secondary extranodal
(including bone marrow involvement) | 9 (45)b |
| Cell origin, n
(%) |
|
|
Germinal center | 7 (35) |
|
Activated B-cell | 9 (45) |
|
Unknown | 4 (20) |
| Bulky disease, n
(%) |
|
| No | 6 (30) |
| >5
cm | 6 (30) |
| >10
cm | 8 (40) |
| IPI score, n
(%) |
|
| 2 | 9 (45) |
| 3 | 11 (55) |
Efficacy and survival outcomes
Intent-to-treat analyses were used to determine
efficacy and survival outcomes. After ≥4 cycles of CHOP-R-14, a
response was achieved in all the patients, namely a CR in 15
patients (75%) and a PR in 5 patients (25%). A total of 16 patients
(11 in CR and 5 in PR) subsequently received
90Y-ibritumomab; of these 16 patients, 15 achieved a CR
and 1 maintained a PR. Of note, among the 5 patients with a PR
following chemo-immunotherapy induction, 4 patients (80%) converted
to a CR after treatment with RIT. Those patients who did not
proceed with RIT remain in CR, making the final CR rate in the
entire cohort 95%.
A total of 5 patients relapsed, 3 of whom within 6
months after 90Y-ibritumomab treatment; these patients
had extensive secondary extranodal involvement and/or bulky
disease. One of these patients achieved a CR to second-line
chemotherapy followed by autologous stem cell transplantation,
while the other 2 patients developed progressive disease refractory
to second-line chemotherapy. The remaining 2 patients developed
late (after 2 years) relapse in the CNS and achieved a CR with
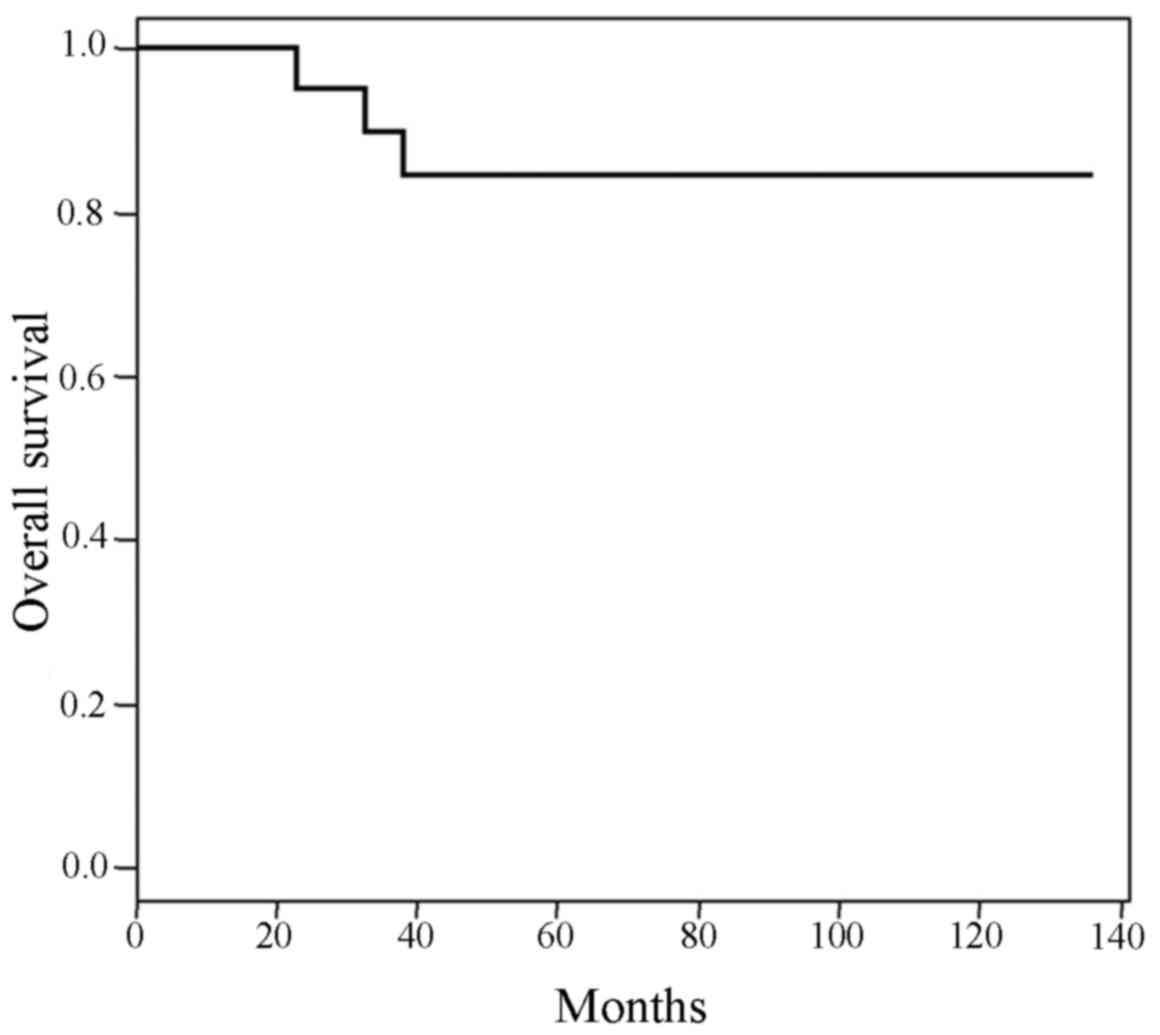
salvage therapy. Survival outcomes were determined at a median
follow-up of 89.7 months: The PFS for the entire cohort was 75%
(Fig. 1) and the OS for the entire
cohort was 85% (Fig. 2). There was
no difference in PFS or OS in patients with GC vs. ABC origin or
those with PN/PEN vs. SEN involvement (P>0.4–0.8).
Safety
Hematological AEs were common in patients after
