Introduction
Patients with malignant biliary tract neoplasm,
especially cholangiocarcinoma, are increasing and diagnosis is
mostly made in the advanced stage (1). For patients with locally advanced or
metastatic stage, median overall survival is 11.7 months (2). Although surgical resection offers a
chance for cure (3), complete
resection is sometimes difficult because of vascular invasion
resulting in poor prognosis. Since treatment planning and surgical
procedures are often determined by the presence or absence of
vascular invasion, precise diagnosis is required. Evaluating
vascular invasion is thus crucial to curative resection in patients
with malignant biliary tract neoplasm. Computed tomography (CT) has
been the standard for preoperative evaluation of cholangiocarcinoma
until now because of its ability to noninvasively perform. However,
vascular invasion has been difficult to assess precisely before
surgery. Our hospital has used convex endoscopic ultrasonography
(EUS) for preoperative evaluations of malignant biliary tract
neoplasm. This modality appears very useful for the assessment of
vascular invasion. We can visualize and evaluate the hepatic artery
(HA) and portal vein (PV) at high resolution with the careful
technique we have reported previously (4). However, we do not have clear criteria
for vascular findings from EUS or how to take advantage of vascular
evaluation clinically. The usefulness of vascular evaluation using
EUS in pancreatic cancer cases has been reported (5,6), but no
reports have described in detail the use of this modality for
malignant biliary tract neoplasm. The aim of this study was to
examine the utility of convex EUS for the preoperative evaluation
of malignant biliary tract neoplasm by comparing EUS findings with
histological findings from resected specimens.
Patients and methods
Between January 2008 and January 2016, a total of
150 patients who had been diagnosed with malignant biliary tract
neoplasm (intrahepatic/extrahepatic cholangiocarcinoma, gallbladder
carcinoma, or cystic duct carcinoma) underwent surgery at Aichi
Cancer Center Hospital. We performed EUS as preoperative evaluation
in 82 cases of them and retrospectively retrieved for the
comparison of convex EUS findings with histological findings from
resected specimens. We excluded patients who did not undergo EUS
