Introduction
Cancer is one of the leading causes of mortality
worldwide. In 2012, it was reported that 14 million individuals
suffered from cancer and that 8.2 million patients succumbed to the
disease. The number of patients who succumbed to lung cancer
increased from 1.2 to 1.6 million worldwide between 2000 and 2012
(1). Over the last decade, advances
in combined therapeutic modalities have a granted survival benefit
to patients with lung cancer. However, the survival of patients who
undergo radical surgery for non-small-cell lung cancer (NSCLC) is
unsatisfactory, with a median relapse-free survival (RFS) of 52.8
months and a 5-year RFS rate of 47.3% (2). The main reason for these disappointing
figures is that lung cancer easily develops metastases in distant
organs, such as the adrenal grand, liver, brain and bone. It is
reported that ~60% of patients with NSCLC already have
micro-metastases at initial diagnosis (3), indicating that early detection and
treatment of distant metastases is crucial for improving the
prognosis of lung cancer patients.
The bones are one of the most common metastatic
sites in patients with advanced lung cancer. Previous studies have
reported detection of spinal metastases in ~one-third of autopsied
cancer patients (4), and 60% of
patients with lung cancer have been found to have spinal metastases
(5). Lung cancer (as well as breast
and prostate cancer) is a type of cancer that frequently develops
bone metastases, which cause skeletal-related events (SREs)
including pain, paralysis, pathological fractures and hypercalcemia
(6). These SREs compromise the
patients' quality of life (QoL) and activities of daily living
(ADL), and may deprive them of the opportunity to receive further
anticancer therapy.
Medical treatment of bone metastases includes a
bisphosphonate, zoledronic acid, which delays the onset of SREs. In
addition, denosumab, a human monoclonal antibody against the
receptor activator of nuclear factor κB ligand, was reported to
significantly delay the time to onset of SREs when compared with
zoledronic acid (20.6 vs. 16.3 months, respectively) (7). Surgical treatment for vertebral
metastases often reduces symptoms such as pain and progressive
paralysis, contributing to improvement in the patients' ADL. These
surgical effects may be immediately observed in patients with
vertebral metastases. However, surgical treatment is only
recommended if the patients' expected survival is >3 months
(8).
The Tokuhashi score (9) and the Tomita score (10) are used to predict the prognosis of
patients with bone metastases; based on these scores, the
indications for surgical treatment of bone metastases may be
assessed. The criteria of the Tokuhashi score include general
condition [performance status (PS)], number of extraspinal bone
metastases, number of metastases in the vertebral body, metastases
in major internal organs, site of primary cancer and the extent of
paralysis according to the Frankel grade functional score (11). The criteria of the Tomita score
comprise the aggressiveness of the primary tumor, the presence of
visceral metastases and the number of bone metastases.
In Tokuhashi and Tomita scoring, patients with bone
metastases from advanced NSCLC are allotted a high score due to the
aggressive nature of the NSCLC. Therefore, such patients are
unlikely to be considered as candidates for surgical treatment.
However, given that these scores do not take into consideration the
effect of novel anticancer therapy consisting of molecular-targeted
drugs, it was questioned whether these scores are still suitable
for determining the indications for surgical treatment of bone
metastases in NSCLC. In this study, we examined the clinical
benefit of surgical treatments, including laminectomy and
posterolateral fusion, in patients with vertebral metastases from
NSCLC, and evaluated the discrepancy between clinical outcome and
prognosis as predicted by the Tokuhashi and Tomita scores prior to
surgery.
Patients and methods
Patients
The clinical course of patients who received
surgical treatment for neurological paralysis resulting from
vertebral metastasis of advanced NSCLC at the Shiga University of
Medical Science Hospital (Otsu, Japan) between April, 2007 and
March, 2012 was retrospectively analyzed. All the patients provided
written informed consent prior to surgery, and underwent
laminectomy in combination with posterior spinal fixation surgery.
