Introduction
Simple renal cysts are the most common renal masses
in the urinary tract. The majority of these cysts are benign,
asymptomatic, and are usually treated conservatively. The major
clinical concern is distinguishing simple renal cysts from complex
cysts that may harbor malignancy. Recent advances in radiology have
improved the clinical approach to asymptomatic renal masses,
including benign cysts and renal cell carcinoma (RCC), by
ultrasound (US), computed tomography (CT) or magnetic resonance
imaging. Clinically, the classification of renal cystic tumors is
based on the Bosniak classification system (1,2). In
Bosniak category I, the incidence of malignancy is very low. In
categories II and III, a certain extent of malignant cystic disease
is included and adequate treatment may be required. Renal cysts
with thickened, irregular or smooth walls or septa and enhancement
following contrast injection, favor malignancy.
Case reports of RCCs presenting as simple cysts are
extremely rare. It is difficult to determine preoperatively whether
or not a cyst is malignant. Although cytology and serum tumor
markers have also been investigated, their diagnostic value is
limited to cases of renal malignancy (3). We herein describe the case of a patient
with transformation of a simple renal cyst to RCC.
Case report
A 39-year-old female patient with left flank pain
for 3 months was referred to the Sir Run-Run Shaw Hospital
(Hangzhou, China). The patient had no underlying predisposing
conditions or syndromes, such as a history of trauma, chronic renal
disease, or tuberous sclerosis. There was also no family history of
renal cysts, RCC, or renal malformations. The results of the
laboratory investigations were normal. US examination revealed a
70×60-mm cyst in the upper pole of the left kidney and an abdominal
contrast-enhanced CT scan showed a simple cyst in the lateral
aspect of the left kidney (Fig. 1).
The density of the cyst contents was similar to that of water and
there was no enhancement. The patient underwent laparoscopic
decortication of the cyst. Under laparoscopic visualization, the
cystic fluid was aspirated by a syringe and immediately sent for
biochemical analysis. The cystic fluid was clear and yellow, and
the biochemical analysis showed that the aspirated fluid contained
extremely low levels of potassium, sodium, calcium and glucose
(Table I). This was quite different
from the contents of regular cysts, which usually have a
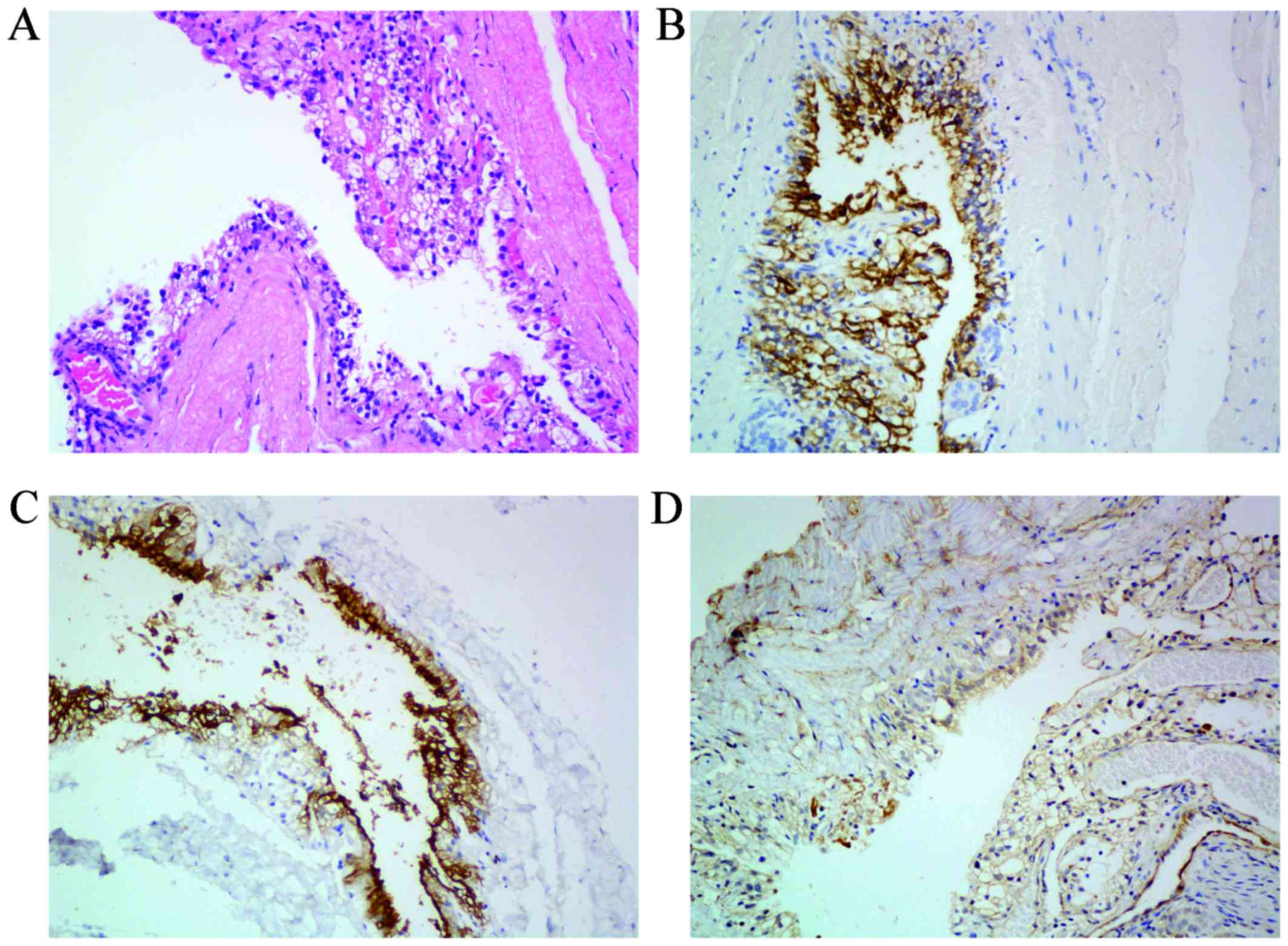
consistency similar to that of serum. The cyst wall was excised and
sent for pathological evaluation and the histological examination
of the floor of the cyst indicated malignancy. Macroscopically, the
external surface of the cyst was smooth, but small excrescences