before surgery. All patients provided written informed consent for
EUS, and this study was approved by the Institutional Review Board
of Aichi Cancer Center Hospital (approval no. 2016-1-322).
Preoperative evaluation
We performed EUS at 7.5-MHz frequency using a convex
linear-array echoendoscope (GF-UGT240 or GF-UCT260; Olympus Medical
Systems, Tokyo, Japan) connected to an ultrasound device (Prosound
α10; Aloka, Tokyo, Japan or EU-ME2 Premier Plus; Olympus Medical
Systems). EUS was performed under conscious sedation using
intravenous midazolam and pethidine hydrochloride. We visualized
and evaluated the HA and PV using a careful technique as we have
reported previously (4). We
evaluated entire HA From the proper HA to the left and right HA. We
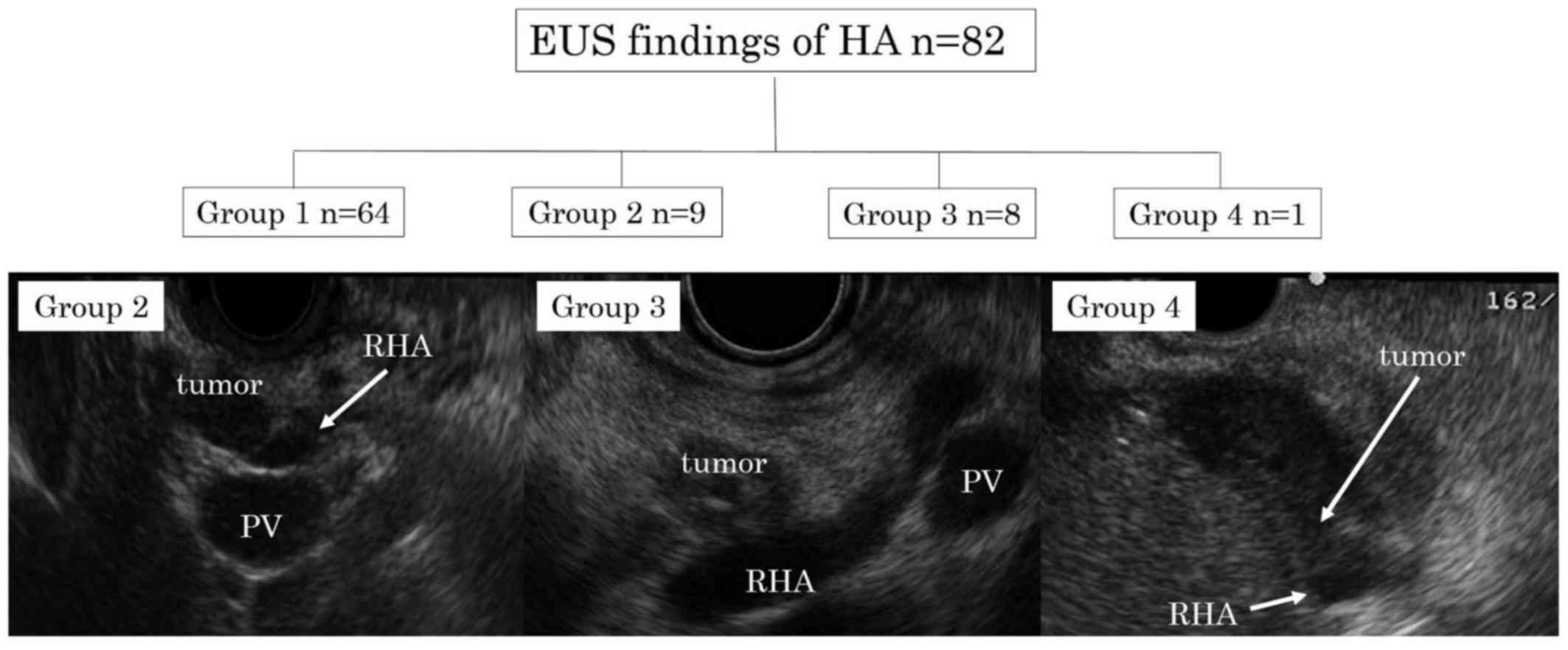
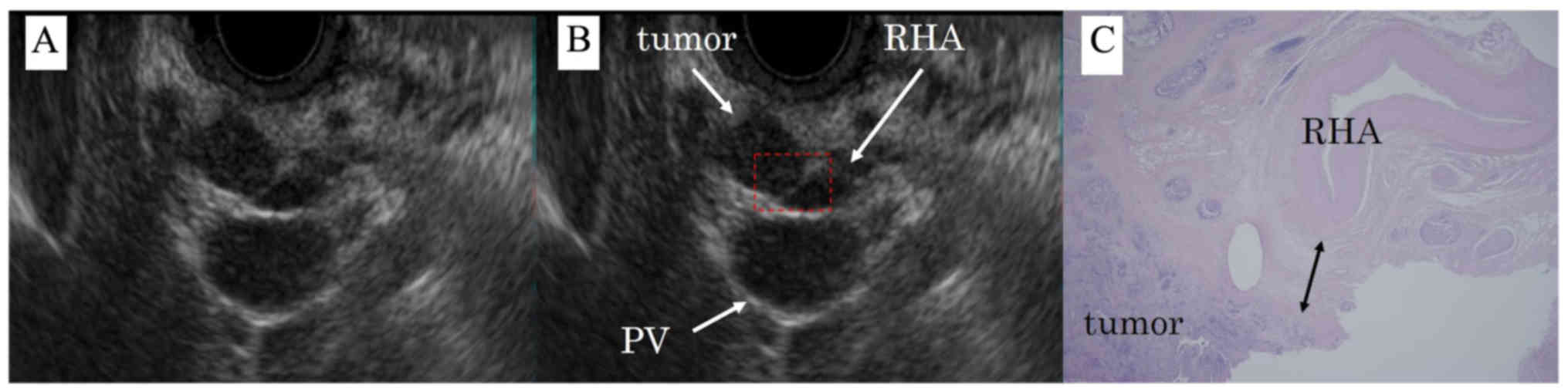
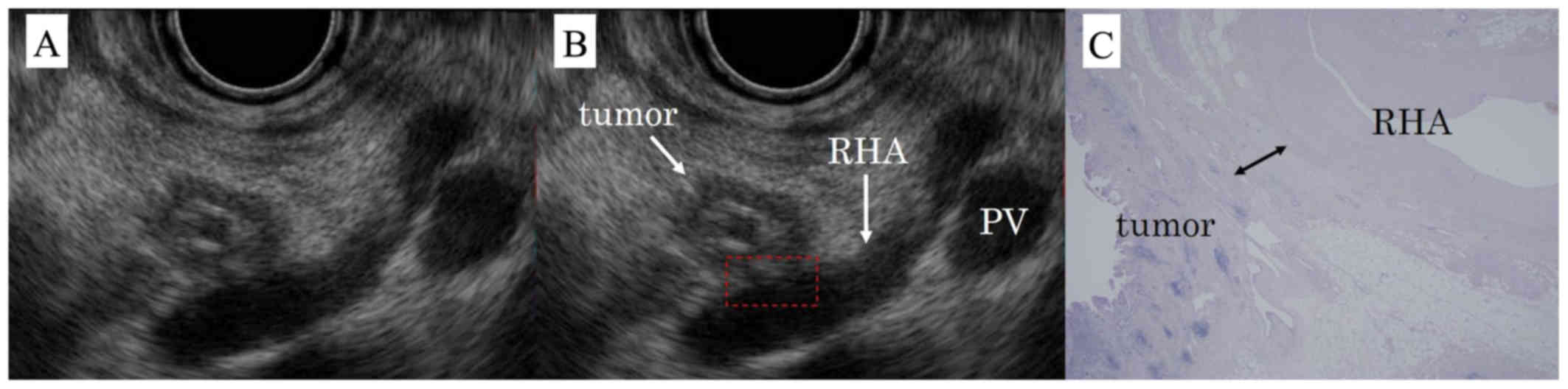
evaluated EUS findings of the HA and PV were evaluated and cases
were divided into four groups by two experienced endosonographers,
as follows: Group 1, obvious hyperechoic tissue between tumor and
vessel; Group 2, close proximity between tumor and vessel without
loss of hyperechoic tissue; Group 3, tumor and vessel contiguity