CHOP-R-14 and 90Y-ibritumomab treatment. The rates of
grade 3 or 4 hematological toxicities with CHOP-R-14 were as
follows: 60% with neutropenia (n=12), 25% with anemia (n=5) and 20%
with thrombocytopenia (n=4). Of note, 4 of these patients had bone
marrow involvement at diagnosis. Only 5 patients (25%) required
dose delay/reduction, with 1 patient suffering a serious AE as a
result of hematological toxicity (hospitalized with fever). Grade 3
neutropenic fever was reported in 4 patients (20%) undergoing
CHOP-R-14 therapy. Assuming 120 anticipated cycles of chemotherapy
to be delivered (6 cycles/patient for 20 patients), there was a
delay in 14 cycles (12%) and 2 cycles were omitted (2%); not all
delays/omissions were attributed to hematological toxicity. A total
of 4 patients required erythrocyte-stimulating agents.
Of the 16 patients receiving RIT, 8 (50%) had grade
3 or 4 hematological toxicity (anemia in 1, neutropenia in 8 and
thrombocytopenia in 2 patients). Of these 8 patients, 5 also
developed grade 3 or 4 cytopenias with CHOP-R-14. After RIT, the
median nadir of neutropenia was 930/mm3 and no
neutropenic fevers were reported. The incidence of hematological
toxicity did not meet the criteria to terminate the study at the
first stage (only 6 of the first 11 patients met criteria counted
towards the stopping threshold). The most common non-hematological
AEs occurring in >10% of the patients included gastrointestinal
events, neuropathy and infections. All these AEs were more common
after treatment with CHOP-R-14 rather than with RIT, the majority
of which were of grade 1 or 2 severity. Four patients (20%)
experienced grade 3 neuropathy after CHOP-R-14, persisting into the
RIT phase of the trial, with no new cases reported. Infections were
low-grade and occurred more commonly during CHOP-R-14 therapy (60%)
than during subsequent 90Y-ibritumomab therapy
(38%).
