1. Introduction
Mammary microcalcifications (MCs) are deposits
<0.5 mm in diameter within the breast tissue. This radiological
feature was first described by Albert Salomon, a German surgeon who
imaged >3,000 surgical specimens in an attempt to describe the
association of MCs with breast cancer and tumor spread to lymph
nodes (1). In diagnostic
mammograms, MCs were first described in 1951 and became
progressively crucial in cancer detection. Currently, 30-50% of
non-palpable breast cancers are detected solely by MCs revealed by
mammography (2-4).
The presence of MCs in mammograms strongly suggests
premalignant or malignant lesions. The type and composition of MCs
are crucial for risk stratification. For example, pleomorphic or
fine linear MCs are strongly associated with malignancy, as
demonstrated in a meta-analysis involving >10,000 patients
(5).
Most breast calcifications are dystrophic and appear
in the terminal ductal-lobular units, and they associated with
various pathological processes, such as fluid collections in cysts,
inflammation, infection, and benign or malignant tumors (6,7). The
aim of the present review was to provide details regarding the
types of MCs and associated radiological and pathological aspects,
in order to provide insights and practical approaches to the topic,
including specific clinical scenarios.
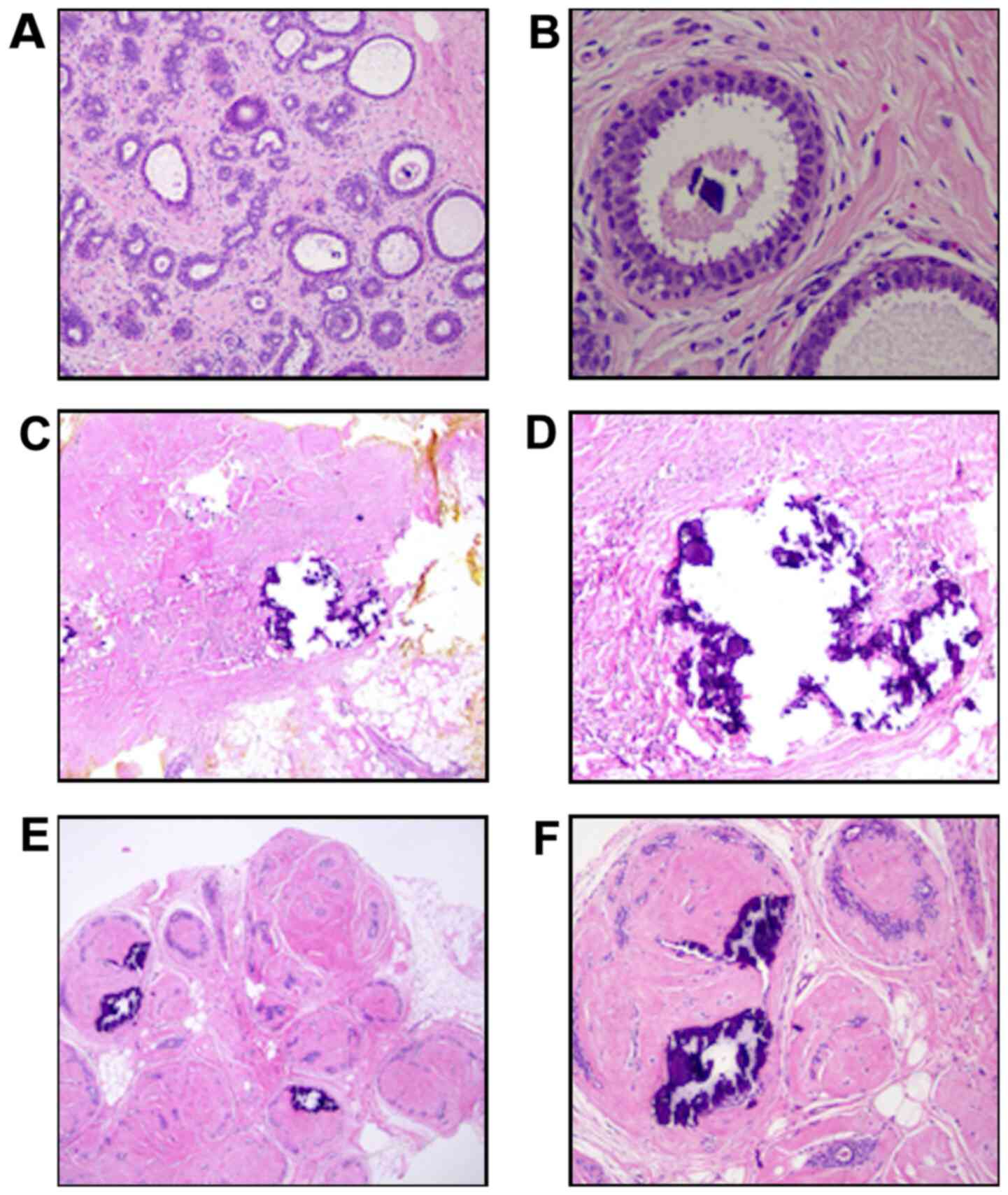
2. Microscopic localization of MCs
Histologically, MCs are calcium-related deposits in
the mammary ductal-lobular units associated with an epithelial
component, such as microcystic adenosis, sclerosing adenosis,
cystic lesions and proliferative lesions (6). MCs may also be entrapped within a
mesenchymal component, either in the stroma (stromal reaction
within a malignant tumor) or they may appear as fibrous lesions
with a connective component (fibroadenoma), a fibrotic healing
process, or steatonecrosis (Fig.
1) (6).
At the biochemical level, MCs are generally
classified into two main types: Type I, composed of calcium oxalate
(CO), and type II, composed of hydroxyapatite (HA). The
classification is based on chemical composition and mammographic
characteristics, including morphology, distribution and density
(Table I) (8-10).
The difference between types is significant because evidence
suggests that type II is often associated with malignant lesions