with loss of hyperechoic tissue; and Group 4, encasement >180°
(Fig. 1).
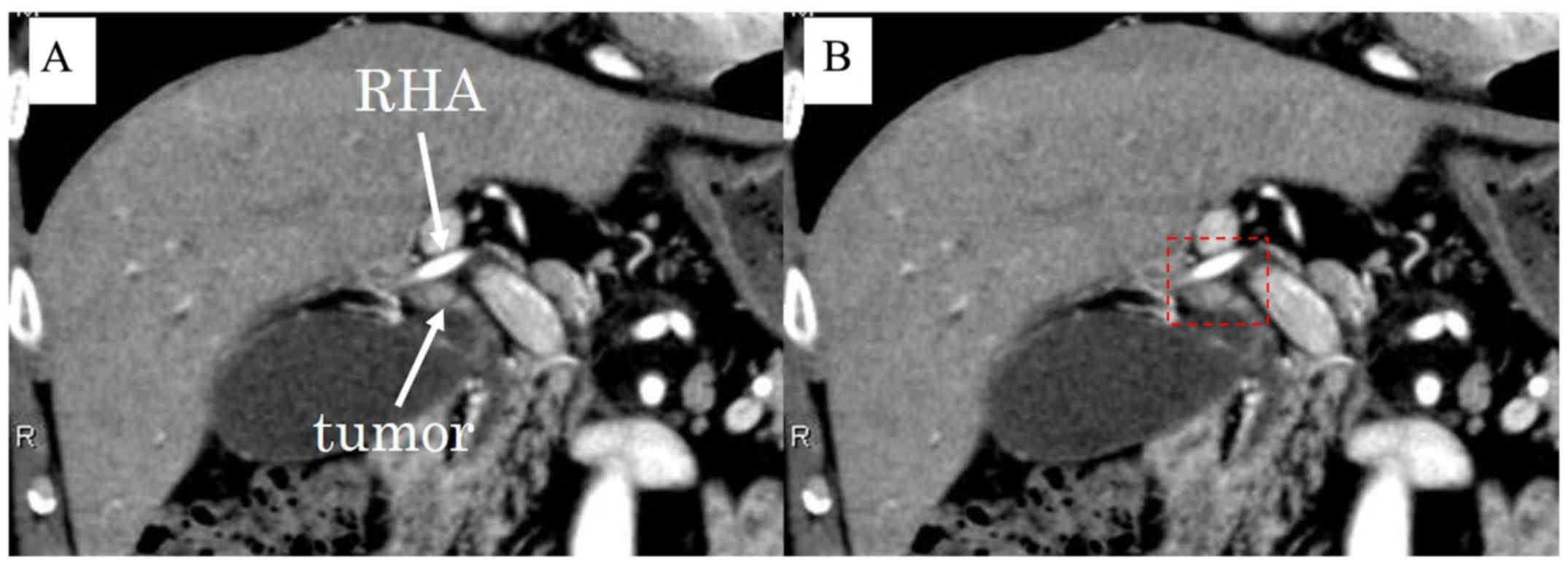
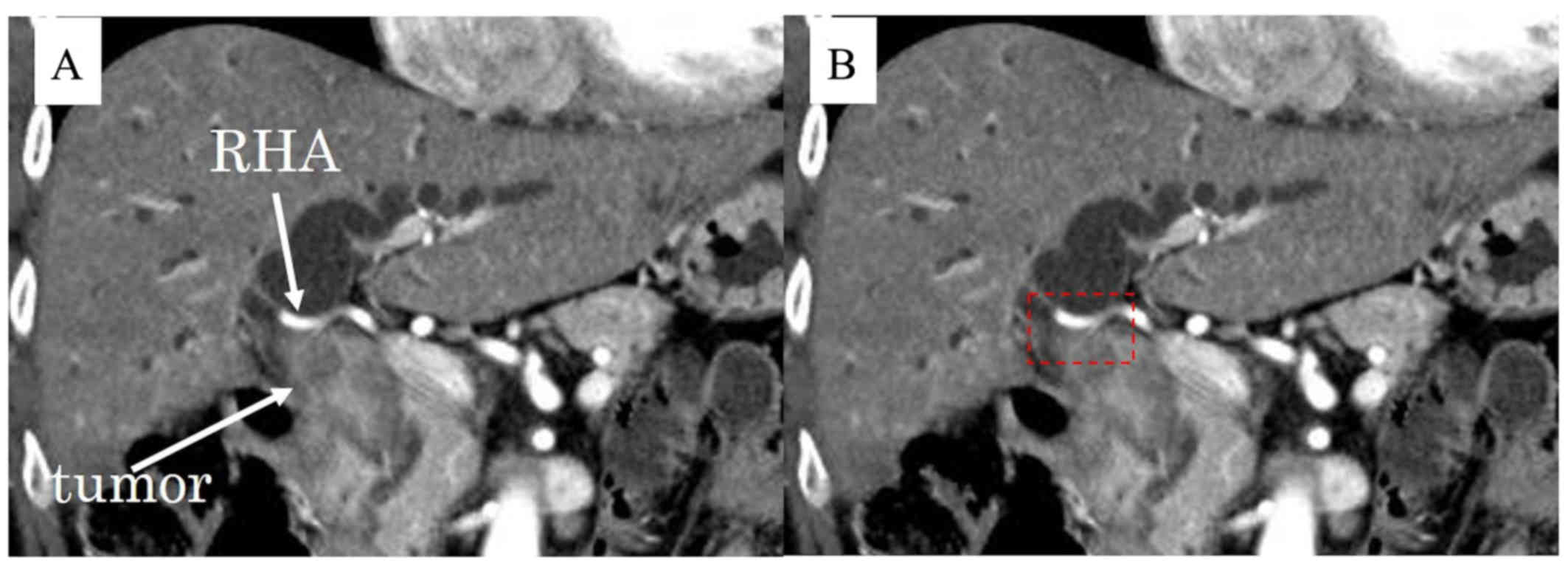
CT findings for the HA and PV were evaluated by two
radiologists. On CT, we defined cases as showing ‘invasion’ when no
boundary was evident between the tumor and vessel (Figs. 2 and 3).
Histological evaluation
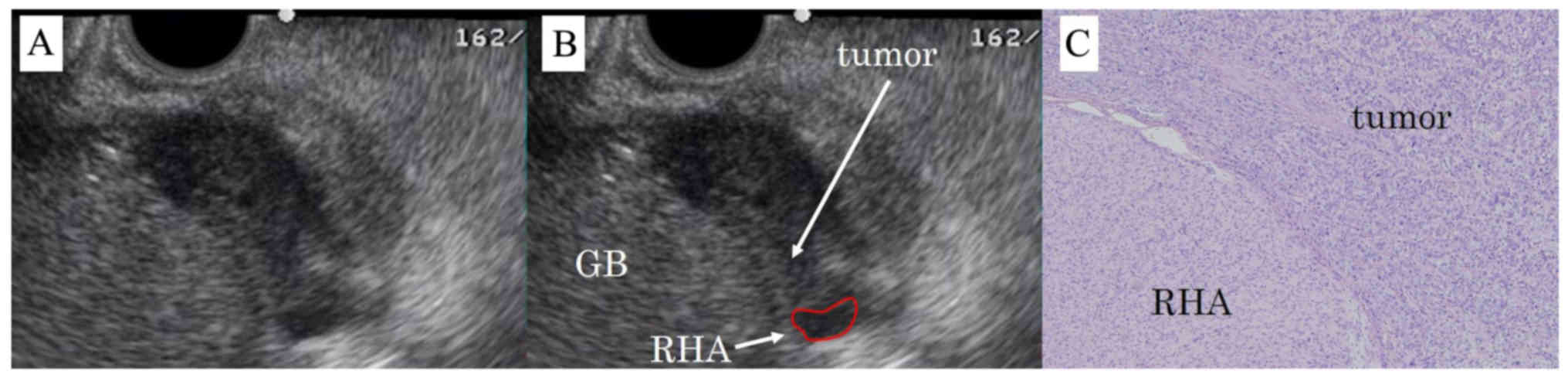
After fixation in 10% formalin, the surgical
specimen was cut transversely into 5-mm slices and slices of serial
sections were added as needed. Each slice was sectioned and stained
with hematoxylin and eosin (H&E). Two pathologists performed
examinations for resected vessels and diagnosed histological
invasion when tumor was found to have infiltrated to the vascular
adventitia (Fig. 4). If no vascular
invasion was present, the distance between the tumor and vascular
adventitia was measured pathologically using a microscope in cases
whose the HA and PV had been resected (Figs. 5 and 6). In cases whose the HA was able to be
separated from the tumor intraoperatively despite being close on
EUS, we analyzed the clinical course and local recurrence rate.
