Introduction
Ectopic thyroid tissue is a rare condition resulting
from abnormal embryological development and migration of thyroid
gland. It can be found anywhere along the path of the thyroid
descent, from the floor of the primitive foregut to the final
position of the thyroid in the neck. The estimated frequency of
ectopic thyroid is 1 per 100,000 to 300,000 individuals (1), with lingual thyroid accounting for 90%
of cases (2). Extra-lingual ectopic
thyroid is less frequently encountered and its location in breast
is extremely rare. According to the literature review performed by
the authors this is the first case of multifocal ectopic thyroid
tissue including breast. Ectopic intra-mammary thyroid can be
confused with other diseases such as cysts, intra-mammary lymph
nodes, and fat necrosis.
Case report
A 53-year-old woman was admitted to Kangbuk Samsung
Hospital (Seoul, Korea) to confirm the breast lesion. She visited
our Breast and Thyroid Center due to multiple nodular lesions in
the left breast, which were detected during routine radiological
examinations for more than 10 years. She has a surgical history of
right thyroidectomy due to nodular hyperplasia diagnosed 16 years
ago. In addition, she had excision for palpable masses in the right
medial infraclavicular lesion (measuring 1.6 cm in the largest
diameter) and left sternoclavicular junction (1.4 cm in the largest
diameter) 10 years ago. The pathologic diagnosis for masses was
ectopic thyroid. Thyroid function tests assessing TSH and Free T4
were carried out every year and showed euthyroidism status. Because
the patient's thyroid function was normal, the patient did not
receive any medications or thyroid hormone supplements, except
vitamin D3. Ultrasonography performed 10 years ago showed multiple
scattered cysts in bilateral breast. The largest lesion was located
