Introduction
Gastric schwannoma is slow-growing mesenchymal
neoplasm that originates from Schwann cells (1). This is a rare subgroup of
gastrointestinal stromal tumors (GISTs), which have low malignant
potential, and are clinically distinct from other non-epithelial
tumors of the gastrointestinal (GI) tract, including leiomyoma,
leiomyosarcoma and GI autonomic neurogenic tumors. GI schwannomas
account for ~2–6% of all submucosal tumors, and ~60–70% occur
within the stomach (2). While this
type of tumor rarely occurs in the bowel, schwannomas may develop
in any anatomical region. While the majority of schwannomas are
benign, it is important to accurately identify these tumors as they
may mimic other malignant lesions of the GI tract. This report
presents a case of a schwannoma found at the transverse colon upon
surveillance colonoscopy, which was treated by endoscopic mucosal
resection.
Case report
A 70-year-old female patient was referred by her
primary care physician for surveillance colonoscopy in January
2017. The patient reported no major symptoms, but complained of
occasional episodes of diarrhea over the past month. The patient
was a non-smoker and non-drinker, and review of the systems was
negative for any weight loss. The finding on physical examination
were unremarkable. The vital signs were stable, and the laboratory
results were within normal limits. The patient underwent a
colonoscopy, which revealed evidence of moderately severe
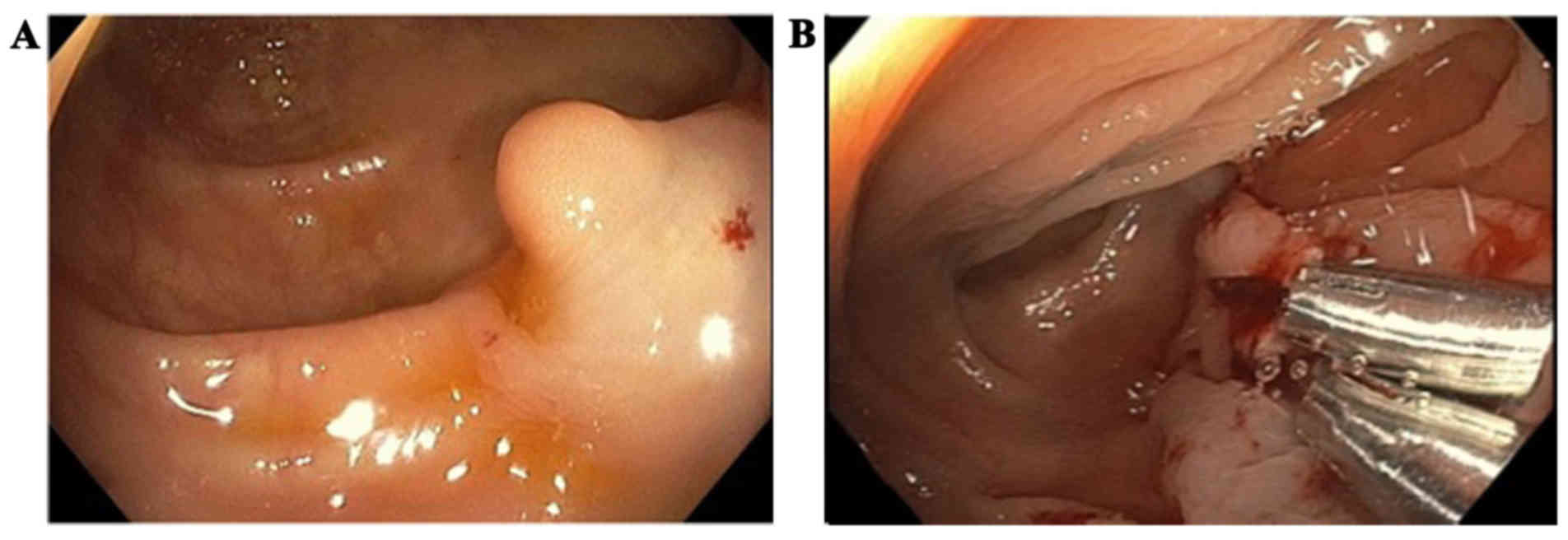
diverticulosis in the sigmoid and descending colon. A single polyp,
measuring 1 cm in size, was identified in the transverse colon.