Pathological findings were described using the TNM Classification
of Malignant Tumors by the International Union Against Cancer
(7).
Results
Patients included 58 men and 23 women, with a median
age of 70 years (range, 44–86 years). Patients underwent surgery
for intrahepatic/extrahepatic cholangiocarcinoma (n=2/54),
gallbladder carcinoma (n=21), cystic duct carcinoma (n=4), or lymph
node recurrence of cholangiocarcinoma (n=1). One case involved
extrahepatic cholangiocarcinoma concomitant with gallbladder
carcinoma. Histological type included 79 adenocarcinomas and 3
adenosquamous carcinomas (Table I).
Operative procedures for these patients are shown in Table II. Twenty-seven patients underwent
pancreatoduodenectomy, while 16 patients underwent right
hepatectomy, caudal lobectomy, and bile duct resection. Patient
groupings according to EUS findings for the HA were: Group 1, 64
patients; Group 2, 9 patients; Group 3, 8 patients; and Group 4, 1
patient.
 | Table I.Clinicopathological features of
patients in this study. |
Table I.
Clinicopathological features of
patients in this study.
| Characteristics | n |
|---|
| Males/females | 58/23 |
| Age, years, median
(range) | 70 (44–86) |
| Location |
|
|
Extrahepatic bile duct
(Bp/Bd) | 21/33 |
|
Gallbladder (Gn/Gb/Gf/C) | 5/4/12/4 |
|
Intrahepatic bile duct | 2 |
|
Recurrence of
cholangiocarcinoma (lymph node) | 1 |
| Histological
type |
|
|
Adenocarcinoma/adenosquamous
carcinoma | 79/3 |
| Stage (UICC 7th) |
|
|
0/I/IA/IB/II/IIA/IIB/III/IIIA/IIIB/ | 1/3/6/7/12/9/16/ |
|
IV/IVA/IVB | 1/1/18/2/2/4 |
| Table II.Operative procedures in this
study. |
Table II.
Operative procedures in this
study.
| Operative
procedure | n |
|---|
| PD | 27 |
| BDR | 3 |
| Cholecystectomy | 3 |
|
Cholecystectomy+gallbladder bed
resection | 6 |
|
Cholecystectomy+gallbladder bed
resection+BDR | 3 |
| Right
hepatectomy+CHx+BDR | 16 |
| Right
hepatectomy+CHx+BDR+PD | 3 |
| Left
hepatectomy+CHx+BDR | 10 |
| Left
hepatectomy+CHx+BDR+PD | 3 |
| Right
trisectionectomy+PD | 1 |
| Left
trisectionectomy | 3 |
| Central
bisectomy+PD | 1 |
| CHx+PD | 1 |
| Lymphadenectomy | 1 |
We then compared EUS results with findings from
resected specimens. No cases in Group 1 showed invasion from
intraoperative macroscopic findings or histological findings of
resected specimens. Naturally, the single case in Group 4 showed
histological invasion (Fig. 4).
These results were not inconsistent with preoperative EUS
findings.
We thus performed detailed examinations of Groups 2
and 3, in which the tumor was close to the HA but no obvious
encasement was evident (Tables
III, IV). In preoperative
evaluation by CT, 2 of 9 cases in Group 2 (22.2%) and 7 of 8 cases
in Group 3 (87.5%) were predicted positive for HA invasion. As
shown in Tables III and IV, the HA was more difficult to evaluate
on CT in cases from Group 3 than in cases from Group 2, naturally.