After the surgical treatment, systemic anticancer therapy for bone
metastasis, consisting of cytotoxic chemotherapeutic agents or
molecular-targeted drugs and radiotherapy, was considered in
patients whose PS and ADL improved.
Tokuhashi and Tomita scores
To predict the prognosis of patients with bone
metastases, the Tokuhashi and Tomita scores were calculated
preoperatively. The Tokuhashi scores range between 0 and 15 and are
based on six criteria: PS (0: PS 3-4; 1: PS 2; and 2: PS 0–1);
number of extraspinal bone metastases (0: n≥3; 1: n=1–2; and 2:
n=0); number of spinal bone metastases (0: n≥3; 1: n=2; and 2:
n=1); primary organ of cancer (0: lung cancer); metastases in major
internal organs (0: unresectable; 1: resectable; and 2: no
metastases); and status of paralysis (0: Frankel A-B; 1: Frankel
C-D; and 2: Frankel E). The prognosis of the patients is estimated
as follows: 0–8, ≤6 months; 9–11, ≥6 months; and 12–15, ≥12 months
(9). The Tomita score ranges from 2
to 10 and includes three criteria: Status of bone metastases (1:
solitary or isolated; 2: multiple); metastases in visceral organs
(2: treatable; 4: untreatable); and primary organ of cancer (4:
lung cancer). The surgical strategy for the patients is recommended
as follows: Score 2–3, wide or marginal excision; 4–5, marginal or
intralesional excision; 6–7, palliative surgery; and 8–10,
supportive care (10).
Statistical analysis
The clinical courses of the patients were obtained
from their clinical records, and the median paralysis-free survival
and overall survival (OS) after the fixation surgery were
calculated according to the Kaplan-Meier method using SPSS 22.0
software (IBM, Armonk, NY, USA).
Results
Patient characteristics
Four patients with SREs attributable to advanced
NSCLC were enrolled in this study (Table
I). The patients included 3 men and 1 woman, with a median age
of 56.5 years (range, 41–67 years). The histological type of NSCLC
was adenocarcinoma in all patients, and 2 patients were found to
have pulmonary adenocarcinoma with epidermal growth factor receptor
gene (EGFR) mutation. The median time from the initial diagnosis of
NSCLC to the onset of SREs was 1.5 months (range, 0–38 months). Of
the symptoms commonly associated with SREs, pain, paralysis and
pathological fractures were observed in 3, 4 and 4 patients,
respectively, whereas hypercalcemia was not observed in any of the
patients. By the onset of SREs, 3 patients had been administered
zoledronic acid. The median time from the onset of SREs to fixation
surgery was 22.5 days (range, 10–25 days). The status of paralysis
prior to fixation surgery was considered to be Frankel grade C for
all patients, whereas the Eastern Cooperative Oncology Group PS was
2 in all patients.
 | Table I.Patient characteristics (n=4). |
Table I.
Patient characteristics (n=4).
| Characteristics | N (%) |
|---|
| Median age, years
(range) | 56.5 (41 67) |
| Gender |
|
| Male | 3 (75.0) |
|
Female | 1 (25.0) |
| Histology |
|
|
Adenocarcinoma | 4 (100.0) |
| EGFR status |
|
|
Mutated | 2 (50.0) |
|
Wild-type | 2 (50.0) |
| Symptoms associated
with SREs |
|
| Pain | 3 (75.0) |
|
Paralysis | 4 (100.0) |
|
Pathological fractures | 4 (100.0) |
Tokuhashi and Tomita scores prior to surgical
fixation. The Tokuhashi score prior to surgical fixation was
calculated to be 7 for 1 patient, 8 for 1 patient and 9 for 2
patients, with a median preoperative score of 8.3. The data
suggested a survival prognosis of <6 months in 2 patients and
<12 months in the other 2 patients. As regards the Tomita score
prior to surgical fixation, 2 patients were calculated to have 6
points, indicating that palliative surgery was recommended; the
remaining 2 patients were calculated to have 8 points, which was an
indication for supportive care but not palliative surgery.
