Introduction
Malignant ascites (MA) is a common clinical
manifestation of advanced-stage abdominal cancer. Peritoneal
carcinomatosis (PC) is the cause of >50% of the cases of MA
(PCMA). In >50% of PC patients, MA is the first clinical symptom
of the disease (1). The appearance
of MA indicates an unfavorable prognosis, with an expected median
survival time of ~20 weeks from the time of diagnosis (2). Reduction of MA may improve the quality
of life (QoL) of the patients, create conditions for further
anticancer treatments and prolong survival.
As the existing conservative treatment of PCMA is
mainly based on different forms of chemotherapy with its inherent
toxicity, there is a strong demand for a safe and non-toxic method
for the treatment of this condition. The objective of the present
trial was to develop such an alternative for conventional
chemotherapy-based treatments of PCMA.
In addition to conventional cancer treatments,
hyperthermia (HT) is the most widely investigated complementary
cancer treatment modality for the conservative treatment of PCMA in
combination with chemotherapy (Table
I). However, although temperature-based HT has a long history
of application in oncology, its efficacy and safety remain unproven
(3,4)
and it is currently considered as experimental treatment (5).
 | Table I.Clinical trials on combination of
hyperthermia and chemotherapy for malignant ascites. |
Table I.
Clinical trials on combination of
hyperthermia and chemotherapy for malignant ascites.
| Author (year) | No of patients
(SG/CG) | Study type | Study
treatment | Control
treatment | ORR | Other | Refs. |
|---|
| Li et al
(2010) | 44 (22/22) | Controlled,
double-arm | High-frequency
HT | HIPEC: CDDP 80
mg/m2 in 1l saline + 5FU 500 mg/m2 in 1l
saline | 72.7 vs. 45.5%
31.8% (P<0.05) | KPS IR 54.5% vs.
(P<0.05) | (37) |
| Yu et al
(2007) | 50 (22/28) | Controlled,
double-arm | Microwave whole
body HT 41–42°C 1–2 h | IPCI: CDDP (40–60
mg/m2) + 5FU (500–750 mg/m2) + elemene
(0.2–0.3 g) + IL-2 (2×106 U) | 77.3 vs. 46.4%
(P<0.05) | MST 32 vs. 28
weeks | (38) |
| Yin et al
(2007) | 47 (23/24) | RCT | High-frequency HT
60 min 2/week for 2 weeks | IPCI: CDDP 60
mg/m2 in 60 ml saline + 5FU 500 mg/m2 in 100
ml saline | 65.2 vs. 45.8%
(P<0.05) | KPS IR 47.8% vs.
33.3% (P<0.05) | (39) |
| Wang et al
(2015) | 68 (34/34) | RCT | Radiofrequency
HT | IPCI: CDDP 60
mg/m2 2/week for 3 weeks, 2 cycles | 70.6 vs. 44.1%
(P<0.05) | Higher KPS IR
(P<0.05) | (40) |
The new technology of modulated electro-HT (mEHT;
Oncothermia™) is drawing increasing attention due to its minimal
side effects and synergy with other treatments (6). mEHT is based on the nano-thermal but
not temperature-dependent effects of electromagnetic fields and
special modulation (7), whose effect
may exceed the effect of the overall heating (macroscopic
temperature elevation) by 3–4-fold (8). mEHT does not require hyperthermia-range
temperature and may be performed safely, without invasive thermal
control. Unlike conventional hyperthermia, mEHT is also effective
as monotherapy (7,9). Our previous phase II randomized trial
on the combination of mEHT with traditional Chinese medicine (TCM)
in colorectal cancer (9) suggested a
synergetic effect of mEHT and TCM and was found to be sufficiently
beneficial in PCMA patients for the present trial to be
initiated.
TCM has a long history of application in patients
with advanced cancer as symptomatic treatment and enhancer of the
general resistance of the organism (10). TCM is holistic medicine, which treats
the body as a whole combined with lifestyle and environmental
factors, describing it in terms of ‘vital energy’, also referred to
as ‘Qi’.
In terms of TCM, MA belongs to the category of ‘Gu
Zhang’ (11), which means tympanites
or distension of the abdomen caused by the accumulation of gas or
fluid (12). The pathogenesis of Gu
Zhang is connected with illness of three organs, namely the liver,
spleen and kidney, which leads to stasis of Qi, blood and water in
the abdomen, leading to abdominal distention and, finally, the
formation of Gu Zhang. The application of TCM effectively relieves
the symptoms and improves the QoL of patients with MA (12) by clearing heat and removing dampness,
purging water, promoting blood flow and relieving blood stasis,
promoting the circulation of Qi and dissipating dampness,
invigorating the spleen and kidney, and dissipating warmth
resolving watery dampness (13).
The number of clinical trials on TCM as co-treatment
for PCMA (Table II) using different
TCM treatments is limited (14–17). The
Shi Pi decoction is considered to be the optimal treatment for Gu
Zhang. This decoction was first described in Ji Sheng Fang
(Life-saving Prescriptions) (18).
This may warm Yang, invigorate the spleen and promote Qi
circulation to induce diuresis. The main effect of the Shi Pi
decoction is treatment of the Foot-Taiyin meridian.
| Table II.Clinical studies on TCM at malignant
ascites. |
Table II.
Clinical studies on TCM at malignant
ascites.
| Study (year) | No. of patients
(SG/CG) | Study type | Disease | TCM | Combined
therapy | Control
treatment | ORR | QoL (KPS IR) | Refs. |
|---|
| Chen (2011) | 120 (60/60) | Controlled,
double-arm | MA and MP | TCM | HF-HT | CTx or immune
therapy | 86.7 vs. 58.3%,
(P<0.05) | 75 vs. 30%
(P<0.05) | (14) |
| Zhou and Zhang
(2010) | 41 | Cohort, single
arm | MA | Wu Ling
decoction | No | No | 70.7% | NA | (15) |
| Huang (2006) | 69 | Controlled,
double-arm | MA | Shen Zhu
decoction | Fever therapy | Diuretics | 82.6%
P<0.05 | 28.57% | (16) |
| Gong (2011) | 30 | Cohort, single
arm | MA and MP | No. 3 readjusted
decoction | MW-HT | No | 83.3% | Improved | (17) |
The optimal or standard treatment is considered as
the control treatment in randomized studies. In clinical practice,
diuretics, abdominal paracentesis and local injection of biological
agents and chemotherapeutic drugs are commonly used to treat PCMA
(19). The standard treatment for
PCMA is currently intraperitoneal chemotherapy applied as
chemoinfusion (IPCI) or chemoperfusion (IPCP). IPCP is usually
performed following cytoreductive peritonectomy (CRPE), whereas
IPCI is mainly a stand-alone conservative procedure. Although
IPCP/CRPE appears to be superior to IPCI, it is a difficult,
high-risk and costly procedure. Furthermore, there are not
sufficient data to conclude on IPCP feasibility in this combination
(20). Hyperthermic intraperitoneal
chemoperfusion (HIPEC) appears to be the most commonly used IPCP
method providing better survival times, although it is currently
not recommended as a standard-of-care option due to the controversy
surrounding its use (21). In
addition, there is no definitive proof supporting the advantage of
HIPEC over normothermic IPCP, and accumulating preclinical data
suggest that HIPEC has no advantage over IPCP (22–24).