Saline was injected at the base to raise the polyp prior to removal
(Fig. 1A). The polyp was completely
removed by snare cautery polypectomy. To control bleeding, 2 clips
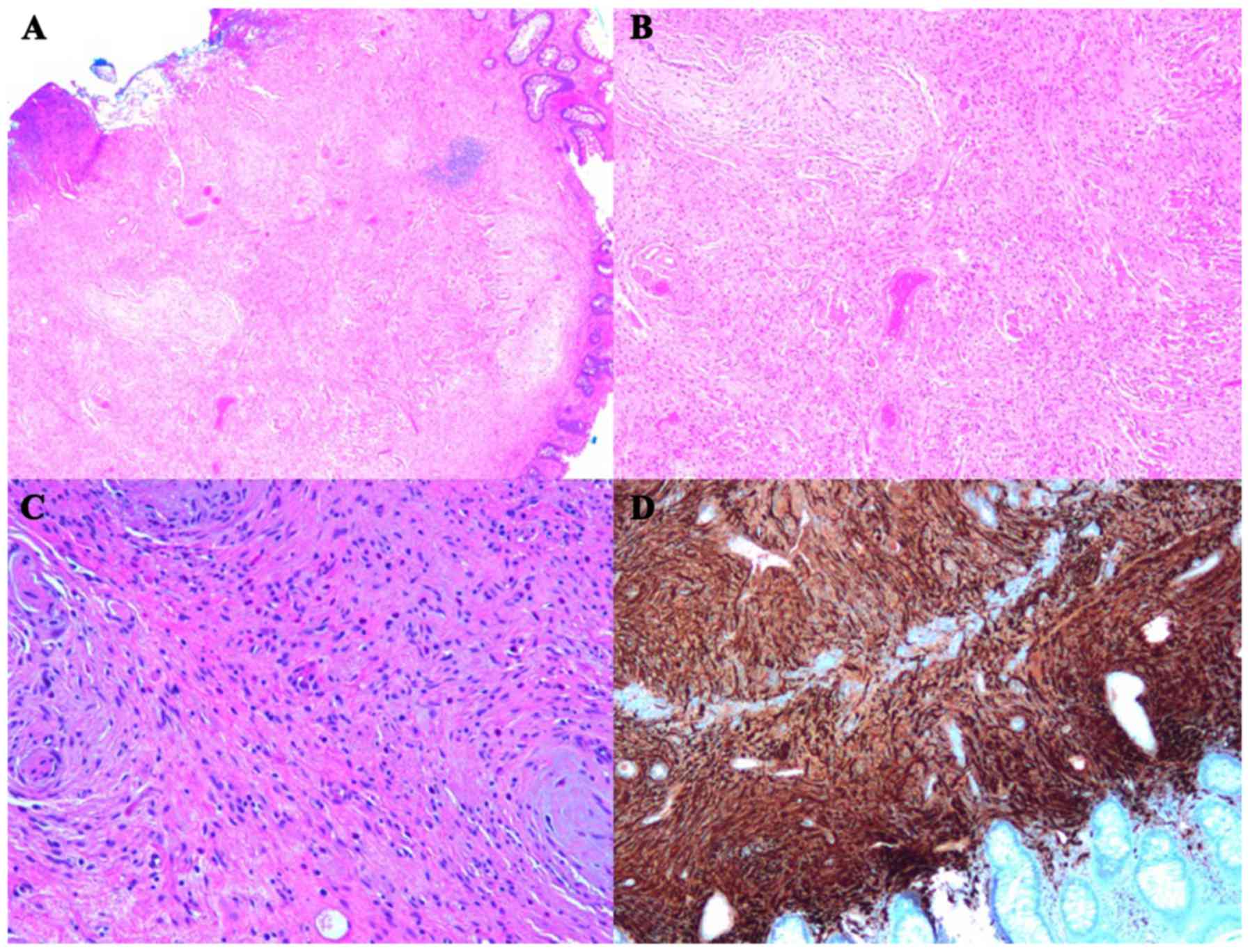
were applied (Fig. 1B). Histological
examination of the polyp showed a solid mass with peripheral
colonic mucosa (Fig. 2A). Higher
resolution revealed fascicles of spindle cells exhibiting nuclear
palisading (Fig. 2B and C).
Immunohistochemistry was positive for S-100 and vimentin, but
negative for CD34 and smooth muscle actin, consistent with GI
schwannoma. The patient made a good postoperative recovery. Consent
was obtained from the patient regarding the publication of the case
details and associated images.