were observed in the inner wall of the cyst. On immunostaining, the
tumor cells stained positive for RCC marker, CD10 and vimentin, and
negative for cytokeratin 7 (Fig. 2).
Laparoscopic nephrectomy was performed 20 days after decortication
and the pathological examination confirmed the diagnosis of RCC of
the clear cell type. The postoperative course was uneventful. The
patient was followed up by chest X-ray, liver function tests,
abdominal CT scans and physical examination every 3 months for the
first year and every 6 months thereafter. There has been no
evidence of local recurrence or metastatic disease to date.
 | Table I.Biochemical analysis of the cystic
fluid. |
Table I.
Biochemical analysis of the cystic
fluid.
| Potassium
(mmol/l) | Sodium (mmol/l) | Chlorine
(mmol/l) | Calcium (mmol/l) | Blood urea nitrogen
(mmol/l) | Creatinine
(µmol/l) | Glucose (mmol/l) |
|---|
| <1.00 | <100 | <50 | 0.87 | 2.40 | 22 | 1.94 |
Discussion
RCC presenting as a simple renal cyst is extremely
rare and only few cases have been reported to date in the English
literature. Lin et al (4)
reported a patient with flank pain who was initially diagnosed with
a simple cyst and was treated by ultrasound-guided aspiration, but
the pain developed again 3 weeks later and ultrasound examination
indicated a recurrent sizeable cyst. Nephrectomy was then performed
and pathological examination confirmed the diagnosis of papillary
RCC. Visapää et al (5)
evaluated 482 patients who underwent partial or radical nephrectomy
for kidney tumors and demonstrated an association between simple
renal cysts and papillary RCC. Sakai et al (6) reported the case of a simple renal cyst
that developed into a septated renal cyst and finally, to cystic
RCC of the clear cell type, over a period of 6 years. That case
demonstrated the natural history of malignant transformation from a
simple renal cyst, and emphasized that careful follow-up of renal
cysts, particularly of complicated cysts, is mandatory for
successful treatment of RCC. Furthermore, in the Japanese
literature, Takao et al (7)
also reported a cystic RCC diagnosed as a simple cyst
preoperatively.
Diagnosing a simple renal cyst is generally not
difficult. The Bosniak classification system has been accepted as a
method for diagnosing and determining the management of cystic
renal masses, which was designed to analyze the morphology of
cystic masses based solely on CT findings. However, it is difficult
to determine preoperatively whether or not a cyst is malignant. Our
patient, who initially presented with a simple cyst on CT imaging,
apparently classified as Bosniak category I, was pathologically
diagnosed with RCC. This may be due to the small size of the
malignant tissue inside the cyst, which cannot be detected by
imaging examinations alone.