Hyperthermia has already been proven to be of no value in isolated
limb chemoperfusion (25). IPCP is
associated with the inherent toxicity of chemotherapy and
additional toxicity due to damage of the peritoneum (26) and septic shock (27). In China, IPCI with cisplatin and
fluorouracil is a widely used standard treatment for PCMA (28,29)
(Table I).
Patients and methods
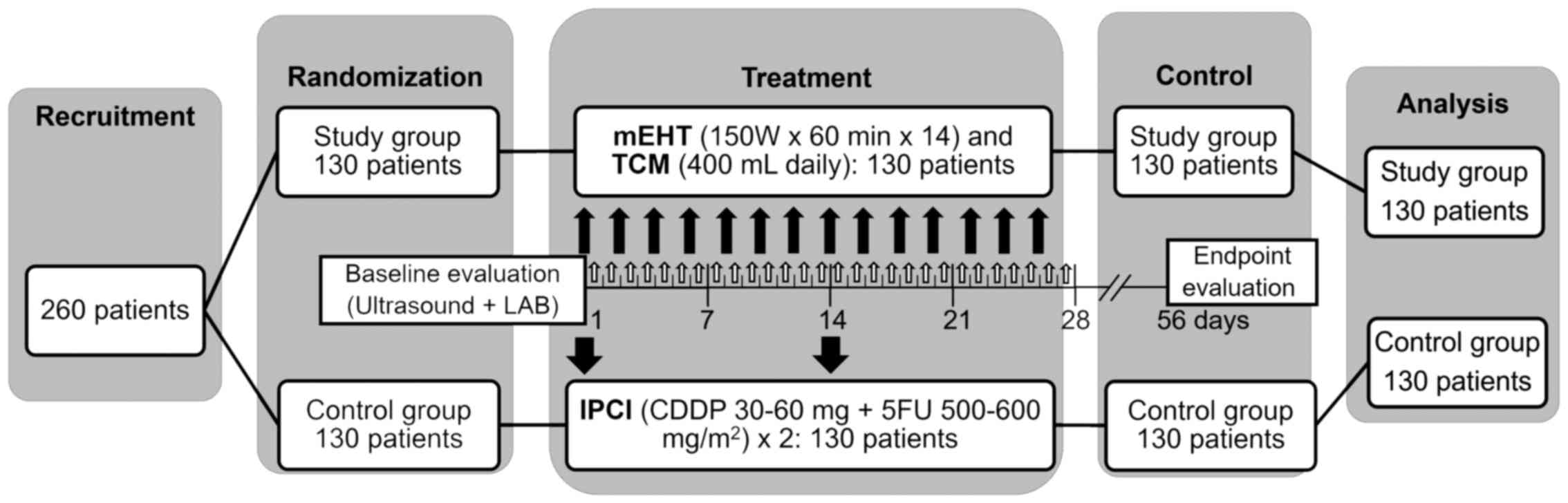
Study design
The present study was a randomized, controlled,
single-center, open-label clinical trial (phase II) with two
parallel groups (allocation ratio, 1:1), which was conducted to
investigate the efficacy and safety of mEHT in combination with TCM
(study group, SG) vs. standard IPCI (control group, CG) in PCMA by
intention-to-treat analysis.
Inclusion and exclusion criteria
Patients who were hospitalized at the Department of
Oncology of Clifford Hospital (Guangzhou, China) were recruited
based on the following inclusion criteria: i) Pathologically
confirmed PC with malignant ascites; ii) Karnofsky performance
status (KPS) score (30) ≥60%; iii)
normal function of bone marrow; iv) predicted survival time >1
month; and v) written informed consent. The exclusion criteria were
as follows: i) Surgery within 3 weeks or incomplete recovery of
postoperative sutures; ii) active bleeding or vascular occlusion in
the mEHT treatment area; iii) emotional instability; iv) difficulty
in placing the patient into the mEHT machine; v) metallic implants
or replacements in the treatment area; vi) implanted electronic
devices; vii) missing or damaged heat-sense nerves or other
field-sensitive issues in the treatment area; and viii) very low
white blood cell count (<1.5×109/l), agranulocytosis
(<0.5×109/l) or severe anemia. Disease staging was
performed according to the NCCN staging criteria (31).
Interventions
Local mEHT
For local mEHT, the EHY-2000 local oncothermia
device was applied (Oncotherm GmbH, Troisdorf, Germany). Treatment
was performed in the supine position with a 30-cm diameter
electrode, 60 min per session. Step-up heating was applied, with a
power increasing from 100 to 150 W over 5–15 min according to the
heat tolerance of the patient. mEHT was applied every second day
within 4 weeks, for a total of 14 sessions.
TCM
The composition of the Shi Pi base decoction was as
follows: i) Atractylodes macrocephala koidz (15 g); ii) Cortex
magnoliae officinalis (10 g); iii) Chaenomeles sinensis (Thouin)
Koehne (9 g); iv) Radix Aucklandiae (6 g); v) Fructus Tsaoko (5 g);
vi) Areca catechu L. (9 g); vii) Poria cocos (Schw.) Wolf (15 g);
viii) Rhizoma zingiberis (9 g); ix) Radix Aconiti Lateralis
Preparata (6 g); x) Radix Glycyrrhizae Preparata (9 g); xi)
Zingiber officinale Roscoe (3 slices); and xii) Fructus jujubae (3
pcs.).
The composition was adjusted according to the
diagnostic criteria of treatment determination based on
pathogenesis obtained through differentiation of symptoms and signs
of TCM (32) as follows:
Syndrome of accumulated dampness-heat
Distension and hardness of abdomen, tympanites and
pain in the gastric cavity and abdomen, feverish dysphoria, bitter
taste in the mouth, feeling of thirst but unwillingness to drink,
occasionally yellow discoloration of the face, eyes and skin of the
body, oliguria with yellow urine, constipation, red tongue with
greasy yellow coating, and stringy, rapid pulse.
Adjustment: Exclusion of Rhizoma zingiberis
and Radix Aconiti Lateralis; addition of Radix Stephaniae
Tetrandrae (15 g), Lepidium apetalum Willd. (12 g),
Fructus Gardeniae (15 g) and Herba Artemisiae
Scopariae (20 g).