(11).
 | Table IDescription of differences among type
I, II and Mg-HA of MCs according to distinct features. |
Table I
Description of differences among type
I, II and Mg-HA of MCs according to distinct features.
| Features of
MCs | Type I | Type II | Mg-HA | Refs. |
|---|
| Composition | CO
(CaC2O42H2O) | Calcium HA
[Ca10(PO4)6(OH)2] | Mg-HA
[Mg10(PO4)6(OH)2] | (8) |
| Association with
lesions | Benign disease | Benign and
malignant disease | Mostly malignant
disease | (8) |
| Carbonate | Not present | More carbonate in
the malignant the lesion | Data not
available | (9) |
| Color in optical
microscopy | Amber or
transparent | Opaque,
grey/white | Opaque,
grey/white | (9) |
| Birefringence in
polarized light microscopy | Birefringent |
Non-birefringent |
Non-birefringent | (9) |
| Experimental effect
in breast cancer cell lines | Not capable of
inducing motility | Capable of inducing
motility | Data not
available | (13) |
CO is produced by apocrine cells in the breast and
is frequently associated with benign breast tissue alterations. CO
cannot be metabolized by mammalian cells, and evidence suggests
that its presence may metabolically affect epithelial cells, as it
was shown to induce proliferation and c-Fos overexpression in MCF-7
cells (12).
Type II MCs may be associated with benign and
malignant breast entities; they are present in a wide range of
benign entities, such as fibroadenomas, fibroadenosis and
sclerosing adenosis, and may be partially attributed to two
mechanisms that are also associated with malignant invasive cancer
in experimental models, namely necrosis and fibrosis (9,13).
Collagen type I is commonly associated with osteogenesis, and it is
a significant component of benign nodular lesions, such as
fibroadenomas and areas of fibroadenomatoid changes. Indeed,
detection of type II collagen in these lesions is common in
clinical practice (10).
Another morphological feature present in benign as
well as malignant entities is macrophage recruitment. It has been
reported that tumor-associated macrophages (TAMs) that secrete
cytokines play a pivotal role in MCs. Cysts, areas exhibiting
damage, such as adiponecrosis or inflammation, and previous
surgical procedures are associated with MCs and they are usually
densely infiltrated with macrophages (14).