No deaths occurred during the CHOP-R-14 or
90Y-ibritumomab treatment periods. A total of 3 deaths
were reported during follow-up: Two patients succumbed to disease
progression after receiving RIT at 18.5 and 34 months,
respectively; the third patient succumbed to BOOP 30 months after
completing 5 cycles of CHOP-R-14 (and excluded from the RIT phase).
There were no other serious AEs reported in patients during
follow-up.
Discussion
Despite the survival advantage conferred by the
addition of rituximab to chemotherapy for the treatment of DLBCL,
the clinical course of patients with this type of lymphoma remains
heterogeneous and unpredictable (1,23). Novel
therapeutic strategies tailored to specific high-risk
clinicopathological characteristics are required to optimize care.
Our study investigated the efficacy and safety of first-line
dose-dense CHOP-R-14 induction followed by
90Y-ibritumomab consolidation in patients with high-risk
clinical and biological characteristics. The results appeared to be
promising as compared with those reported by the Groupe d'Etude des
Lymphomes de l'Adulte (GELA) at 5 years of follow-up in patients
receiving CHOP-R-21 (5-year PFS rates stratified according to IPI
of 69 and 47% in low- and high-risk patients, respectively),
maintained during a long-term follow-up of 89.7 months (24).
At the time of designing this study, the rationale
for the use of CHOP-R-14 was based on German data demonstrating the
superiority of CHOP-14 over CHOP-21, with improved 5-year
event-free survival and OS rates (10). The RICOVER-60 trial has since
established the synergistic effects of combining 6 cycles of
dose-intensified CHOP-14 with rituximab in patients aged >60
years (25). However, in time, the
relative benefit of dose-dense chemo-immunotherapy has not held up
in head-to-head comparisons of standard CHOP-R-21 with CHOP-R-14:
Cunningham et al demonstrated similar response rates [ORR,
88 vs. 91% (P<0.139) and CR/unconfirmed CR (CRu), 63 vs. 58%
(P<0.183), respectively] and survival outcomes with CHOP-R-14
and CHOP-R-21 (11). These results
were corroborated by GELA in elderly patients with DLBCL (12). By contrast, dose intensification with
R-ACVBP has demonstrated a significant survival advantage in young
patients with low- or low-intermediate-risk disease compared with
CHOP-R-21, but with an associated significant increase in toxicity,
raising questions of the generalizability of such a regimen
(26). Similarly, in high-risk
DLBCL, a subset analysis of the SWOG trial suggested a benefit to
dose intensification via high-dose chemotherapy with stem cell
rescue. This was, however, an unplanned analysis in a population
that was heterogeneously treated with immunotherapy and not
translatable to an older population (27). Taken collectively, these studies
suggest that manipulation of chemo-immunotherapy induction alone is
not optimal for improving clinical outcomes. Our study is
innovative in investigating radioimmunotherapy consolidation with
dose-dense chemo-immunotherapy as an alternative therapeutic
strategy.
Over the last decade, RIT has emerged as a safe and
effective consolidative strategy in indolent as well as aggressive
lymphomas, most effective when administered earlier during the
disease course. In patients with high-risk DLBCL, several studies
have confirmed the benefit of first-line RIT consolidation
following chemo-immunotherapy (Table
II). For example, Zinzani et al administered
90Y-ibritumomab consolidation after 4 cycles of
CHOP-R-21 in 48 high-risk elderly (≥60 years) patients with DLBCL.
The CR rates improved from 58% after CHOP-R-21 to 73% after RIT,
with a 50% PR to CR conversion rate after
90Y-ibritumomab (18).
After a median follow-up of 18 months, the estimated 2-year PFS and
OS rates were 85 and 86%, respectively. Similar results with RIT
have been published in comparable high-risk patient populations,
including those with bulky disease (28–31).
Although direct comparisons of these studies to our own cannot be
made, our study demonstrated higher CR rates after dose-dense
chemo-immunotherapy (75%) augmented by RIT (95% CR; 80% PR to CR
conversion rate), with durable responses maintained over >7
years of follow-up.
| Table II.Studies using RIT consolidation in
the first-line setting in patients with highrisk DLBCL. |
Table II.