Qi-stagnancy and blood stasis type
Distended abdomen, varicose veins on the abdominal
wall, prickling flank pain, unpressable pain, swarthy grey
discoloration of the face, violet discoloration of the lips,
vascular nevus on the cheeks and chest of snake-like shape or
striped, red marks on the palms, feeling of thirst but
unwillingness to drink, black stool, purple red tongue with yellow
coating and thready, irregular pulse.
Adjustment. Exclusion of Atractylodes
macrocephala koidz. and Radix Aconiti Lateralis;
addition of Rhizoma cyperi (12 g), Semen persicae (15
g), Cortex Moutan (12 g) and Radix paeoniae rubra (12
g).
Asthenia of the spleen and kidney type
Distended abdomen, epigastric distension and
depression, anorexia, loose stool, tiredness, aversion to cold,
edema of lower limbs, paleness of the face, pale tongue with thin
white coating and deep, thready, weak pulse.
Adjustment: Addition of Polyporus umbellatus
(Pers) Fr. (15 g) and Radix Aconiti Lateralis (≤12 g).
A total of 400 ml of decoction were prepared from
each dose of the herbs. The decoction was administered orally for 4
weeks, twice a day, 200 ml each time, 30 min after breakfast and
supper.
IPCI
Abdominal paracentesis was performed by
catheterization following closed drainage of the ascites with only
a small amount of residual fluid, and was followed by infusion of
cisplatin (30–60 mg) and fluorouracil (500–600 mg/m2
body surface); dose reductions were applied depending on the
general condition of each patient. Each medication was dissolved in
100 ml of normal saline. Following IPCI, the catheter was occluded.
IPCI was performed every 2 weeks during the 4-week treatment
course, for a total of two courses.
Outcomes
The primary outcome was objective response rate
(ORR); the secondary outcomes were AER and QoL. Tumor response was
assessed according to the World Health Organization criteria
(33) for evaluation of the
therapeutic effect in MA: Complete remission (CR) was defined as
complete absorption of the ascites with no obvious regeneration for
>1 month; partial remission (PR) was defined as >50%
reduction of the ascites, with obvious relief of the abdominal
distention, with maintenance of a less than moderate volume of
ascites under ultrasound detection for >1 month; and no change
(NC) was defined as <50% reduction of the ascites, or no obvious
reduction of the ascites under ultrasound detection, or even
increase of the ascites, with obvious abdominal distention. ORR was
calculated as CR + PR.
QoL was assessed by KPS improvement rate (KPS IR)
and pain according to the KPS IR criteria (20) as follows: (i) Improvement was defined
as a KPS increase of ≥10% after treatment; (ii) worsening was
defined as a KPS reduction of ≥10% after treatment; and (iii) NC
was defined as a change in KPS of <10%.
The pain was assessed using the visual analog scale
(VAS) (34) and AER in accordance
with the Common Terminology Criteria for Adverse Events (CTCAE)
(35).
Sample size and randomization
The sample size was determined as follows: n =
(Uα + Uβ)2 × 2P × (1_P) /
(P1_P0)2, where n is the sample
size of the SG (same for CG); Uα and Uβ are
the corresponding U values for α=0.05 and β=0.01 according to
normal distribution quantile table; P0 and P1
are the expected ORR in CG and SG, respectively, estimated by the
previous results of TCM + mEHT and IPCI at Clifford Hospital; P is
the average ORR. P1=80%, P0=62%;
Uα(0.05)=1.65, Uβ(0.01)=1.28 and
P=(P1+P0)/2=0.71; therefore
n=(1.65+1.28)2 ×2×0.71x(1–0.71)/(0.8–0.62)2
=109.
As ~15% of the sample could be lost, ‘n’ should be
≥126; thus, 130 was defined as the size of the SG.
The patients were randomly distributed into two
groups (SG and CG) according to a random number table with an
allocation ratio of 1:1. For each patient, the dichotomous decision
on the treatment regimen was made by a random allocation sequence
and placed into an opaque, sealed, sequentially numbered envelope.
When the patient consented to entering the trial, the respective
envelope was opened and the appropriate intervention was
applied.
There was no blinding, as concealing mEHT treatment
from both patients and personnel was not feasible (open-label
trial). In order to prevent selection bias and to ensure proper
allocation concealment, recruiting, allocation, operation,
evaluation of therapeutic effect and data analysis were performed
by different individuals. The ‘Chinese wall policy’ was applied to
prevent any communication regarding the trial between different
segments of the trial process.
Data collection and management
All the patients were evaluated after each treatment
by B-mode ultrasound, clinical and laboratory examinations. The
adverse events were evaluated based on objective data and voluntary
testimonies of the patients, or through non-leading questions, and
were recorded into a ‘table of adverse events’.
Data were analyzed by SPSS 19.0 software (IBM Corp,
Armonk, NY, USA). Quantitative data were assessed using the
t-test and multifactor analysis of variance. Data with
non-normal distribution were assessed using the rank-sum test.
Categorical data were assessed by the Chi-squared test.
The present study was performed in accordance with
the CONSORT 2010 statement (36) and
registered on ClinicalTrials.gov (NCT02638051).
Results
Patients and treatment
Between January 3 and December 20, 2014, 260
patients were recruited at the Clifford Hospital. The patients were
randomly allocated into the two groups, with 130 patients assigned
to each group (Fig. 1). There was no
dropout or exclusion following randomization (0/260). All the
patients in the SG (130/130) received the complete prescribed local
mEHT + TCM treatment course, whereas all the patients in the CG
(130/130) received the complete prescribed ICPI course (Fig. 1) with the following average/median
doses: CDDP, 49.63±10.19/50 mg; 5FU, 48.5±39.68/550
mg/m2. There were no significant differences in
symptomatic supportive treatment between the two groups. All the
patients (260/260) were recorded and analyzed on an
intention-to-treat basis.
Baseline data
In the SG, the age range was 27–73 years, with a
mean ± standard deviation (SD) of 58.88±12.43 years. In the CG, the
age range was 24–75 years, with a mean ± SD of 56.07±15.38 years
(P=0.11; Table III). The
percentage of male patients was 55.4 and 46.9% in the SG and CG,
respectively (P=0.17). The primary disease was gastric cancer (16.0
and 18.5% in the SG and CG, respectively), colon cancer (26.2 and
28.5%), rectal cancer (13.8 and 11.5%), pancreatic cancer (10.0 and
6.2%), endometrial cancer (6.9 and 3.8%), ovarian cancer (8.5 and
12.3%) and hepatic cancer (17.7 and 19.2%). There was no
statistically significant difference in terms of primary disease
between the two groups (P=0.7). In SG and CG, the rate of lung
metastasis was 17.7 and 15.4%, of liver metastasis 24.6 and 26.9%,
of metastasis to the celiac lymph nodes 40.8 and 38.5% and to the
bones 16.9 and 19.2%, respectively. There was no statistically
significant difference in the rate and location of metastases
between the two groups (P=0.89). There were no stage I/II patients.