Recently, a novel third biochemically distinct form
of MC has been described as magnesium-substituted HA (Mg-HA). Mg-HA
and type II MCs are robustly associated with malignancy (15). Scimeca et al (15) observed that CO MCs were associated
with benign lesions in 81.8% of the cases (18 of 22), whereas 97.7%
(43 of 44) of malignant lesions displayed complex forms of MCs,
primarily composed of a different form of HA, namely Mg-HA; this
form was present only in malignant lesions (23 of 44).
3. Etiology of MCs
Dystrophic calcification is traditionally considered
a passive feature associated with cell degeneration and necrosis
and, therefore, is considered to be a passive and unspecific
process (16). However, breast MCs
are under pathophysiological scrutiny. While type I MCs are usually
associated with cysts or fat necrosis (a representative example of
passive deposits), type II MCs are more frequently associated with
abnormal epithelial cells (16).
Bone HA deposition represents an active
cell-mediated process (17) and is
part of physiological mineralization. However, breast MCs occur
outside the skeleton and, therefore, are considered to represent a
pathological mineralization process. Moreover, evidence suggests
that MCs may be regulated similarly to physiological bone
mineralization. Mineralization also occurs in apoptotic cells and
vesicles found in the intracellular and extracellular matrices
(18). The latter is the most
common source of breast MCs, suggesting that mammary MC formation
is an active secretory rather than a passive process, such as in
degeneration or necrosis (19,20).
When MCs are associated with epithelial cells, it is
possible that, under specific circumstances, a subpopulation of
epithelial breast cells may undergo epithelial-to-mesenchymal
transition (EMT) and then switch to osteoblast-like phenotypes
(21). In concordance to this
rationale, other reports demonstrated that the expression of
certain osteogenic proteins, such as osteopontin and bone
morphogenetic protein 2, is upregulated in breast cancer (22-27).
While these osteogenic features are well-documented
in invasive breast cancer and in breast cancer cell lines in
vitro, the reports on EMT features are scarce; changes related
to mineralization and osteogenic model were reported in