In Group 2, the HA could be separated from the tumor during surgery
in 5 cases, whereas 4 cases underwent combined HA resection. Local
recurrence was seen in 1 of the 5 cases in which the HA was
separable from the tumor (20%). Distances between the HA and the
bile duct of the tumor site in the pathological specimens of the 4
cases that underwent combined HA resection were 710, 1,200, 1,300
and 2,300 µm. Among these, local recurrence was observed in 1 case.
Group 3 included 5 cases in which the HA could be separated from
the tumor during surgery, and 3 cases that underwent combined HA
resection. Distances between the HA and the bile duct of the tumor
site on the pathological specimens of the 3 cases with combined HA
resection were 0, 200 and 474 µm. Of these, local recurrence was
seen in the case with a distance of 474 µm. In Group 3 cases, it
was confirmed that the distance between the tumor and the HA was
close compared to Group 2 on the pathological specimen. Normal
hyperechoic tissue between the tumor and vessel disappeared at
distances of 474–710 µm according to the results. We could not
visualized the boundary between the tumor and the HA in group 3
cases by convex EUS. No clinical differences in separation rates
were evident between cases in Groups 2 and 3. Among the 10 cases
from Groups 2 and 3 in which the HA and tumor were able to be
separated during surgery, only 1 case showed local recurrence, and
no significant difference in local recurrence rate was evident
between Groups 2 and 3. All cases from Groups 2 and 3 either showed
no histological invasion or could be separated from the tumor
intraoperatively. When the tumor could be separated from the HA,
circumferential resection margins were also negative for cancer
cells on histological examination.
| Table III.Characteristics of clinical findings
and postoperative course in Group 2. |
Table III.
Characteristics of clinical findings
and postoperative course in Group 2.
| Case | Location | Vessel | CT diagnosis | Histological
diagnosis | Distance between
tumor and HA | Postoperative
follow-up (months) |
|---|
| 1 | Bd | RHA | − | − | 710 µm | 85 |
| 2 | Bp | RHA | − |
| N/A | 4 (local
recurrence) |
| 3 | Bd | RHA | − | − | 1,200 µm | 31 (peritoneal
recurrence) |
| 4 | Gn | RHA | − | − | 1,300 µm | 2 (local
recurrence) |
| 5 | Bp | RHA | + |
| N/A | 68 |
| 6 | Bp | RHA | − | − | 2,300 µm | 11a |
| 7 | Bp | RHA | − |
| N/A | 11 (peritoneal
recurrence) |
| 8 | Bd | RHA | − |
| N/A | 13 |
| 9 | C | RHA | + |
| N/A | 12 |
| Table IV.Characteristics of clinical findings
and postoperative course in Group 3. |
Table IV.
Characteristics of clinical findings
and postoperative course in Group 3.
| Case | Location | Vessel | CT diagnosis | Histological
diagnosis | Distance between
tumor and HA | Postoperative
follow-up (months) |
|---|
| 10 | Bp | RHA | + |
| N/A | 3a |
| 11 | Bp | RHA | + |
| N/A | 25 (LN
recurrence) |
| 12 | Bd | MHA | + |
| N/A | 9 (liver
recurrence) |
| 13 | Bp | RHA | + | − | 0 | 39a |
| 14 | Bp | RHA | + | − | 474 µm | 7 (local
recurrence) |
| 15 | Bp | RHA | + |
| N/A | 22 |
| 16 | Bd | RHA | + | − | 200 µm | 24 (LN
recurrence) |
| 17 | Bd | RHA | − |
| N/A | 37 |
We also investigated PV invasion (Table V). One case in Group 2 underwent
combined PV resection. The distance between the PV and the bile
duct of the tumor site on pathological specimens was 2,000 µm. In
Group 3 (n=6), the PV could be separated from the tumor during
surgery in 1 case, and 1 case underwent combined PV resection
without histological infiltration; all the remaining cases showed
histological invasion. Among the 6 cases in which the tumor and PV
appeared in contact with each other on EUS (Group 3), 4 cases
(66.7%) showed PV invasion. This result differed from the
examination of the HA.
| Table V.Clinical features of cases with
suspected PV invasion. |
Table V.