Clinical outcome of surgical fixation. All 4
patients underwent laminectomy in combination with posterior spinal
fixation surgery, and experienced no complications associated with
the operation. At a median time of 15 days after fixation surgery,
the Frankel grade was D for 3 patients and E for 1 patient,
demonstrating that the paralysis was improved by the surgery.
Furthermore, the Eastern Cooperative Oncology Group PS of all
patients was 1, demonstrating that the patients' ADL had also
improved postoperatively. After the surgery, all the patients
received several anticancer therapies; systemic chemotherapy was
initiated in all 4 patients, EGFR-tyrosine kinase inhibitor (TKI)
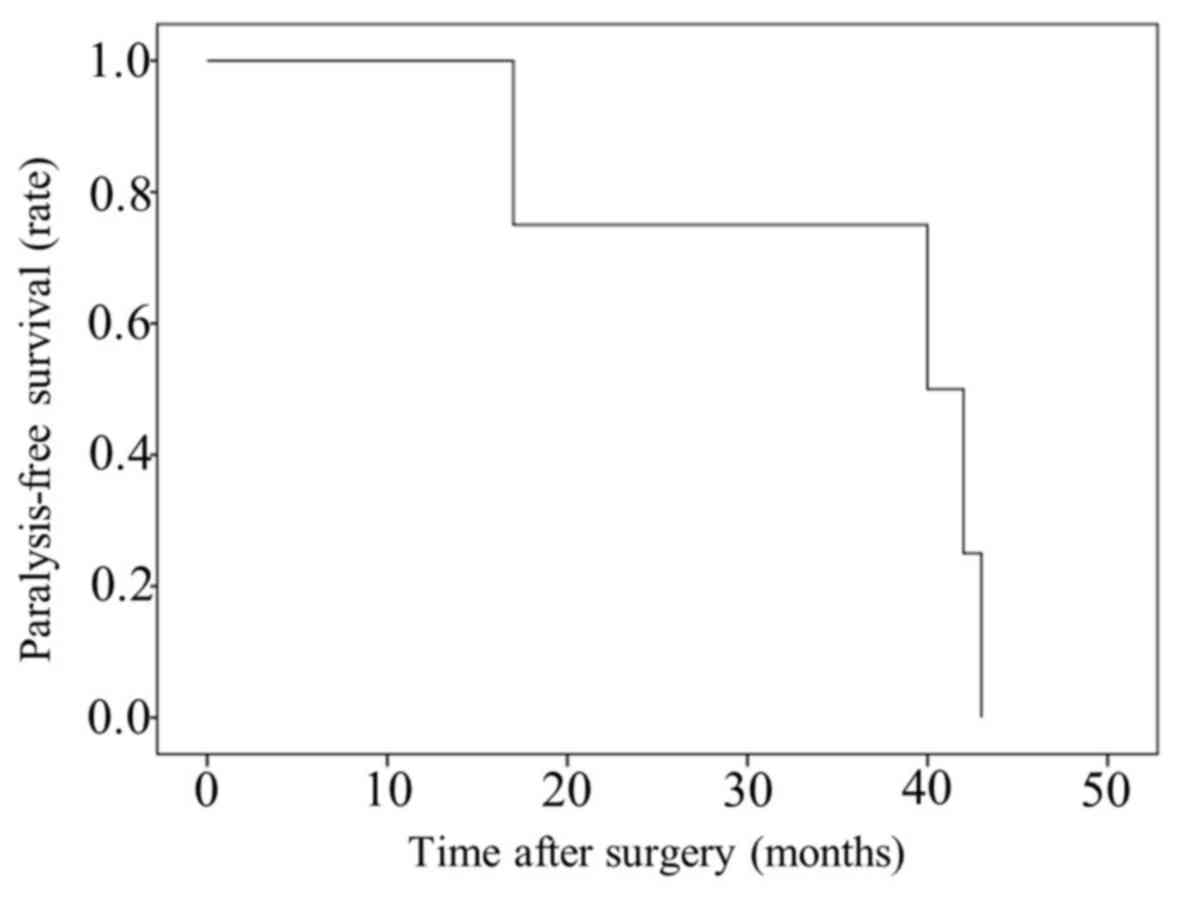
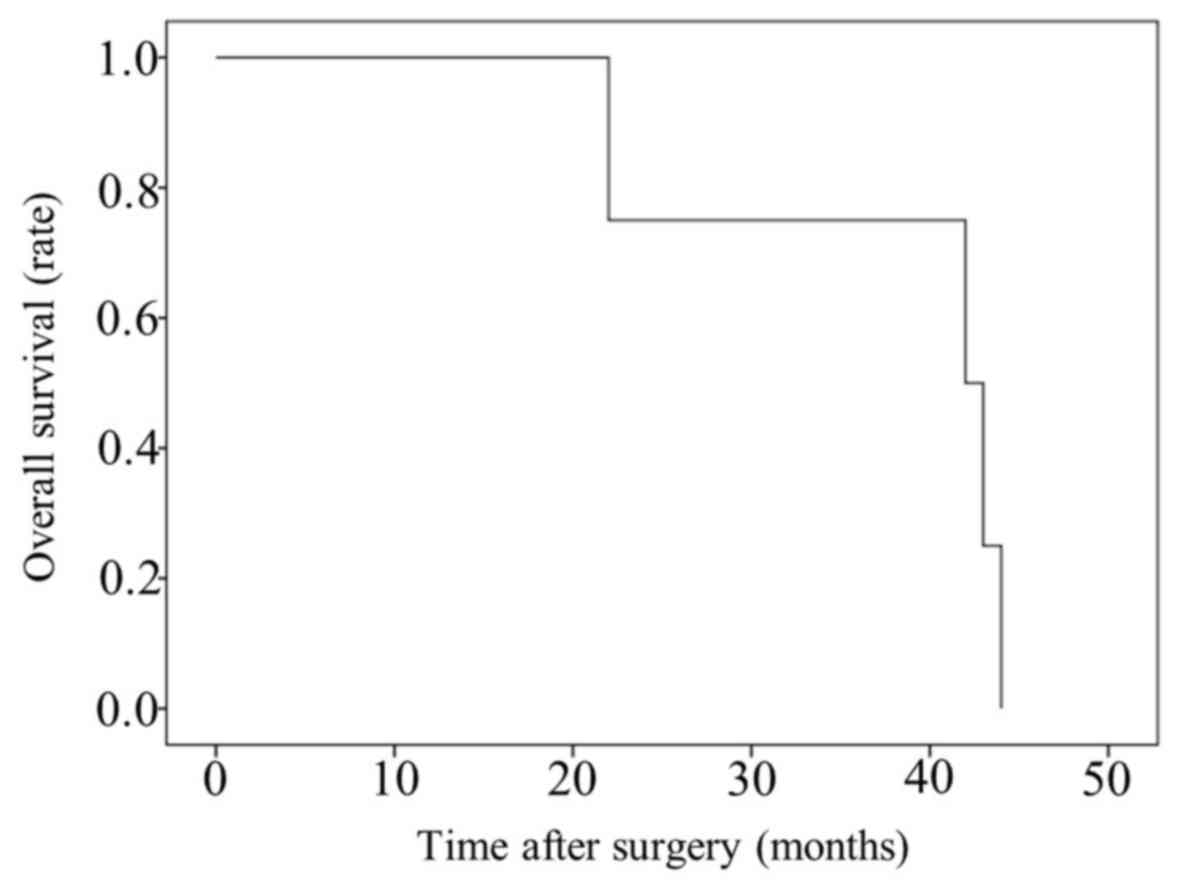
treatment in 4, and radiation therapy in 2 patients. The median
paralysis-free time following fixation surgery was 41.0 months
(range, 17–43 months; Fig. 1), and
the median OS postoperatively was 42.5 months (range, 22–44 months;
Fig. 2, Table II).
| Table II.Clinical outcomes. |
Table II.