proliferative and precursor epithelial lesions associated with MCs
(15). Although discrimination
according to biochemical properties could improve the predictive
value of MCs in mammograms, this requires biopsies providing
sufficient samples for chemical determination, and this procedure
is currently designed for diagnostic purposes only. An improvement
in this setting would be using mass spectrometry profile from
fine-needle aspiration samples (28,29).
Unlike type I MCs, type II MCs may also be
associated with malignant entities; therefore, the presence of
casting-type HA MCs raises suspicion. The problem is that HA MCs
are also frequently associated with benign entities (30,31).
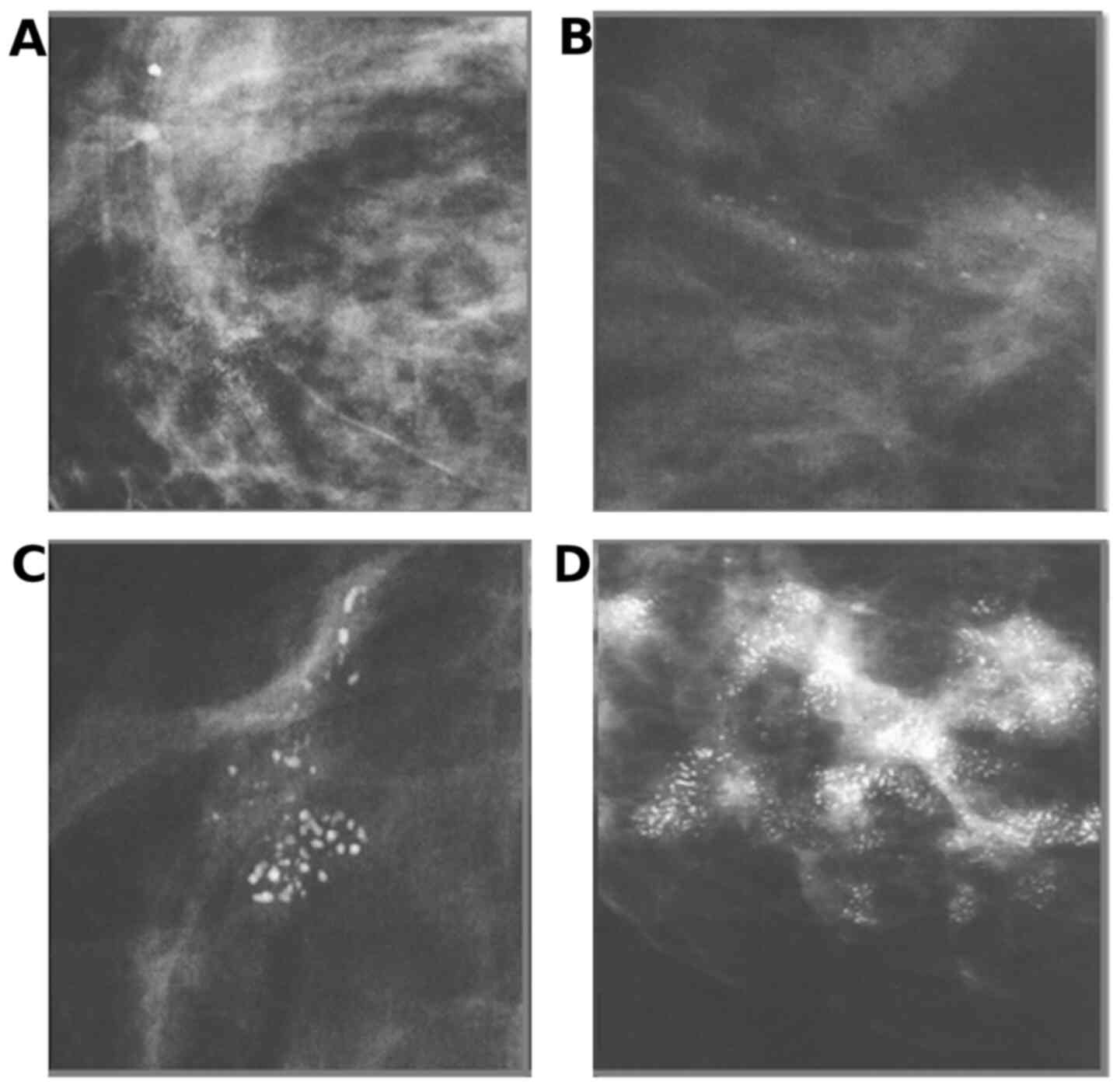
4. Radiological classification of MCs
MCs are commonly seen on mammograms and, therefore,
there are well-described radiological patterns that help
distinguish benign from potentially malignant calcifications
(32). According to the fifth
edition of the Breast Imaging Reporting and Data System (BI-RADS),
MCs are classified as benign and suspicious. Benign calcifications
on mammography are typically more extensive, coarser, rounder with
smooth margins, and more easily seen than malignant calcifications
(Fig. 2; Table II). Calcifications associated with
malignancy are usually small in size and often require
magnification to be well-visualized. MCs must be described
according to morphology and distribution (33).
| Table IIDistinct features of typical benign
and malignant-related MCs in mammograms. |
Table II
Distinct features of typical benign
and malignant-related MCs in mammograms.
|
Characteristics | Benign breast
lesions | Malignant breast
lesions |
|---|
| MCs | Spaced | Compact
clusters |
| Amount of
carbonate | Higher | Lower |
| Shape | Ring-shaped | Vermicular,
casting-type |
| Protein
matrix/mineral ratio | High | Low |
| Rate of Mg
substitution | Lower | Higher |
Suspicious morphology includes coarse heterogeneous
appearance, amorphous nature, fine pleomorphic elements, and fine
linear branching calcifications. The risk of malignancy of each
descriptor are 13, 27, 50 and 78%, respectively (Fig. 3). The five distribution categories
are diffuse, segmental, regional, grouped and linear (5).