Stage III patients comprised 50.8% of SG and 58.5% of CG. There
were more stage IV patients in SG vs. those in CG (49.2 vs. 41.5%,
respectively), although the difference was not statistically
significant (P=0.21). The performance status was similar between
the two groups (P=0.76; Table
III).
| Table III.Baseline demographic and clinical
characteristics. |
Table III.
Baseline demographic and clinical
characteristics.
|
Characteristics | Study group | Control group | χ2 | P-value |
|---|
| No.
recruited/analyzed | 130/130 | 130/130 |
| 0.106 |
| Age years (mean ±
SD) | 58.88±12.43 | 56.07±15.38 |
|
|
| Gender, n (%) |
|
| 1.863 | 0.172 |
|
Male | 72 (55.4) | 61 (46.9) |
|
|
|
Female | 58 (44.6) | 69 (53.1) |
|
|
| Type of cancer, n
(%) |
|
| 3.829 | 0.700 |
|
Gastric | 22 (16.9) | 24 (18.5) |
|
|
|
Colon | 34 (26.2) | 37 (28.5) |
|
|
|
Rectal | 18 (13.8) | 15 (11.5) |
|
|
|
Pancreatic | 13 (10.0) | 8 (6.2) |
|
|
|
Endometrial | 9 (6.9) | 5 (3.8) |
|
|
|
Ovarian | 11 (8.5) | 16 (12.3) |
|
|
|
Hepatic | 23 (17.7) | 25 (19.2) |
|
|
| Metastases, n
(%) |
|
| 0.622 | 0.891 |
|
Lungs | 23 (17.7) | 20 (15.4) |
|
|
|
Liver | 32 (24.6) | 35 (26.9) |
|
|
| Celiac
lymph nodes | 53 (40.8) | 50 (38.5) |
|
|
|
Bones | 22 (16.9) | 25 (19.2) |
|
|
| Stage, n (%) |
|
| 1.552 | 0.213 |
| I | 0 (0.0) | 0 (0.0) |
|
|
| II | 0 (0.0) | 0 (0.0) |
|
|
|
III | 66 (50.8) | 76 (58.5) |
|
|
| IV | 64 (49.2) | 54 (41.5) |
|
|
| Karnofsky
performance score, n (%) |
|
| 1.179 | 0.758 |
| 60 | 26 (20.0) | 21 (16.2) |
|
|
| 70 | 50 (38.5) | 47 (36.2) |
|
|
| 80 | 42 (32.3) | 48 (36.9) |
|
|
| 90 | 12 (9.2) | 14 (10.8) |
|
|
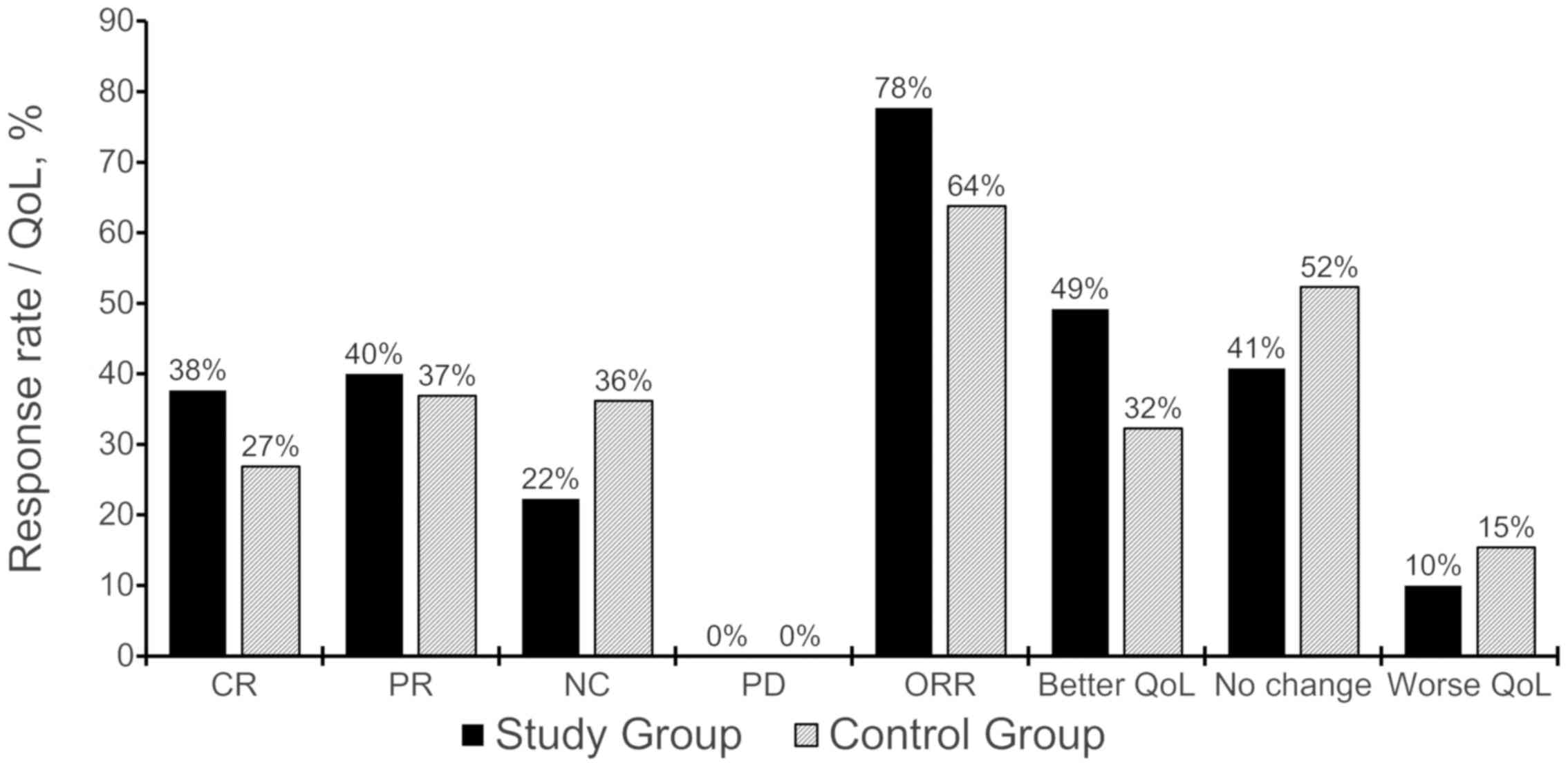
Outcomes and estimation
In the SG, 101 patients (77.69%) exhibited an
objective response (CR + PR) vs. 73 patients (63.85%) in the CG;
the difference was statistically significant (χ2=6.02,
P=0.005). SG patients also exhibited a better CR rate (37.7 vs.