Studies using RIT consolidation in
the first-line setting in patients with highrisk DLBCL.
| Study, year | N (number on
RIT) | High-risk
characteristics | Treatment
regimen | Response rates with
RIT | Survival | Refs. |
|---|
| Hamlin et
al, 2010 | 63 (44) | Age >60
years-Age adjusted intermediate-high and high-risk IPI | CHOP-R-21 ×6 →
90Y-ibritumomab tiuxetan | PR or CRu →CR: 16%
Final CR/CRu: 86% | Median f/u: 42
months PFS: 62% OS: 64% | (28) |
| Yang et al,
2009 | 20 (20) | Bulky disease | CHOP-R-21 ×6 →
90Y-ibritumomab tiuxetan | PR →CR: 67% Final
CR: 90% | Median f/u: 17.5
months 2year PFS: 78.9±9.1% OS: NR | (29) |
| Zinzani et
al, 2010 | 55 (48) | Age >60
years | CHOP-R-21 ×4 →
90Y-ibritumomab tiuxetan | PR →CR: 50% Final
CR: 73% | Median f/u: 18
months 2-year PFS: 85% 2-year OS: 86% | (18) |
| Kraeber-Bodere
et al, 2010 | 29 (23) | Age >60
years | CHOP-R-14 ×6 →
90Y-epratuzumab tetraxetan | PR →CR:30.7% Final
CR: 56.5% | Median f/u: 12
months PFS: 75% OS: 83% | (30) |
| Friedberg et
al, 2010 | 84 (50) | Bulky disease or
advanced stage | CHOP-R-21 ×6 →
CHOP-21 × 2 → Iodine- 131 tositumomab | PR →CR: NR Final
CR: NR PR →CR: 80% | Median f/u: 12
months PFS: 75% OS: 83% Median f/u: 89.7 months | (31) |
| Karmali et
al, present study | 20 (16) | 90% of patients
with ≥1 highrisk characteristic: 55% IPI ≥3, 70% bulky disease, 45%
SEN site, 45% nonGC origin | CHOP-R-14 ×6 →
90Y-ibritumomab tiuxetan | Final CR: 94% | PFS: 75% OS:
85% |
|
|
Our study accrued a substantial number of patients
with secondary extranodal involvement and bulky disease, other
high-risk characteristics associated with late relapse (32). Consolidation with RIT was able to
achieve reasonable survival outcomes in these patients, suggesting
a role in eradicating minimal residual disease, a likely reason for
late relapse. At best, given our small sample size, there were
signals of activity of the immunomodulatory effects of RIT in GC
and ABC patients. Targeted approaches to the underlying biology
associated with cell of origin may be more effective, as
demonstrated with early-phase trials with agents such as
lenalidomide and ibrutinib, specifically for ABC-origin DLBCL
(33,34).
Our small sample size and the inability to accrue 20
patients completing treatment in its entirety due to limited
resources is a shortcoming that makes conclusions on toxicity
difficult as well. For patients that did undergo therapy,
toxicities were not unexpected, with an observed incidence and
severity consistent with those of other studies using CHOP-R-14
and/or 90Y-ibritumomab in patients with DLBCL (16,18,19,35). By
the completion of this study, clinically significant grade 3/4
hematological toxicities after chemotherapy and/or any grade 3/4
toxicity after RIT was observed in 10 patients, with only 1 patient
suffering a serious AE; all were manageable with treatment
interruption and standard medical interventions. In the CHOP-R-14
phase of the trial, 87% of the cycles were delivered in a timely
manner. A total of 18 patients completed all 6 cycles of CHOP-R-14
and the remaining 2 patients completed 5 cycles; only 3 patients
had hematological toxicities accounting for cycle delays/omissions.