Clinical outcomes.
| Variables | Case 1 | Case 2 | Case 3 | Case 4 |
|---|
| Regions of vertebral
metastases | C5-Th2 | Th4–10 | Th4–10 | C5-Th6 |
| Preoperative
Tokuhashi score | 9 | 8 | 7 | 9 |
| Preoperative Tomita
score | 8 | 6 | 8 | 6 |
| Frankel grade
(before→after surgery) | C→D | C→D | C→D | C→E |
| ECOG PS (before→after
surgery) | 2→1 | 2→1 | 2→1 | 2→1 |
| Postoperative
therapy | Chemotherapy | Chemotherapy | Chemotherapy | Chemotherapy |
|
| EGFR-TKI | EGFR-TKI | Radiation | EGFR-TKI |
|
| Radiation | Bisphosphonate | Bisphosphonate | Bisphosphonate |
| Predicted prognosis
by Tokuhashi score (months) | <12 | <6 | <6 | <12 |
| Postoperative
paralysis-free period (months) | 17 | 43 | 40 | 42 |
| Postoperative
survival time (months) | 22 | 44 | 40 | 43 |
Discussion
In the present study, the clinical benefit of
surgical treatment in patients with vertebral metastases arising
from advanced NSCLC was reported. At the onset of SREs, these
patients were predicted to have a poor prognosis as estimated
according to the Tokuhashi score. However, surgical fixation
improved the patients' ADL and enabled them to receive anticancer
therapy, contributing to prolonged survival.
It has been reported that bone metastasis develops
in 30–60% of patients with advanced lung cancer. The most frequent
site of bone metastasis are the vertebrae (12), comprising >50% of all bone
metastases from lung cancer (13).
Bone metastasis may cause SREs such as intolerable pain,
pathological fractures and paralysis, leading to deterioration of
the patients' ADL, PS and QoL. Patients with SREs appear to miss
the opportunity to receive active anticancer therapy due to their
SRE-related deteriorating status. Thus, surgical intervention for
SREs may improve the patients' condition and, subsequently, their
ADL and QoL.
In this study, the clinical benefit of surgical
treatments, including laminectomy and posterolateral fusion, was
evaluated in patients with vertebral metastases from advanced
NSCLC. The median OS of our patients following fixation surgery was
42.5 months. Taking into consideration the previously reported OS
of 13.4 months for patients with bone metastases from lung cancer
(14), our patients achieved a
significantly prolonged survival. The surgical treatment for SREs
contributed to the improvement of their PS and enabled them to
receive subsequent anticancer (but not palliative) therapy, such as
molecular-targeted therapy (EGFR-TKIs) and cytotoxic chemotherapy.
It has been reported that EGFR-TKIs may prolong the OS of patients
with EGFR-mutated NSCLC to 21.6–30.9 months (15–17).
Surgical treatment of vertebral metastases from lung cancer
provides the patient with the further opportunity to receive active
molecular-targeted therapy or chemotherapy, thus contributing to
the prolongation of OS.
To aid the decision-making process for the surgical
treatment of bone metastases, the Tokuhashi score has been used to
predict the prognosis of cancer patients (9). In this report, the suitability of this
scoring system was evaluated in cases with advanced NSCLC with
vertebral metastases. According to the Tokuhashi score, the
survival prognosis of patients in the study was predicted to be
<6 months for 2 patients and 6–12 months for the other 2
patients; however, their OS was in fact significantly longer
compared with that predicted by the Tokuhashi score prior to
surgery.