26.9%), although the difference was not statistically significant
(P=0.063). The KPS improved in 49.23% of SG patients vs. 32.3% of
CG patients; the difference was statistically significant
(χ2=7.54, P<0.05; Table
IV and Fig. 2).
| Table IV.Treatment results. |
Table IV.
Treatment results.
|
|
| Objective response,
n (%) | QoL, n (%) |
|---|
|
|
|
|
|
|---|
| Groups | Total cases, n | CR | PR | NC | PD | ORR | Better | NC | Worse | KPS IR, % |
|---|
| Study | 130 | 49 (37.7) | 52 (40.0) | 29 (22.3) | 0 (0.0) | 101 (77.7) | 64 (49.2) | 53 (40.8) | 13 (10.0) | 49.2 |
| Control | 130 | 35 (26.9) | 48 (36.9) | 47 (36.2) | 0 (0.0) | 83 (63.8) | 42 (32.3) | 68 (52.3) | 20 (15.4) | 32.3 |
| P-value | <0.05 | <0.05 |
The total AER was 2.3% (3 cases) in the SG vs. 12.3%
(16 cases) in the CG (P<0.05; Table
V). In SG, all the patients exhibited mild abdominal pain due
to distention. In CG, 5 patients exhibited abdominal pain, 3 had
gastrointestinal reactions, 2 had compromised hepatic or renal
function, and 6 patients exhibited bone marrow suppression. All the
adverse events were grade 1 and they were relieved spontaneously
without special treatment.
| Table V.Adverse event rate. |
Table V.
Adverse event rate.
| Adverse events | Study group, n
(%) | Control group, n
(%) | P-value |
|---|
| Total | 3/130 (2.31) | 16/130 (12.31) | <0.05 |
| Blood and lymphatic
system disorders |
|
|
|
| Bone
marrow suppression | 0/130 (0.00) | 6/130 (4.62) | <0.05 |
| Gastrointestinal
disorders |
|
|
|
|
Abdominal pain | 3/130 (2.31) | 5/130 (3.85) | >0.05 |
|
Gastrointestinal
reactions | 0/130 (0.00) | 3/130 (2.31) | >0.05 |
| Hepatobiliary
disorders |
|
|
|
|
Compromised hepatic
function | 0/130 (0.00) | 1/130 (0.77) | >0.05 |
| Renal and urinary
disorders |
|
|
|
|
Compromised renal
function | 0/130 (0.00) | 1/130 (0.77) | >0.05 |
Discussion
In this study, mEHT was applied in combination with
an orally administered herbal TCM decoction to treat PCMA. mEHT +
TCM treatment was found to achieve better control of PCMA compared
with standard IPCI, with lower toxicity: The ORR in SG vs. CG
patients was 77.69 vs. 63.85%, respectively (P<0.05), and the
KPS improvement rate was 49.23 vs. 32.3%, respectively (P<0.05),
without any significant adverse reactions. Therefore, this combined
treatment may be preferred due to the better balance of benefit and
harm.
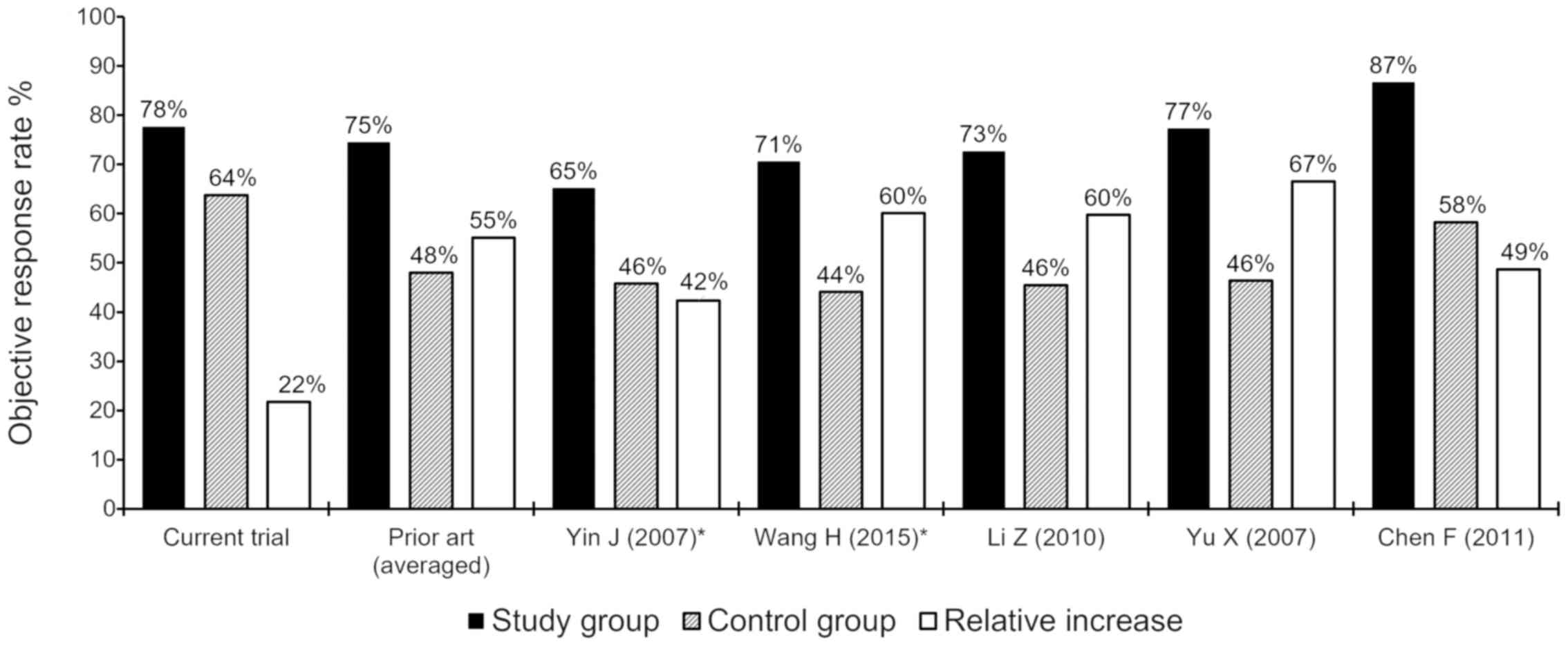
A comparison of the results of the present study to
those of previous HT + TCM studies for PCMA (Tables I–II), suggests that our results were
superior (ORR, 77.7 vs. 74.5% in the SG and 63.8 vs. 48.0% in the
CG, respectively; Fig. 3). It should
be noted that three of the five previous studies were
non-randomized (14,37,38),
whereas the two RCTs (39,40) were small-sized (47 and 68 patients in
total, respectively). Randomization and sample increase
significantly decrease the selection and informational bias,
leading to a significant reduction of the absolute and relative
efficacy. Moreover, the study by Chen (14) with the highest ORR included 33% of
patients with malignant pleuritis, which is clinically a more
easily manageable condition, and the overall population in our
study had more advanced disease (49.2% of the SG patients had stage
IV disease) compared with the other studies.