There were no grade 3/4 infections or cases of neutropenic fever
following RIT, despite a 56% rate of grade 3 or 4 neutropenia with
consolidation. Neuropathy was the most common non-hematological
toxicity following chemo-immunotherapy; a decrease in all grades of
neuropathy post-RIT implicates CHOP-R-14 rather than RIT as the
likely cause. A similar association between CHOP-R-14 and
neuropathy was observed in the RICOVER-60 trial after the treatment
of elderly patients with CHOP-R-14 (36).
In the present study, no cases of secondary AML/MDS
were reported. Despite these reassuring findings, longer follow-up
is required to definitively determine the risk of development of
therapy-related myelodysplastic syndrome/acute myeloid leukemia
attributed to combinations of RIT and
anthracyclines/alkylators.
Several large randomized controlled trials have
evaluated the safety and efficacy of dose-dense
chemo-immnunotherapy in DLBCL with equivocal results, suggesting
the need for alternative strategies. To the best of our knowledge,
our trial is the first designed to investigate the efficacy of
combining dose-dense CHOP-R-14 with RIT consolidation and the first
to report survival outcomes with the longest follow-up post-RIT
consolidation in DLBCL to date. Our high-risk patients achieved
durable responses with acceptable toxicities in the first-line
setting. There were several limitations to our study, including the
small sample size and incomplete accrual; thus, our results on
efficacy must be interpreted with caution. Additionally, our study
predates the PET era. Nonetheless, our long-term follow-up provides
a reliable measure of response, with evidence of benefit in
patients with high-risk characteristics. In an era of targeted
therapies, we consider that closer investigation of RIT
consolidation should not be entirely abandoned as a potential
treatment option in DLBCL.
Acknowledgements
The authors wish to thank the staff of the Rush
University Cancer Center for their assistance in conducting this
study, the patients for their participation, and Dr Amjad Ali
(Department of Diagnostic Radiology and Nuclear Medicine) for his
active involvement in the study. This study was supported by Biogen
IDEC (Weston, MA, USA) and Spectrum Pharmaceuticals, Inc. (Irvine,
CA, USA). Dr Stephanie A. Gregory has received research support
from Biogen IDEC and is on the Advisory Panel for Spectrum
Pharmaceuticals. Dr Venugopal participated in the speaker's bureau
with and received research support from Biogen IDEC. Teresa O'Brien
was a consultant and participated in the speaker's bureau with
Biogen IDEC.
References
|
1
|
Flowers CR, Sinha R and Vose JM: Improving
outcomes for patients with diffuse large B-cell lymphoma. CA Cancer
J Clin. 60:393–408. 2010.PubMed/NCBI
|
|
2
|
Coiffier B, Thieblemont C, Van Den Neste
E, Lepeu G, Plantier I, Castaigne S, Lefort S, Marit G, Macro M,
Sebban C, et al: Long-term outcome of patients in the LNH-98.5
trial, the first randomized study comparing rituximab-CHOP to
standard CHOP chemotherapy in DLBCL patients: A study by the Groupe
d'Etudes des Lymphomes de l'Adulte. Blood. 116:2040–2045. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pfreundschuh M, Trümper L, Osterborg A,
Pettengell R, Trneny M, Imrie K, Ma D, Gill D, Walewski J, Zinzani
PL, et al: CHOP-like chemotherapy plus rituximab versus CHOP-like
chemotherapy alone in young patients with good-prognosis diffuse
large-B-cell lymphoma: A randomised controlled trial by the
MabThera International Trial (MInT) Group. Lancet Oncol. 7:379–391.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wilson WH, Dunleavy K, Pittaluga S, Hegde
U, Grant N, Steinberg SM, Raffeld M, Gutierrez M, Chabner BA,
Staudt L, et al: Phase II study of dose-adjusted EPOCH and
rituximab in untreated diffuse large B-cell lymphoma with analysis
of germinal center and post-germinal center biomarkers. J Clin
Oncol. 26:2717–2724. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gisselbrecht C, Glass B, Mounier N, Gill D
Singh, Linch DC, Trneny M, Bosly A, Ketterer N, Shpilberg O,
Hagberg H, et al: Salvage regimens with autologous transplantation
for relapsed large B-cell lymphoma in the rituximab era. J Clin
Oncol. 28:4184–4190. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fu K, Weisenburger DD, Choi WW, Perry KD,
Smith LM, Shi X, Hans CP, Greiner TC, Bierman PJ, Bociek RG, et al:
Addition of rituximab to standard chemotherapy improves the
survival of both the germinal center b-cell-like and non-germinal
center b-cell-like subtypes of diffuse large b-cell lymphoma. J
Clin Oncol. 26:4587–4594. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Larouche JF, Berger F, Chassagne-Clément
C, Ffrench M, Callet-Bauchu E, Sebban C, Ghesquières H,
Broussais-Guillaumot F, Salles G and Coiffier B: Lymphoma
recurrence 5 years or later following diffuse large B-cell
lymphoma: Clinical characteristics and outcome. J Clin Oncol.