in the left breast and measured about 0.5 cm in size (Fig. 1). They were thought to be benign
findings such as cysts, intra-mammary lymph nodes or fat necrosis
based on Breast Imaging-Reporting and Data System 2 criteria. No
associated inflammatory signs or skin changes were detected.
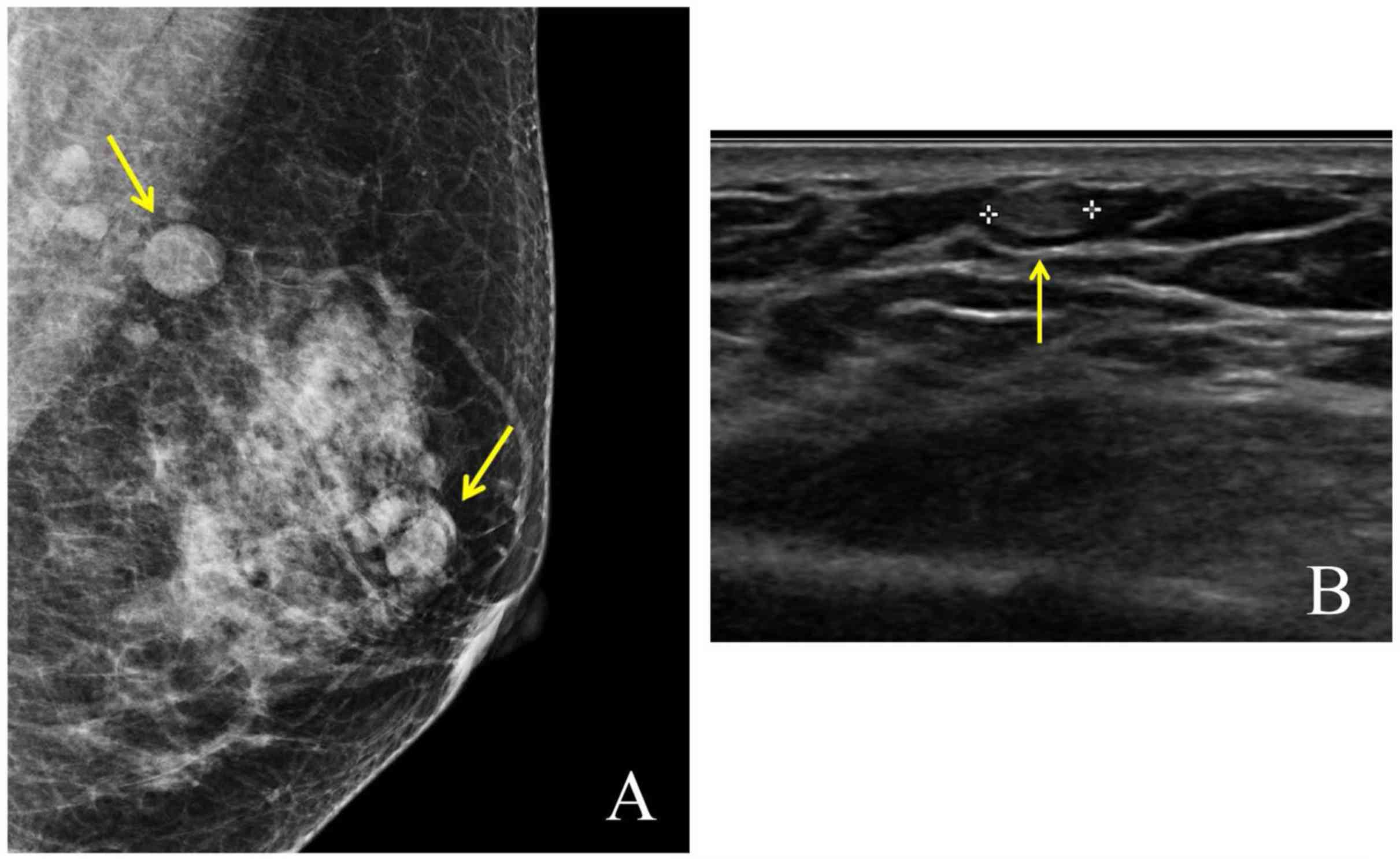
However, a recent radiological study showed an
increase in the size and area of left breast lesion. Radiological
breast examination including mammography and ultrasonography
revealed multiple, well-defined, oval nodules in the inner and
upper area measuring less than 1 cm and located in the subcutaneous
fat layer. The lesions revealed segmental distribution and
occasionally increased vascularity, warranting pathologic
confirmation. No abnormal findings were detected in both axillae.
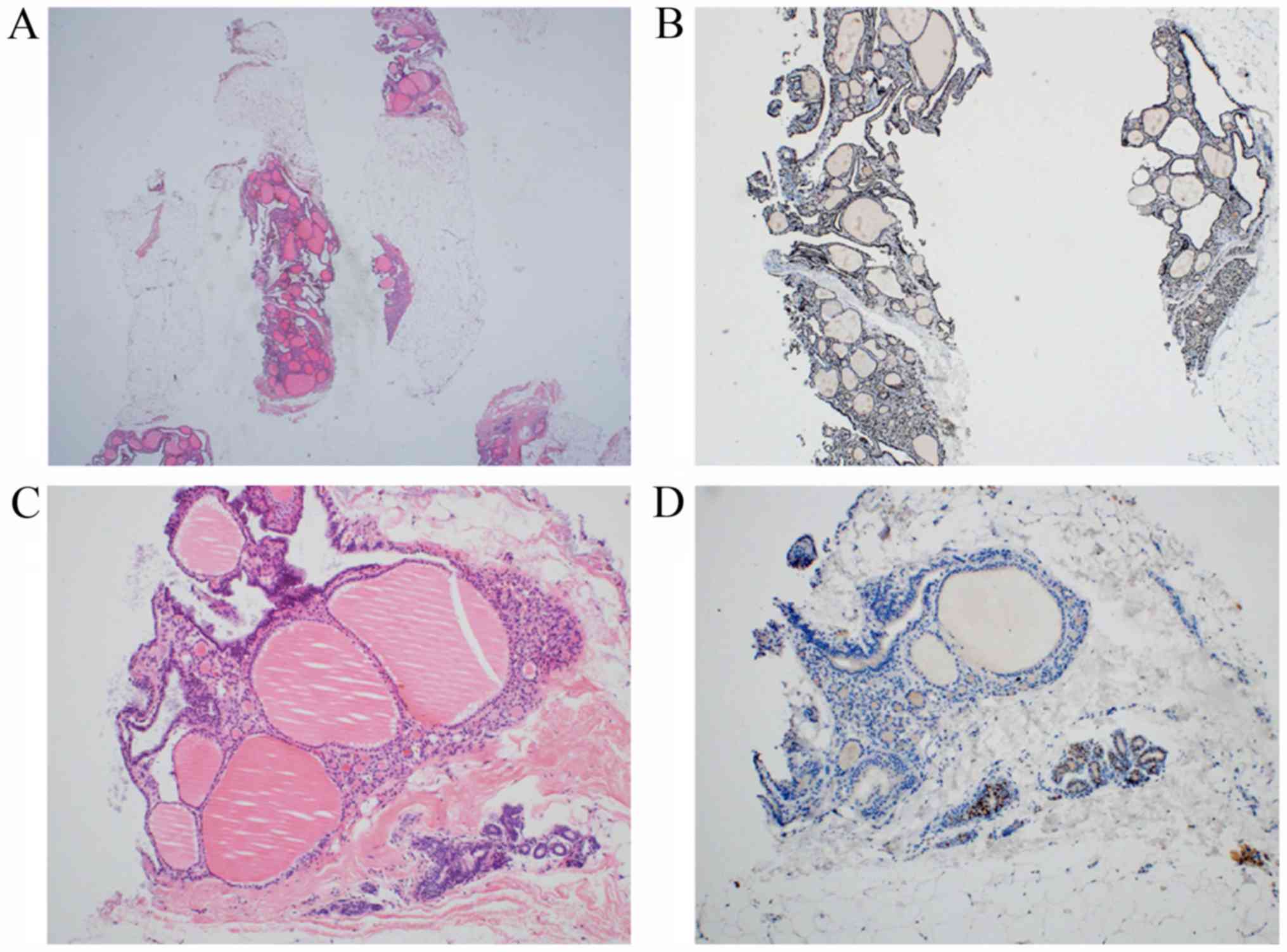
The patient underwent core needle biopsy of the breast lesion to
establish the diagnosis. Five portions of breast tissue, including
the largest one measuring 1.5x1.0 cm, were submitted. Microscopic
evaluation confirmed the presence of thyroid tissue with
predominantly macrofollicular structures, but normal surrounding
breast parenchyma. The thyroid tissue tested positive for thyroid
transcription factor-1 based on immunohistochemistry staining
(Fig. 2). The thyroid function was
normalized after the surgery based on TSH levels of 1.49 µIU/ml,
and free T4 concentrations of 1.18 ng/dl.
Discussion
This is the first reported case of multiple ectopic
thyroid in breast. We found a previous report of thyroidal nodule
in the right breast of a 19-year-old woman (3). However, the patient had a history of
endoscopic right thyroidectomy through breast. Pathology report of
the tissue specimen indicated the presence of follicular tissue at
the drainage incision site and the inner canal. Therefore, the
thyroid nodule in the breast involved grafted thyroid cells at the