The reason why the predicted prognosis was poorer
compared with the actual OS is associated with a specific criterion
of the Tokuhashi score. The primary site of cancer, i.e.,
aggressiveness of cancer growth, is reflected in the score. Given
that lung cancer is particularly aggressive, a lung cancer patient
is given a low Tokuhashi score. Thus, based on this score the
predicted survival of patients with NSCLC is estimated to be up to
12 months, which is consistent with the data of patients with bone
metastases from lung cancer, reporting an OS of ≤6 months (12,18).
However, the OS was recently reported to be prolonged up to 13.4
months (14) by the administration
of EGFR-TKIs and newly developed chemotherapies.
In this context, the Tokuhashi score at present is
likely unsuitable for the prediction of prognosis in patients with
lung cancer and requires a revision. Hessler et al compared
the predicted and achieved OS in 76 patients with vertebral
metastases from lung cancer, reporting that they were similar in 51
of the 76 cases (67.1%) and unequal in 25 of the 76 cases (32.9%);
they concluded that the Tokuhashi score was a suboptimal tool for
the prediction of prognosis in patients with bone metastases from
lung cancer (19). Given that their
data were collected between 1999 and 2004, it is highly likely the
patients in their study were not treated with EGFR-TKIs. We
consider that a specific prognostic score for evaluating the
prognosis of patients with bone metastases from NSCLC should be
developed, including the criteria of genetic and histological types
of lung cancer.
The Tomita score is also a decision-making tool with
regard to surgical treatment for bone metastasis (10) when selecting a suitable treatment
strategy. We evaluated whether the Tomita score would be applicable
in cases of lung cancer with vertebral metastases. According to
this scoring system, 2 of the 4 patients in the study were
recommended to receive supportive care, but not palliative surgery.
In fact, all our patients received palliative surgery, achieving a
median OS after surgical fixation of 42.5 months. Both the Tomita
and Tokuhashi scores are influenced by the primary organ of cancer.
Therefore, the Tomita score generally recommends that patients with
NSCLC who have metastases in the bone as well as other organs
should receive supportive care. However, if the clinical condition
of the patients is improved by palliative surgery, they are given
the opportunity to receive active anticancer therapy. Aoude et
al reported that surgical treatment for vertebral metastases of
lung cancer was decided upon when the Tomita score was 5 (20). However, in patients with lung
adenocarcinoma with EGFR mutation, the prognosis may improve by
administration of EGFR-TKIs.
In conclusion, surgical treatment, including
fixation surgery, may be beneficial for a proportion of patients
with neurological paralysis caused by vertebral metastasis of
advanced NSCLC. A specific score suggesting the appropriate
treatment for patients with bone metastases from advanced NSCLC
should be developed, incorporating criteria in relation to the
genetic and histological types of lung cancer.
References
|
1
|
Stewart BW and Wild CP: World Cancer
Report. IARC; Lyon: 2014
|
|
2
|
Silvestri GA, Tanoue LT, Margolis ML,
Barker J and Detterbeck F: American College of Chest Physicians:
The noninvasive staging of non-small cell lung cancer: The
guidelines. Chest. 123:(Suppl). 147S–156S. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Peters S, Weder W, Dafni U, Kerr KM,
Bubendorf L, Meldgaard P, O'Byrne KJ, Wrona A, Vansteenkiste J,
Felip E, et al: ETOP Lungscape Investigators: Lungscape: Resected
non-small-cell lung cancer outcome by clinical and pathological
parameters. J Thorac Oncol. 9:1675–1684. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wong DA, Fornasier VL and MacNab I: Spinal
metastases: The obvious, the occult, and the impostors. Spine.