28:2094–2100. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fang C, Xu W and Li JY: A systematic
review and meta-analysis of rituximab-based immunotherapy for
subtypes of diffuse large B cell lymphoma. Ann Hematol.
89:1107–1113. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hui D, Proctor B, Donaldson J, Shenkier T,
Hoskins P, Klasa R, Savage K, Chhanabhai M, Gascoyne RD, Connors JM
and Sehn LH: Prognostic implications of extranodal involvement in
patients with diffuse large B-cell lymphoma treated with rituximab
and cyclophosphamide, doxorubicin, vincristine, and prednisone.
Leuk Lymphoma. 51:1658–1667. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pfreundschuh M, Trümper L, Kloess M,
Schmits R, Feller AC, Rübe C, Rudolph C, Reiser M, Hossfeld DK,
Eimermacher H, et al: Two weekly or 3-weekly CHOP chemotherapy with
or without etoposide for the treatment of elderly patients with
aggressive lymphomas: Results of the NHL-B2 trial of the DSHNHL.
Blood. 104:634–641. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cunningham D, Hawkes EA, Jack A, Qian W,
Smith P, Mouncey P, Pocock C, Ardeshna KM, Radford JA, McMillan A,
et al: Rituximab plus cyclophosphamide, doxorubicin, vincristine,
and prednisolone in patients with newly diagnosed diffuse large
B-cell non-Hodgkin lymphoma: A phase 3 comparison of dose
intensification with 14-day versus 21-day cycles. Lancet.
381:1817–1826. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Delarue R, Tilly H, Mounier N, Petrella T,
Salles G, Thieblemont C, Bologna S, Ghesquières H, Hacini M,
Fruchart C, et al: Dose-dense rituximab-CHOP compared with standard
rituximab-CHOP in elderly patients with diffuse large B-cell
lymphoma (the LNH03-6B study): A randomised phase 3 trial. Lancet
Oncol. 14:525–533. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Morschhauser F, Radford J, Van Hoof A,
Vitolo U, Soubeyran P, Tilly H, Huijgens PC, Kolstad A, d'Amore F,
Diaz M Gonzalez, et al: Phase III trial of consolidation therapy
with yttrium-90-ibritumomab tiuxetan compared with no additional
therapy after first remission in advanced follicular lymphoma. J
Clin Oncol. 26:5156–5164. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Witzig TE, Gordon LI, Cabanillas F,
Czuczman MS, Emmanouilides C, Joyce R, Pohlman BL, Bartlett NL,
Wiseman GA, Padre N, et al: Randomized controlled trial of
yttrium-90-labeled ibritumomab tiuxetan radioimmunotherapy versus
rituximab immunotherapy for patients with relapsed or refractory
low-grade, follicular, or transformed B-cell non-Hodgkin's
lymphoma. J Clin Oncol. 20:2453–2463. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Morschhauser F, Illidge T, Huglo D,
Martinelli G, Paganelli G, Zinzani PL, Rule S, Liberati AM, Milpied
N, Hess G, et al: Efficacy and safety of yttrium-90 ibritumomab
tiuxetan in patients with relapsed or refractory diffuse large
B-cell lymphoma not appropriate for autologous stem-cell
transplantation. Blood. 110:54–58. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Witzig TE, Molina A, Gordon LI,