However, our RCT, which included a larger sample
[>2-fold compared with the nearest trial (14)] and was well-randomized, demonstrated
a better ORR compared with four of five comparative studies, and a
significantly better result in the control arm compared with all
the previous trials. The result in the CG is of major significance,
as it was on the level of the SG results from other RCTs (64 vs.
65–71%) and significantly higher compared with their CGs (64 vs.
42–44%) (39,40). Such a significant superiority in
treatment efficacy (higher by 33% compared with the mean of the
previous studies) indicates significantly better treatment control,
which is pivotal to the quality of an RCT, as inadequate control is
a well-known and widespread cause of bias. Although the relative
increase of the ORR in our study was significantly lower compared
with that in previous trials (22 vs. 55%, respectively), this is
entirely due to the significantly better ORR in the control arm,
which emphasizes the quality of the trial.
In our trial, the relief of MA was usually
associated with a significant decrease or even disappearance of PC
manifestations (Fig. 4). In
addition, although ascites in a proportion of SG patients was not
completely absorbed after 4 weeks of treatment, it was further
absorbed to different degrees (even completely absorbed) at the
1-month follow-up after treatment completion (Fig. 4). This delayed effect of the
treatment may be associated with mEHT, which is known to elicit
delayed apoptotic reactions (41,42) and
to improve immunity (43,44), as well as with the TCM. TCM herbal
medicines increase the sensitivity of cancer to mEHT and, vice
versa, mEHT increases the anticancer effect of herbal medicines
(9). There are broad prospects for
the combination of mEHT with herbal medicines, particularly for
patients who are not sensitive to chemotherapy or those who are
unable to receive chemotherapy. However, further research is
required to study this long-term combined therapeutic effect.
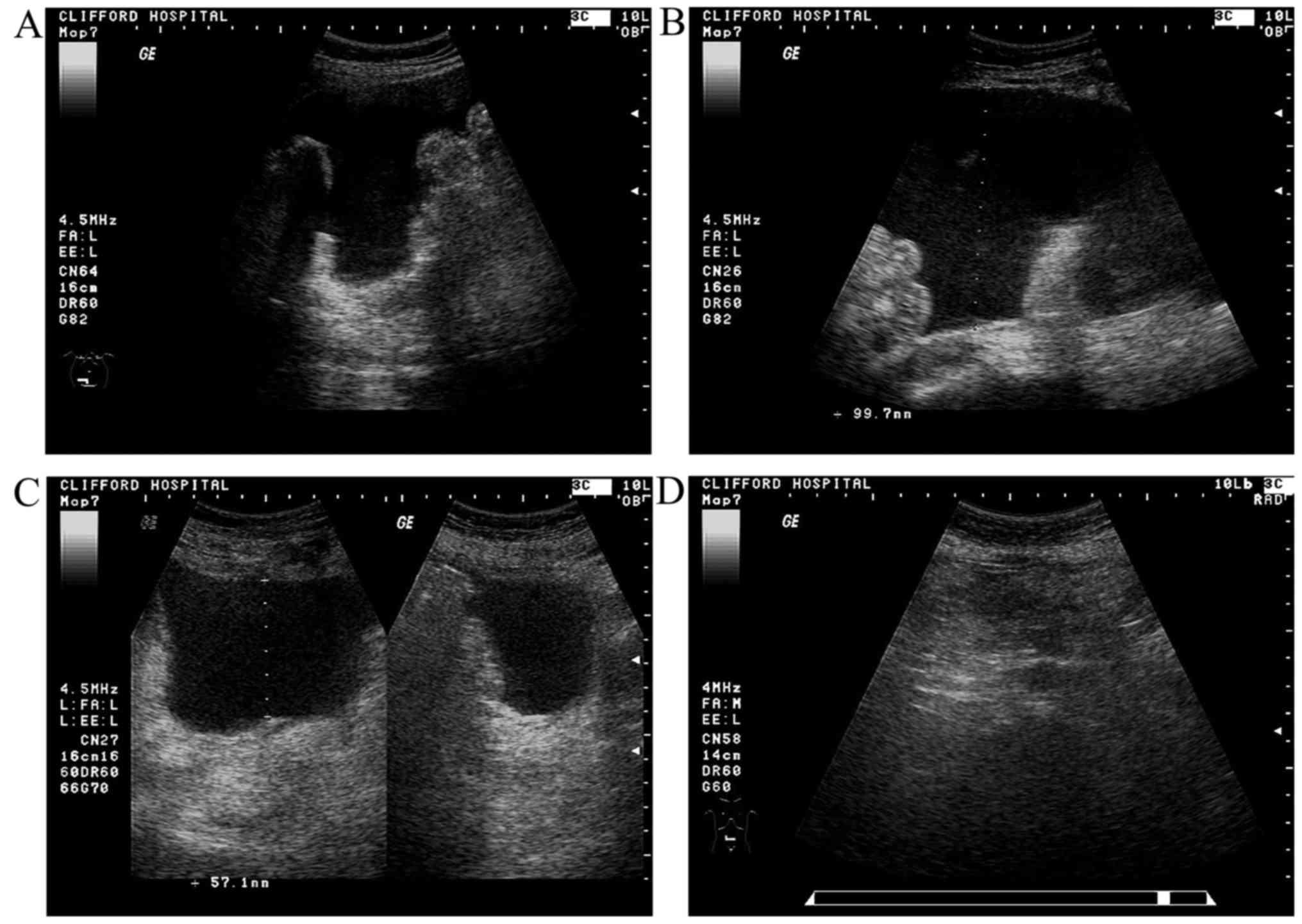 | Figure 4.A typical case of a complete response
in a 60-year-old postoperative patient with ovarian cancer
(oophorohysterectomy in 2007). The patient was diagnosed with
multiple extensive metastases in the liver and the abdominal cavity
with ascites in 2013; following administration of four courses of
IPCI (CDDP + CTX); the ascites resolved. Abdominal distention and
edema of the lower limbs was observed in August, 2014, and one
course of IPCI was administered, without relief and with associated
with adverse reactions such as nausea, vomiting and loss of
appetite. (A and B) The patient was admitted to Clifford Hospital
on September 12, 2014, with severe malignant ascites (maximum
depth, 10.0 cm) and ultrasound signs of multiple peritoneal
carcinomatosis and a KPS of 60%, with significantly compromised
hepatic and renal function on blood tests. mEHT with TCM (‘asthenia
of both the spleen and kidney’ type) treatment was administered
according to the study protocol, without adverse reactions. (C)
Following completion of the treatment on October 16, 2014, there
was relief of the abdominal distention and the edema of the lower
limbs; on blood tests, the hepatic and renal function had returned
to normal; the ascites was moderate (5.7 cm deep), with a
significant reduction in peritoneal carcinomatosis manifestations;
the KPS was 90%. (D) On re-evaluation (November 13, 2014) the
hepatic and renal function tests were normal, there was no obvious
ascites, no obvious intestinal wall thickening and no
characteristic sign of neoplasia; there was also no discomfort and
the KPS was 100%. The patient was in complete remission. |
mEHT was used without previous drainage of the
ascites, as recommended by the EHY-2000 device user manual. This
approach is based on several previous observations of ‘as is’ mEHT
application in cases with tense ascites, with high efficacy and
without side effects. This simplified approach significantly
reduces time and cost, promotes patients' tolerability to treatment
and provides an outstanding advantage in clinical practice.