15:1–4. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Weigel B, Maghsudi M, Neumann C,
Kretschmer R, Müller FJ and Nerlich M: Surgical management of
symptomatic spinal metastases. Postoperative outcome and quality of
life. Spine. 24:2240–2246. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Schaberg J and Gainor BJ: A profile of
metastatic carcinoma of the spine. Spine. 10:19–20. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Henry DH, Costa L, Goldwasser F, Hirsh V,
Hungria V, Prausova J, Scagliotti GV, Sleeboom H, Spencer A,
Vadhan-Raj S, et al: Randomized, double-blind study of denosumab
versus zoledronic acid in the treatment of bone metastases in
patients with advanced cancer (excluding breast and prostate
cancer) or multiple myeloma. J Clin Oncol. 29:1125–1132. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Walker MP, Yaszemski MJ, Kim CW, Talac R
and Currier BL: Metastatic disease of the spine: Evaluation and
treatment. Clin Orthop Relat Res. 415:(Suppl). S165–S175. 2003.
View Article : Google Scholar
|
|
9
|
Tokuhashi Y, Matsuzaki H, Toriyama S,
Kawano H and Ohsaka S: Scoring system for the preoperative
evaluation of metastatic spine tumor prognosis. Spine.
15:1110–1113. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tomita K, Kawahara N, Kobayashi T, Yoshida
A, Murakami H and Akamaru T: Surgical strategy for spinal
metastases. Spine. 26:298–306. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Frankel HL, Hancock DO, Hyslop G, Melzak
J, Michaelis LS, Ungar GH, Vernon JD and Walsh JJ: The value of
postural reduction in the initial management of closed injuries of
the spine with paraplegia and tetraplegia. I. Paraplegia.
7:179–192. 1969. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Coleman RE: Clinical features of
metastatic bone disease and risk of skeletal morbidity. Clin Cancer
Res. 12:6243s–6249s. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tsuya A, Kurata T, Tamura K and Fukuoka M:
Skeletal metastases in non-small cell lung cancer: A retrospective
study. Lung Cancer. 57:229–232. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Deberne M, Ropert S, Billemont B, Daniel
C, Chapron J and Goldwasser F: Inaugural bone metastases in
non-small cell lung cancer: A specific prognostic entity? BMC
Cancer. 14:4162014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mok TS, Wu YL, Thongprasert S, Yang CH,
Chu DT, Saijo N, Sunpaweravong P, Han B, Margono B, Ichinose Y, et
al: Gefitinib or carboplatin-paclitaxel in pulmonary
adenocarcinoma. N Engl J Med. 361:947–957. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mitsudomi T, Morita S, Yatabe Y, Negoro S,
Okamoto I, Tsurutani J, Seto T, Satouchi M, Tada H, Hirashima T, et
al: West Japan Oncology Group: Gefitinib versus cisplatin plus
docetaxel in patients with non-small-cell lung cancer harbouring
mutations of the epidermal growth factor receptor (WJTOG3405): An
open label, randomised phase 3 trial. Lancet Oncol. 11:121–128.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Maemondo M, Inoue A, Kobayashi K, Sugawara
S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I,
et al: North-East Japan Study Group: Gefitinib or chemotherapy for
non-small-cell lung cancer with mutated EGFR. N Engl J Med.
362:2380–2388. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Decroisette C, Monnet I, Berard H, Quere
G, Le Caer H, Bota S, Audigier-Valette C, Geriniere L, Vernejoux JM
and Chouaid C: Groupe Français de Pneumo-Cancérologie 0601 Team:
Epidemiology and treatment costs of bone metastases from lung
cancer: A French prospective, observational, multicenter study
(GFPC 0601). J Thorac Oncol. 6:576–582. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hessler C, Vettorazzi E, Madert J,
Bokemeyer C and Panse J: Actual and predicted survival time of
patients with spinal metastases of lung cancer: Evaluation of the
robustness of the Tokuhashi score. Spine. 36:983–989. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Aoude AA and Amiot LP: Surgical treatment
of a patient with lung cancer metastasized to the spine with EGFR
mutation: A case report. Int J Surg Case Rep. 3:510–512. 2012.
View Article : Google Scholar : PubMed/NCBI
|