Emmanouilides C, Schilder RJ, Flinn IW, Darif M, Macklis R, Vo K
and Wiseman GA: Long-term responses in patients with recurring or
refractory B-cell non-Hodgkin lymphoma treated with yttrium 90
ibritumomab tiuxetan. Cancer. 109:1804–1810. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zinzani PL, Tani M, Fanti S, Stefoni V,
Musuraca G, Castellucci P, Marchi E, Farsad M, Fina M, Pellegrini
C, et al: A phase II trial of CHOP chemotherapy followed by yttrium
90 ibritumomab tiuxetan (Zevalin) for previously untreated elderly
diffuse large B-cell lymphoma patients. Ann Oncol. 19:769–773.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zinzani PL, Rossi G, Franceschetti S,
Botto B, Di Rocco A, Cabras MG, Petti MC, Stefoni V, Broccoli A,
Fanti S, et al: Phase II trial of short-course R-CHOP followed by
90Y-ibritumomab tiuxetan in previously untreated high-risk elderly
diffuse large B-cell lymphoma patients. Clin Cancer Res.
16:3998–4004. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cheson BD, Horning SJ, Coiffier B, Shipp
MA, Fisher RI, Connors JM, Lister TA, Vose J, Grillo-López A,
Hagenbeek A, et al: Report of an international workshop to
standardize response criteria for non-Hodgkin's lymphomas. NCI
Sponsored International Working Group. J Clin Oncol. 17:12441999.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hans CP, Weisenburger DD, Greiner TC,
Gascoyne RD, Delabie J, Ott G, Müller-Hermelink HK, Campo E,
Braziel RM, Jaffe ES, et al: Confirmation of the molecular
classification of diffuse large B-cell lymphoma by
immunohistochemistry using a tissue microarray. Blood. 103:275–282.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Simon R: Optimal two-stage designs for
phase II clinical trials. Control Clin Trials. 10:1–10. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kalbfleisch JD and Prentice RL: The
Statistical Analysis of Failure Time Data. New York: John Wiley
& Sons, Inc., 1980. Canadian Journal of Statistics. 10:64–66.
1982. View
Article : Google Scholar
|
|
23
|
Sehn LH, Berry B, Chhanabhai M, Fitzgerald
C, Gill K, Hoskins P, Klasa R, Savage KJ, Shenkier T, Sutherland J,
et al: The revised International Prognostic Index (R-IPI) is a
better predictor of outcome than the standard IPI for patients with
diffuse large B-cell lymphoma treated with R-CHOP. Blood.
109:1857–1861. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Feugier P, Van Hoof A, Sebban C,
Solal-Celigny P, Bouabdallah R, Fermé C, Christian B, Lepage E,
Tilly H, Morschhauser F, et al: Long-term results of the R-CHOP
study in the treatment of elderly patients with diffuse large
B-cell lymphoma: A study by the Groupe d'Etude des Lymphomes de
l'Adulte. J Clin Oncol. 23:4117–4126. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pfreundschuh M, Schubert J, Ziepert M,
Schmits R, Mohren M, Lengfelder E, Reiser M, Nickenig C, Clemens M,
Peter N, et al: Six versus eight cycles of bi-weekly CHOP-14 with
or without rituximab in elderly patients with aggressive CD20+
B-cell lymphomas: A randomized controlled trial (RICOVER-60).