Clinical features of cases with
suspected PV invasion.
| Case | Location | Vessel | EUS
classification | CT diagnosis | Distance between
tumor and PV |
|---|
| 4 | Gf | PV | Group 2 | + | 2,000 µm |
| 5 | Bp | LPV | Group 3 | + | Invasion |
| 11 | Bp | LPV | Group 3 | + | 385 µm |
| 12 | Bd | PV | Group 3 | − | Invasion |
| 15 | Bp | RPV | Group 3 | − | N/A |
| 18 | Gn | PV | Group 3 | + | Invasion |
| 19 | Bp | LPV | Group 3 | + | Invasion |
| 20 | Bp | LPV | Group 4 | + | Invasion |
| 21 | Bd | RPV | Group 4 | − | Invasion |
| 22 | Bp | RPV | Group 4 | + | Invasion |
Discussion
For patients with malignant biliary tract neoplasm,
surgical resection is the only chance for cure (3). Accurate evaluation of vascular invasion
is thus critical for choosing the most appropriate surgical
procedure. The evaluation for resectability requires careful
patient selection and meticulous interpretation of imaging studies
(8). EUS offers marked advantages
over CT and other imaging modalities in allowing assessment of echo
structures in lesions <1 cm in diameter (9). We have reported convex EUS as useful
for the assessment of vascular invasion in cancers including the
hepatic hilum (4). EUS provides
high-resolution power without echo attenuation and without the
influence of gastrointestinal gas, thanks to the close apposition
of the echoendoscope to abdominal vessels (10). As a result, EUS is suited to the
evaluation of vessel invasion. The accuracy of identifying vascular
invasion by cholangiocarcinoma has been reported as 87–100%
(11–14) for CT, whereas EUS offers 88–100%
accuracy for predicting PV invasion and performs better than
transabdominal US and angiography in this regard (15–17).
However, those reports did not compare other imaging modalities and
clinical courses in detail and we do not have clear criteria for
vascular findings obtained by EUS. To the best of our knowledge,
the present study represents the first report to compare EUS
findings with histological findings from resected specimens and to
analyze histological invasion, clinical course, and local
recurrence rates in detail. Normal hyperechoic tissue between the
tumor and vessel disappeared at distances of 474–710 µm according
to the results of this study. When tumor was close to the HA on CT
but no obvious encasement was visualized on convex EUS, all cases
either showed no histological invasion or the HA was able to be
separated from the tumor during the operation. However, the same
could not be said for the PV, although the cause was unknown. When
the tumor and PV appeared in contact on EUS (Group 3), 4 of the 6
cases (66.7%) showed PV invasion. Miyazaki et al (18) reported on combined vascular resection
for hilar cholangiocarcinoma. They found that cancer invasion into
the adventitia was present in 80% of the 44 resected portal veins
and 40% of the 9 resected hepatic arteries, and concluded that
caution should be exercised when planning combined hepatic artery
resection, because cancer invasion into the adventitia of the HA
occurs in only about half of the patients despite clinical findings
of apparent invasion. In that series, combined vascular resection
was performed when cancer invasion to the vessels was diagnosed on
the basis of both preoperative imaging and intraoperative
macroscopic findings (18). Ebata
et al also reported performing combined PV resection in 52
cases, 16 of which patients did not show PV invasion, despite the
fact that all PV resections were carried out only after the PV
adhered to and could not be freed from the tumor during surgery. In
that report, the distance between the leading edge of the cancer
and the outer layer of the adventitia ranged from 50 to 1,375 µm
(19). Assessing vascular invasion
before surgery has thus been difficult. Compared with the HA, the
PV is relatively easy to include in combined resection and
reconstruction such as wedge resection is also simpler (19), so invasion to the PV is no longer
considered a contraindication for surgery and is less important
than the evaluation of arterial invasion. Vascular invasion of the
HA is still a contraindication and combined resection and
reconstruction of the HA is technically challenging (20). From the results of our study, we
consider surgery when the tumor is close to the HA on CT but no
obvious encasement is visualized on convex EUS. This study may
offer a new indication in the preoperative evaluation of malignant
biliary tract neoplasm. However, some limitations must be
considered when interpreting the results of this retrospective
study. Selection bias may have been present, because all patients
underwent surgery. In addition, all data were retrospectively
collected from a single center. Further studies are necessary to
clarify the utility of our findings.
In conclusion, convex EUS appears useful for
preoperative evaluation of malignant biliary tract neoplasm. We can
consider surgery when the tumor is close to the HA on CT but there
is no obvious encasement visualized by convex EUS.
References
|
1
|
Valle JW: Advances in the treatment of
metastatic or unresectable biliary tract cancer. Ann Oncol. 21
Suppl 7:vii345–vii348. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Valle J, Wasan H, Palmer DH, Cunningham D,
Anthoney A, Maraveyas A, Madhusudan S, Iveson T, Hughes S, Pereira
SP, et al: Cisplatin plus gemcitabine versus gemcitabine for
biliary tract cancer. N Engl J Med. 362:1273–12781. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Khan SA, Thomas HC, Davidson BR and
Taylor-Robinson SD: Cholangiocarcinoma. Lancet. 366:1303–1314.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hara K, Bhatia V, Hijioka S, Mizuno N and
Yamao K: A convex EUS is useful to diagnose vascular invasion of
cancer, especially hepatic hilus cancer. Dig Endosc. 23 Suppl
1:26–28. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yang R, Lu M, Qian X, Chen J, Li L, Wang J
and Zhang Y: Diagnostic accuracy of EUS and CT of vascular invasion
in pancreatic cancer: A systematic review. J Cancer Res Clin Oncol.