The management options for renal cysts include
radiological surveillance, ultrasound- or CT-guided cyst aspiration
or biopsy and laparoscopic exploration or open surgical
exploration, with or without radical or partial nephrectomy. Cyst
aspiration for cytology may be helpful in the management of a
patient only if malignant cells are clearly seen. Radical or
partial nephrectomy may result in overtreatment, as nephrectomies
often prove unnecessary. Omachi et al (8) reviewed the characteristics of
intracystic fluid associated with RCC from the Japanese literature
and found that cytological examination was negative for tumor cells
in the majority of these cases, and 70% was hemorrhagic intracystic
fluid. CT-guided biopsy may also be difficult and occasionally
leads to misdiagnosis (9,10).
In the present case, the renal lesion was found to
be a simple cyst on ultrasound and CT examination, classified as
Bosniak category I. The possibility of malignancy appeared to be
extremely low, but finally pathology demonstrated RCC.
Interestingly, the biochemical analysis of the aspiration fluid
revealed that it contained low levels of potassium, sodium, calcium
and glucose, which is unusual in a simple renal cyst. In the case
reported by Lin et al (4) the
cystic RCC also had low glucose (0.333 mmol/l), and increased
lactate dehydrogenase (2,361 U/l) levels. In our institute, the
cystic fluid is routinely tested in all patients who undergo
laparoscopic decortication, in order to detect whether the cyst
communicates with the renal pelvis, and we observed that the
consistency of the contents of simple renal cysts is almost the
same as that of the serum (data not shown). The change of
biochemical consistency and protein levels may be associated with
the microenvironment changes in malignancy.
Therefore, it is crucial that we recognize the
possibility of RCC appearing as a simple renal cyst. Biochemical
analysis of the cystic fluid may help identify the presence
malignancy and we recommend that biochemical analysis of the cystic
fluid be routinely performed, either by ultrasound- or CT-guided
cyst aspiration or during laparoscopic procedures. If suspicious,
achieving a rapid pathological diagnosis by biopsy of the cyst wall
is necessary. If the presence of malignancy is pathologically
confirmed, an immediate partial or radical nephrectomy may be
performed under the same anesthetic as the laparoscopic
procedure.
References
|
1
|
Bosniak MA: The current radiological
approach to renal cysts. Radiology. 158:1–10. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Israel GM and Bosniak MA: An update of the
Bosniak renal cyst classification system. Urology. 66:484–488.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Li G, Bilal I, Gentil-Perret A, Feng G,
Zhao A, Peoc'h M, Genin C, Tostain J and Gigante M: CA9 as a
molecular marker for differential diagnosis of cystic renal tumors.
Urol Oncol. 30:463–468. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lin CJ, Chen YC, Chen HH, Wu CJ and Hsu
JM: Renal cell carcinoma presenting as a huge simple renal cyst.
Med Oncol. 25:104–106. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Visapää H, Glucker E, Haukka J, Taari K
and Nisen H: Papillary renal cell cancer is strongly associated
with simple renal cysts. Urol Int. 91:269–272. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sakai N, Kanda F, Kondo K, Fukuoka H and
Tanaka T: Sonographically detected malignant transformation of a
simple renal cyst. Int J Urol. 8:23–25. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Takao T, Gotoh T, Takada S and Sugao H:
Cystic renal cell carcinoma diagnosed as a simple cyst
preoperatively with incidental renal tumor: A case report.
Hinyokika Kiyo. 45:339–342. 1999.(In Japanese). PubMed/NCBI
|
|
8
|
Omachi T, Sakamoto W, Kishimoto T, Kawano
M, Oyama A, Kamizuru M, Maekawa M, Hagihara S and Nakamura K: A
case of renal cyst associated with renal cell
carcinoma-characteristics of intracystic fluid associated with
renal cell carcinoma from Japanese reports. Hinyokika Kiyo.
38:323–326. 1992.(In Japanese). PubMed/NCBI
|
|
9
|
Siegel CL: Accuracy of diagnosis by guided
biopsy of renal mass lesions classified indeterminate by imaging
studies. J Urol. 165:322–323. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kadekawa K, Miyazato M, Saito S, Morozumi
M, Matsuzaki A, Yoshimi N and Sugaya K: Renal cell carcinoma
originating in a renal cyst in a 12-year-old girl. J Pediatr Surg.
44:e5–e7. 2009. View Article : Google Scholar : PubMed/NCBI
|