drainage incision site. Interestingly, our case patient also had a
history of previous thyroid lobectomy. However, she underwent right
thyroid lobectomy and ectopic thyroid tissue was located in the
left breast. Therefore, the possibility of thyroid tissue implant
in breast during surgery was very low. It was not possible to
compare with similar cases because no other studies reported
multiple ectopic thyroid tissues in the breast.
The most common reason for ectopic thyroid tissue
involved inhibition of migration or excessive descent of the
thyroid anlage. Therefore, it was found along the path of descent
in the developing thyroid primordium from the foramen cecum. The
lingual area was the most common site in about 90% of all cases,
with a majority of the cases associated with the base of tongue
(2). Clinical reports of
extra-lingual ectopic thyroid tissue are rare. We found a few
studies of ectopic thyroid in adrenal gland (4,5),
gallbladder (6), jejunum (7) and mesentery (8) but not pure ectopic thyroid in the
breast. The etiology of this abnormality is not fully understood.
However, genetic factors and mutations in the regulatory genes
expressed in the developing thyroid have been implicated in human
thyroid ectopy (2,9). Ectopic thyroid tissue in the breast is
rare and is difficult to explain based on abnormal migration as it
is distant from the path of embryological development.
The treatment of ectopic thyroid tissue depends on
factors such as mass size, symptoms, age of the patient, thyroid
functional status and histological findings (10). Surgical excision is often the
treatment of choice in symptomatic cases, and other options include
hormone suppression and radioactive iodine-131 ablation (11) based on the different factors. In this
case, iodine-131 scan was not carried out because right
thyroidectomy was performed and the opposite thyroid lobe remained.