The main limitations of this trial were the lack of
detailed PC characteristics (45)
and lack of a survival analysis due to the restricted funding of
the trial. Further phase III trials are warranted.
As regards generalizability, the present study
suggests that mEHT in combination with TCM is an effective and safe
treatment for PCMA. Concordance with previous findings indicates
external validity of the present trial's results. In view of
efficacy, safety, ease of application and low treatment cost, our
results are considered to be worthy of clinical generalization.
In conclusion, the combination of mEHT with TCM may
be a preferred treatment option, as it provides better control of
PCMA compared with standard IPCI, with less toxicity. Both
components of this combination are non-toxic treatments easily
tolerated by patients, ensuring a better balance between benefit
and harm.
Acknowledgements
The present trial was funded by the Clifford
Hospital.
Glossary
Abbreviations
Abbreviations:
|
AER
|
adverse event rate
|
|
CG
|
control group
|
|
CR
|
complete remission
|
|
CRPE
|
cytoreductive peritonectomy
|
|
CTCAE
|
Common Terminology Criteria for
Adverse Events
|
|
HIPEC
|
hyperthermic intraperitoneal
chemoperfusion
|
|
HT
|
hyperthermia
|
|
IPCI
|
intraperitoneal chemoinfusion
|
|
IPCP
|
intraperitoneal chemoperfusion
|
|
ITT
|
intention-to-treat analysis
|
|
KPS IR
|
Karnofsky performance score
improvement rate
|
|
MA
|
malignant ascites
|
|
mEHT
|
modulated electro-hyperthermia
|
|
NC
|
no change
|
|
ORR
|
objective response rate
|
|
PC
|
peritoneal carcinomatosis
|
|
PCMA
|
peritoneal carcinomatosis with
malignant ascites
|
|
PR
|
partial remission
|
|
QoL
|
quality of life
|
|
RCT
|
randomized controlled trial
|
|
SG
|
study group
|
|
VAS
|
visual analog scale
|
References
|
1
|
Ayantunde AA and Parsons SL: Pattern and
prognostic factors in patients with malignant ascites: A
retrospective study. Ann Oncol. 18:945–949. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sangisetty SL and Miner TJ: Malignant
ascites: A review of prognostic factors, pathophysiology and
therapeutic measures. World J Gastrointest Surg. 4:87–95. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Roussakow S: Critical analysis of
electromagnetic hyperthermia randomized trials: Dubious effect and
multiple biases. Conference Papers in Medicine 2013. 2013.
View Article : Google Scholar
|
|
4
|
Roussakow S: The history of hyperthermia
rise and decline. Conference Papers in Medicine 2013. 2013.
View Article : Google Scholar
|
|
5
|
The American Cancer Society: Hyperthermia
to Treat Cancer. http://www.cancer.org/treatment/treatmentsandsideeffects/treatmenttypes/hyperthermiaAccessed.
February 16–2017.
|
|
6
|
Ma Shenglin: Research progress of
thermo-chemo-therapy. Mod Pract Med. 16:256–258. 2004.
|
|
7
|
Szasz A, Szasz N and Szasz O: Oncothermia:
Principles and Practices. New York: Springer, NY; pp. 5652011
|
|
8
|
Andocs G, Renner H, Balogh L, Fonyad L,
Jakab C and Szasz A: Strong synergy of heat and modulated
electromagnetic field in tumor cell killing. Strahlenther Onkol.
185:120–126. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pang CLK: Clinical research on integrative
treatment of colon carcinoma with oncothermia and clifford TCM
immune Booster. Oncothermia J. 5:24–41. 2012.
|
|
10
|
Ling Y: Traditional Chinese medicine in
the treatment of symptoms in patients with advanced cancer. Ann
Palliat Med. 2:141–152. 2013.PubMed/NCBI
|
|
11
|
Veith I (translator): The Yellow Emperor's
Classic of Internal Medicine. (1972)Revised paperback edition.
University of California Press; Berkeley, LA: pp. 912002
|
|
12
|
Zheng Y and Gao F: The recognition of TCM
on seroperitoneum of hepatic cirrhosis. J Trad Chinese Med.
5:832008.
|
|
13
|
Zhou D: Oncology of TCM. Guangzhou:
Guangdong High Education Publishing House; pp. 902007
|
|
14
|
Chen F: Clinical research of out-of-body
high frequency hyperthermia in combination with TCM treating
malignant pleural fluid and ascites. J Practical Traditional
Chinese Med. 27:686–687. 2011.
|
|
15
|
Zhou L and Zhang S: Clinical observation
of adjusted Wu Ling Decoction treating 70 patients with malignant
ascites. J Practical Chinese Intern Med. 24:7–711. 2010.
|
|
16
|
Huang X: Observation of Shen Zhu Decoction
in combination with endogeny hyperthermia treating 69 patients with
malignant ascites. J Practical Chinese Intern Med. 20:3882006.
|
|
17
|
Gong S: Observation of the therapeutic
effect of microwave hyperthermia in combination with No2.3
Readjusted Decoction treating malignant pleural fluid and ascites.
J Changchun University of Traditional Chinese Med. 27:643–644.
2011.
|
|
18
|
Ji Sheng Fang: (8 juan/(Song) Yan Yonghe
zhuan). (In Chinese). Taibei: Taiwan shang wu yin shu guan; pp.