140:2077–2086. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tellez-Avila FI, Chavez-Tapia NC,
Lόpez-Arce G, Franco-Guzmán AM, Sosa-Lozano LA, Alfaro-Lara R,
Chan-Nuñez C, Giovannini M, Elizondo-Rivera J and Ramírez-Luna MA:
Vascular invasion in pancreatic cancer: Predictive values for
endoscopic ultrasound and computed tomography imaging. Pancreas.
41:636–638. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Sobin L, Gospodarowicz M and Wittekind C:
UICC international union against cancerTNM Classification of
Malignant Tumours. Wiley-Blackwell; New York: pp. 118–126. 2009
|
|
8
|
Lazaridis KN and Gores GJ:
Cholangiocarcinoma. Gastroenterology. 128:1655–1667. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Irisawa A and Yamao K: Curved linear array
EUS technique in the pancreas and biliary tree: Focusing on the
stations. Gastrointest Endosc. 69(2 Suppl): S84–S89. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mohamadnejad M, DeWitt JM, Sherman S,
LeBlanc JK, Pitt HA, House MG, Jones KJ, Fogel EL, McHenry L,
Watkins JL, et al: Role of EUS for preoperative evaluation of
cholangiocarcinoma: A large single-center experience. Gastrointest
Endosc. 73:71–78. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Unno M, Okumoto T, Katayose Y, Rikiyama T,
Sato A, Motoi F, Oikawa M, Egawa S and Ishibashi T: Preoperative
assessment of hilar cholangiocarcinoma by multidetector row
computed tomography. J Hepatobiliary Pancreat Surg. 14:434–440.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Watadani T, Akahane M, Yoshikawa T and
Ohtomo K: Preoperative assessment of hilar cholangiocarcinoma using
multidetector-row CT: Correlation with histopathological findings.
Radiat Med. 26:402–407. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lee HY, Kim SH, Lee JM, Kim SW, Jang JY,
Han JK and Choi BI: Preoperative assessment of resectability of
hepatic hilar cholangiocarcinoma: Combined CT and cholangiography
with revised criteria. Radiology. 239:113–121. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Endo I, Shimada H, Sugita M, Fujii Y,
Morioka D, Takeda K, Sugae S, Tanaka K, Togo S, Bourquain H and
Peitgen HO: Role of three-dimensional imaging in operative planning
for hilar cholangiocarcinoma. Surgery. 142:666–675. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sugiyama M, Hagi H, Atomi Y and Saito M:
Diagnosis of portal venous invasion by pancreatobiliary carcinoma:
Value of endoscopic ultrasonography. Abdom Imaging. 22:434–438.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tio TL, Reeders JW, Sie LH, Wijers OB,
Maas JJ, Colin EM and Tytgat GN: Endosonography in the clinical
staging of Klatskin tumor. Endoscopy. 25:81–85. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mukai H, Nakajima M, Yasuda K, Mizuno S
and Kawai K: Evaluation of endoscopic ultrasonography in the
pre-operative staging of carcinoma of the ampulla of Vater and
common bile duct. Gastrointest Endosc. 38:676–683. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Miyazaki M, Kato A, Ito H, Kimura F,
Shimizu H, Ohtsuka M, Yoshidome H, Yoshitomi H, Furukawa K and
Nozawa S: Combined vascular resection in operative resection for
hilar cholangiocarcinoma: Does it work or not? Surgery.
141:581–588. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ebata T, Nagino M, Kamiya J, Uesaka K,
Nagasaka T and Nimura Y: Hepatectomy with portal vein resection for
hilar cholangiocarcinoma: Audit of 52 consecutive cases. Ann Surg.
238:720–727. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Matsuyama R, Mori R, Ota Y, Homma Y,
Kumamoto T, Takeda K, Morioka D, Maegawa J and Endo I: Significance
of vascular resection and reconstruction in surgery for hilar
cholangiocarcinoma: With special reference to hepatic arterial
resection and reconstruction. Ann Surg Oncol. 23 Suppl 4:S475–S484.
2016. View Article : Google Scholar
|