Discussion
GI schwannoma is an extremely rare intestinal
mesenchymal tumor that was first described by Daimaru et al
in 1988. Unlike typical schwannomas, which arise from peripheral
nerves of the skin, connective tissue and internal organs, GI
schwannomas are considered to arise from the autonomous nervous
system, more commonly from the Auerbach's plexus, and less
frequently from the Meissner's plexus (1). Drawing from the few case reports and
studies published on this subject, these cases may occur at any
age, but are most frequently encountered in the fifth and sixth
decades of life, with identical rates for men and women (2). GI schwannoma occurs most frequently in
the stomach (83%) and small intestine (13%), making the finding of
transverse colon schwannoma a very rare clinical entity (3).
Neoplasms originating from the Auerbach's plexus
typically protrude into the intestinal lumen and are characterized
by a non-pedunculated oval-shaped mass; those arising from the
Meissner's plexus are often similar to pedunculated polyps.
Schwannomas are known to be benign neoplasms of ectodermal origin,
which are characterized by a slow growth pattern with the capacity
for malignant degeneration if not removed (4). This type of tumor typically manifests
as a polyp that may ulcerate the mucosa, leading to non-specific
symptoms, including abdominal pain with rectal bleeding, defecation
disorders and colonic obstruction (5).
GI schwannoma is a unique clinical finding, which is
not associated with systemic neurofibromatosis or von
Recklinghausen's disease. Furthermore, while schwannomas are
considered to be a subtype of GIST, they have unique
histopathological and immunohistochemical characteristics, which
are vital for accurate identification. Unlike GISTs, schwannomas
are typically negative for CD117 (KIT), CD34 and actin, but
positive for S-100 and vimentin (6).
Schwannomas are histologically characterized by spiral-like forms
consisting of densely arrayed spindle-shaped tumor cells,
palisading arrangement, and loose reticular networks of tumor cells
(7).
As regards the treatment method, a tumor size of ≥5
cm is considered to be a criterion for surgery, as recurrence and
prognosis vary greatly if the tumor is >5 cm in diameter
(8). However, the benign nature of
the tumor is responsible for the good prognosis of patients with
schwannoma; recurrence and metastasis are considered rare events.
Our patient was treated with endoscopic mucosal resection, a safe
and minimally invasive technique used for removing lesions in the
GI tract. The most frequent complication associated with this
technique is bleeding; however, the rate of this complication is
very low (9).
References
|
1
|
Daimaru Y, Kido H, Hashimoto H and Enjoji
M: Benign schwannoma of the gastrointestinal tract: A
clinicopathologic and immunohistochemical study. Hum Pathol.
19:257–264. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Miettinen M, Sarlomo-Rikala M and Lasota
J: Gastrointestinal stromal tumours. Ann Chir Gynaecol. 87:278–281.
1998.PubMed/NCBI
|
|
3
|
Nonose R, Lahan AY, Santos Valenciano J
and Martinez CA: Schwannoma of the colon. Case Rep Gastroenterol.
3:293–299. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lauwers GY, Erlandson RA, Casper ES,
Brennan MF and Woodruff JM: Gastrointestinal autonomic nerve
tumors: A clinicopathological, immunohistochemical, and
ultrastructural study of 12 cases. Am J Surg Pathol. 17:887–897.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kwon MS, Lee SS and Ahn GH: Schwannomas of
the gastrointestinal tract: Clinicopathological features of 12
cases including a case of esophageal tumor compared with those of
gastrointestinal stromal tumors and leiomyomas of the
gastrointestinal tract. Pathol Res Pract. 198:605–613. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zippi M, Pica R, Scialpi R, Cassieri C,
Avallone EV and Occhigrossi G: Schwannoma of the rectum: A case
report and literature review. World J Clin Cases. 1:49–51. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hasegawa T, Tashiro T, Sekine S, et al:
Pathology and classification of gastrointestinal submucosal tumors
including GIST. Stomach Intestine. 39:396–404. 2004.
|
|
8
|
Jacobson BC, Hirsch MS, Lee JH, Van Dam J,
Shoji B and Farraye FA: Multiple asymptomatic plexiform schwannomas
of the sigmoid colon: A case report and review. Gastrointest
Endosc. 53:801–804. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bergmann U and Beger HG: Endoscopic
mucosal resection for advanced non-polypoid colorectal adenoma and
early stage carcinoma. Surg Endosc. 17:475–479. 2003. View Article : Google Scholar : PubMed/NCBI
|