Lancet Oncol. 9:105–116. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Récher C, Coiffier B, Haioun C, Molina TJ,
Fermé C, Casasnovas O, Thiéblemont C, Bosly A, Laurent G,
Morschhauser F, et al: Intensified chemotherapy with ACVBP plus
rituximab versus standard CHOP plus rituximab for the treatment of
diffuse large B-cell lymphoma (LNH03-2B): An open-label randomised
phase 3 trial. Lancet. 378:1858–1867. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Stiff PJ, Unger JM, Cook JR, Constine LS,
Couban S, Stewart DA, Shea TC, Porcu P, Winter JN, Kahl BS, et al:
Autologous transplantation as consolidation for aggressive
non-hodgkin's lymphoma. N Engl J Med. 369:1681–1690. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hamlin P, Rodriguez MA, Noy A, Portlock
CS, Straus D, McLaughlin P, Pro P, Fayad L, Hagemeister F, Wegner
B, et al: Final Results of a Phase II Study of Sequential R-CHOP
and Yttrium-90 Ibritumomab Tiuxetan (RIT) For Elderly High Risk
Patients with Untreated Diffuse Large B-Cell Lymphoma (DLBCL).
Blood. 116:17932010.
|
|
29
|
Yang DH, Kim WS, Suh C, Kwak JY, Jung JS,
Kim SH, Kim JS, Lee JJ and Kim HJ: Phase II trial of
90Y-ibritumomab tiuxetan treatment as consolidation after 6th
R-CHOP chemotherapy in patients with limited-stage, bulky diffuse
large B-cell lymphoma. Blood. 114:37512009.
|
|
30
|
Kraeber-Bodere F, Maisonneuve H, Lamy T,
Gouill SL, Deconninck E, Pallardy A, bodet-Milin C, Milpied N,
Morineau N, Foussard C, et al: Consolidation anti-CD22 fractionated
radioimmunotherapy with 90Y epratuzumab tetraxetan following R-CHOP
in elderly DLBCL patients. Blood. 116:28752010.PubMed/NCBI
|
|
31
|
Friedberg JS, Unger JM, Burack WR, et al:
R-CHOP with iodine-131 tositumomab consolidation for advanced stage
diffuse large B-cell lymphoma (DLBCL): SWOG S0433. Br J Haematol.
116:382–389. 2014. View Article : Google Scholar
|
|
32
|
Larouche JF, Berger F, Chassagne-Clément
C, Ffrench M, Callet-Bauchu E, Sebban C, Ghesquières H,
Broussais-Guillaumot F, Salles G and Coiffier B: Lymphoma
recurrence 5 years or later following diffuse large B-cell
lymphoma: Clinical characteristics and outcome. J Clin Oncol.
28:2094–2100. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Nowakowski GS, LaPlant B, Macon WR, Reeder
CB, Foran JM, Nelson GD, Thompson CA, Rivera CE, Inwards DJ,
Micallef IN, et al: Lenalidomide combined with R-CHOP overcomes
negative prognostic impact of non-germinal center B-cell phenotype
in newly diagnosed diffuse large B-cell lymphoma: A phase II study.
J Clin Oncol. 33:251–257. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Younes A, Thieblemont C, Morschhauser F,
Flinn I, Friedberg JW, Amorim S, Hivert B, Westin J, Vermeulen J,
Bandyopadhyay N, et al: Combination of ibrutinib with rituximab,
cyclophosphamide, doxorubicin, vincristine and prednisone (R-CHOP)
for treatment-naive patients with CD20-positive B-cell non-Hodgkin
lymphoma: A non-randomised, phase 1b study. Lancet Oncol.
15:1019–1026. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Czuczman MS, Emmanouilides C, Darif M,
Witzig TE, Gordon LI, Revell S, Vo K and Molina A:
Treatment-related myelodysplastic syndrome and acute myelogenous
leukemia in patients treated with ibritumomab tiuxetan
radioimmunotherapy. J Clin Oncol. 25:4285–4292. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Boehme V, Schmitz N, Zeynalova S, Loeffler
M and Pfreundschuh M: CNS events in elderly patients with
aggressive lymphoma treated with modern chemotherapy (CHOP-14) with
or without rituximab: An analysis of patients treated in the
RICOVER-60 trial of the German High-Grade Non-Hodgkin Lymphoma
Study Group (DSHNHL). Blood. 113:3896–3902. 2009. View Article : Google Scholar : PubMed/NCBI
|