1491975
|
|
19
|
Becker G, Galandi D and Blum HE: Malignant
ascites: Systematic review and guideline for treatment. Europ J
Cancer. 42:589–597. 2006. View Article : Google Scholar
|
|
20
|
Matharu G, Tucker O and Alderson D:
Systematic review of intraperitoneal chemotherapy for gastric
cancer. Br J Surg. 98:1225–1235. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
21
|
McRee AJ and O'Neil BH: The role of HIPEC
in gastrointestinal malignancies: Controversies and conclusions.
Oncology (Williston Park). 29:523–524, C3. 2015.PubMed/NCBI
|
|
22
|
Verhulst J: Effects of bevacizumab and
hyperthermia in a rodent model of hyperthermic intraperitoneal
chemotherapy (HIPEC). Int J Hyperthermia. 29:62–70. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zeamari S, Floot B, van der Vange N and
Stewart FA: Pharmacokinetics and pharmacodynamics of cisplatin
after intraoperative hyperthermic intraperitoneal chemoperfusion
(HIPEC). Anticancer Res. 23:1643–1648. 2003.PubMed/NCBI
|
|
24
|
Sørensen O, Andersen AM, Kristian A,
Giercksky KE and Flatmark K: Impact of hyperthermia on
pharmacokinetics of intraperitoneal mitomycin C in rats
investigated by microdialysis. J Surg Oncol. 109:521–526. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kroon HM and Thompson JF: Isolated limb
infusion: A review. J Surg Oncol. 100:169–177. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Di Miceli D, Alfieri S, Caprino P, Menghi
R, Quero G, Cina C, Pericoli Ridolfini M and Doglietto GB:
Complications related to hyperthermia during hypertermic
intraoperative intraperitoneal chemiotherapy (HIPEC) treatment. Do
they exist? Eur Rev Med Pharmacol Sci. 16:737–142. 2012.PubMed/NCBI
|
|
27
|
Jafari MD, Halabi WJ, Stamos MJ, Nguyen
VQ, Carmichael JC, Mills SD and Pigazzi A: Surgical outcomes of
hyperthermic intraperitoneal chemotherapy: Analysis of the american
college of surgeons national surgical quality improvement program.
JAMA Surg. 149:170–175. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhenxia Z, Ziwei L and Ran J: Abdominal
indwelling catheter drainage combined with intracavitary perfusion
chemotherapy for patients with malignant seroperitoneum. J Huaihai
Med. 26:306–528. 2008.
|
|
29
|
Chongqi W, Chiping W and Yuying S: The
clinical value of 5-FU combined with cisplatin for hyperthermic
intraperitoneal chemoinfusion in treating cancerous ascites. Chin J
Med Drug Appl. 2:9–10. 2008.
|
|
30
|
de Kock I, Mirhosseini M, Lau F, Thai V,
Downing M, Quan H, Lesperance M and Yang J: Conversion of karnofsky
performance status (KPS) and Eastern cooperative oncology group
performance status (ECOG) to palliative performance scale (PPS),
and the interchangeability of PPS and KPS in prognostic tool. J
Palliat Care. 29:163–169. 2013.PubMed/NCBI
|
|
31
|
Ovarian cancer including fallopian tube
cancer and primary peritoneal carcinoma. NCCN Clinical Practice
Guidelines in Oncology. Ver. 3.2014. https://www.nccn.org/professionals/physician_gls/f_guidelines.aspAccessed.
February 16–2017.
|
|
32
|
Zhou Daihan: TCM Oncology. Guangdong High
Education Press; 1. 2007, View Article : Google Scholar
|
|
33
|
Sun Yan: Medical Oncology. Beijing:
People's Medical Publishing House; pp. 648–649. 2001
|
|
34
|
Hawker GA, Mian S, Kendzerska T and French
M: Measures of adult pain: Visual Analog Scale for Pain (VAS Pain),
Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire
(MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain
Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS),
and Measure of Intermittent and Constant Osteoarthritis Pain
(ICOAP). Arthritis Care Res (Hoboken). 63:(Suppl 11). S240–S252.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Common Terminology Criteria for Adverse
Events (CTCAE) (v4.03: June 14, 2010) U.S. Department of Health and
Human ServicesNational Institutes of Health. National Cancer
Institute;
|
|
36
|
Moher D, Hopewell S, Schulz KF, Montori V,
Gøtzsche PC, Devereaux PJ, Elbourne D, Egger M and Altman DG:
CONSORT: CONSORT 2010 Explanation and Elaboration: Updated
guidelines for reporting parallel group randomised trials. Int J
Surg. 10:28–55. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Li Z, Zhang L and Li L: Treatment of
malignant ascites with hyperthermic perfusion chemotherapy and
high-frequency hyperthermia. Med J West China. 22:517–521.
2010.
|
|
38
|
Yu X, Li X, Zhou J, et al: The clinical
study of intraperitoneal chemotherapy combined with whole body
hyperthermia by using microwave on abdomen for treating malignant
peritoneal effusion. J Clin Intern Med. 24:253–255. 2007.
|
|
39
|
Yin J, Dai P and Xie Z: Clinical study of
chemotherapeutic hyperthermia intraperitoneal perfusion combined
with high frequency hyperthermia for the treatment of malignant
ascites. Med J Wuhan University. 28:248–250. 2007.
|
|
40
|
Wang H, Liu P, Wang Y, et al: Effects
observation of treating malignant ascites with in vitro
radiofrequency thermotherapy combined intraperitoneal perfusion
chemotherapy. China Clinicians. 43:31–32. 2015.
|
|
41
|
Meggyeshazi N, Andocs G, Balogh L, Balla
P, Kiszner G, Teleki I, Jeney A and Krenacs T: DNA fragmentation
and caspase-independent programmed cell death by modulated
electrohyperthermia. Strahlenther Onkol. 190:815–822. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Andocs G, Meggyeshazi N, Balogh L, Spisak
S, Maros ME, Balla P, Kiszner G, Teleki I, Kovago C and Krenacs T:
Upregulation of heat shock proteins and the promotion of
damage-associated molecular pattern signals in a colorectal cancer
model by modulated electrohyperthermia. Cell Stress Chaperones.
20:37–46. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Tsang YW, Huang CC, Yang KL, Chi MS,
Chiang HC, Wang YS, Andocs G, Szasz A, Li WT and Chi KH: Improving
immunological tumor microenvironment using electro-hyperthermia
followed by dendritic cell immunotherapy. BMC Cancer. 15:7082015.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Akutsu Y, Tamura Y, Murakami K, et al: Can
modulated electro-hyperthermia (mEHT) elicit immune reaction? -From
basic and clinical research. Therm Med. 30:62(WS1WS1-3). 2014.
|
|
45
|
Sugarbaker H: Technical Handbook for the
Integration of Cytoreductive Surgery and Perioperative
Intraperitoneal Chemotherapy into the Surgical Management of
Gastrointestinal and Gynecologic Malignancy. 4th. Ludann Company;
Grand Rapids, MI: pp. 672005
|