Hypothyroidism occurs in about 33% of patients with ectopic thyroid
tissue and euthyroidism has been reported in 61% of such patients
(9). The difference in thyroid
function status may be attributed to heterogeneous age distribution
and location of ectopic thyroid tissue. Hypothyroidism was
prevalent in the lingual area with a lower mean age and without an
eutopic thyroid (9). The majority of
patients are generally asymptomatic while a few cases are detected
incidentally. Symptoms are usually related to the size and location
of the ectopic tissue as well as associated endocrine
dysfunction.
It is also important to distinguish metastases from
thyroid carcinoma. Distant metastases of differentiated thyroid
carcinomas have been reported anywhere. A previous study reported
multiple ectopic thyroids in the lung, which might be confused with
pulmonary metastasis (12). Multiple
ectopic thyroids may be considered in a patient with a history of
thyroid carcinoma. However, our patient did not have a cancer
history and the thyroid tissue in breast showed normal follicular
pattern and cells.
Despite the lack of standard therapy for ectopic
thyroid in breast due to its rarity, further surgical treatment was
not considered because the patient did not exhibit thyroid
hormone-related symptoms. Although ectopic thyroid tissue is
benign, it has a tendency to show enlargement and manifest
compression symptoms. In addition, the possibility of carcinomatous
transformation such as papillary carcinoma arising in struma ovarii
should be considered. Therefore, a regular follow-up is
important.
According to the literature review, this is the
first case of ectopic thyroid tissue in the breast, which
underscores the significance of our report. Additional cases and
further discussion are needed to develop an appropriate treatment
protocol or intervention.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
KC is acquired the data, performed the literature
review and wrote the manuscript. AM, HSK, SID acquired the data and
contributed clinical advice. AM evaluated the images and SID
evaluated the specimens. All authors read and approved the final
manuscript.
Ethics and consent to participate
Not applicable.
Patient consent for publication
Informed consent was obtained from the patient about
the publication of the case details and any associated images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Williams ED, Toyn CE and Harach HR: The
ultimobranchial gland and congenital thyroid abnormalities in man.
J Pathol. 159:135–141. 1989.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Ibrahim NA and Fadeyibi IO: Ectopic
thyroid: Etiology, pathology and management. Hormones (Athens).
10:261–269. 2011.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ye MN, Zhang WH, Yuan YX, Zhang XY and
Chen HF: Thyroid nodule of the breast. Breast J. 22:240–243.
2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Casadei GP, Bertarelli C, Giorgini E,
Cremonini N, de Biase D and Tallini G: Ectopic thyroid tissue in
the adrenal gland: Report of a case. Int J Surg Pathol. 23:170–175.
2015.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Gourmaud J, Bongiovanni M, Triponez F and
Pusztaszeri M: Ectopic thyroid tissue in the adrenal gland. Endocr
Pathol. 25:353–355. 2014.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Cassol CA, Noria D and Asa SL: Ectopic
thyroid tissue within the gall bladder: Case report and brief
review of the literature. Endocr Pathol. 21:263–265.
2010.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Hammers YA, Kelly DR, Muensterer OJ,
Hardin WD Jr, Saeed SA and Mroczek-Musulman EC: Giant polypoid
gastric heterotopia with ectopic thyroid tissue: Unusual cause of
jejuno-jejunal intussusception. J Pediatr Gastroenterol Nutr.
45:484–487. 2007.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Güngör B, Kebat T, Ozaslan C and Akilli S:
Intra-abdominal ectopic thyroid presenting with hyperthyroidism:
Report of a case. Surg Today. 32:148–150. 2002.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Zheng W, Tan J and Liu T: Coexistence of
non-functional ectopic thyroid tissue and a normal thyroid: A case
report. Exp Ther Med. 6:1059–1061. 2013.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Guerra G, Cinelli M, Mesolella M, Tafuri
D, Rocca A, Amato B, Rengo S and Testa D: Morphological, diagnostic
and surgical features of ectopic thyroid gland: A review of
literature. Int J Surg. 12 (Suppl 1):S3–S11. 2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Rahalkar M, Rahalkar A and Solav S: A rare
case of triple thyroid ectopia. Indian J Endocrinol Metab.
18:238–240. 2014.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Ryu HS, Chung YJ, Chong S and Lee JI:
Ectopic intrapulmonary thyroid tissue mimicking metastatic tissue.
Thyroid. 22:755–759. 2012.PubMed/NCBI View Article : Google Scholar
|