Calcifications are extremely frequent alterations
seen in 80% of mammograms, they mostly reflect a benign process and
are not associated with cancer. However, when they present as small
particles (MCs), grouped and polymorphic, they may be associated
with malignancy (34-36).
Mammography is the main modality used to evaluate these
alterations. MRI has shown encouraging data in the diagnosis of
breast cancer; however, its role in the evaluation of MCs remains
under study, most likely because of low-grade lesions that exhibit
little angiogenesis. Breast ultrasonography was also shown to lack
the ability to detect MCs, as breast nodules are the lesions most
often identified using ultrasonography (34-36).
5. MC management and biopsy with
radiological guidance
MCs represent a challenge in terms of detection and
interpretation. Small, grouped MCs are easy to miss and difficult
to interpret. When MCs do not exhibit benign features on screening
mammography, the patient must be recalled for assessment using
alternative mammogram views (32,34).
Final radiological evaluation leads to three possibilities: i) On
magnified or supplementary views, MCs may be considered typically
benign and classified as BI-RADS 2, and then follow-up is
recommended; ii) MCs that are rounded and grouped may be classified
as BI-RADS 3, and another imaging 6 months later for re-evaluation
of stability is sufficient; and iii) when MCs exhibit suspicious
morphological characteristics, they are classified as BI-RADS 4,
and stereotactic biopsy is recommended (33).
Breast image-guided biopsies vary immensely
technically. The size of the biopsy needle varies according to
local protocols, device availability and indications on a
case-by-case basis. Open excision is the final option, and the most
frequent diagnostic procedure employed worldwide is a core biopsy.
More recently, vacuum-assisted breast biopsy (VABB) has become more
common (32,37). Core biopsies are usually performed
using a 14G needle, which may be helpful to establish a benign
diagnosis, such as microcystic or fibroadenomatoid change, or a
malignant diagnosis of invasive cancer; however, this method may
underestimate the nature of the disease in ~27% of cases when
ductal carcinoma in situ (DCIS) and indeterminate lesions,
such as atypia, are present (32,37).
VABB uses a large caliber device ranging from 7 to
12G. In most cases, a 14G biopsy is sufficient to make the
diagnosis; exceptions are made when there are very small (<5 mm)
or scattered microcalcified clusters, and VABB is preferred in the
first instance (32,34). In cases of MCs >10 mm in size, a
core needle biopsy can be used alternatively (35,36).
When MCs are detected only on mammography or in
non-nodular lesions, they usually require stereotactic guidance to
ensure a safe biopsy procedure, proper investigation of MCs, and
provide high-quality samples (38). The number and width of the
fragments are larger, comparable to samples obtained in surgical
procedures (32), and MCs are
easily retrieved according to Meyer et al (39). Standard automated needle devices
were able to retrieve MCs within the sample in 90.8% of the cases
compared with 95-100% in samples extracted using a vacuum-assisted
device (11,39). This procedure allows pathologists
to gain access to more tissue for analysis, improving diagnostic
accuracy. It is estimated that at least two cores with at least
five calcium specks are sufficient (38).
The false-negative rate with VABB is low, and the
correlation with final diagnosis is high, although there remains
some degree of underestimation (~12%). Consequently, the likelihood
of subsequent alteration in the grade of the lesion on follow-up is
minimal. This procedure also has the advantage of achieving a
definitive diagnosis with a single pass, reducing the duration of
the procedure, as the needle is introduced only once and the
samples are large in volume (38).
Other advantages are the allowance for placement of
a titanium marker at the biopsy site and a lower diagnostic
underestimation rate compared with core needle biopsy (39). Although vacuum-assisted large core
biopsy provides a number of benefits, its cost is substantially
greater compared with that of a 14G biopsy. Furthermore, this
device is not yet available in many countries and underdeveloped
regions. The surgical approach using segmental excision remains the
only alternative in several facilities worldwide. In such cases,
surgical and pathological management are crucial for determining
the presence of MCs within the parenchyma (32,41).
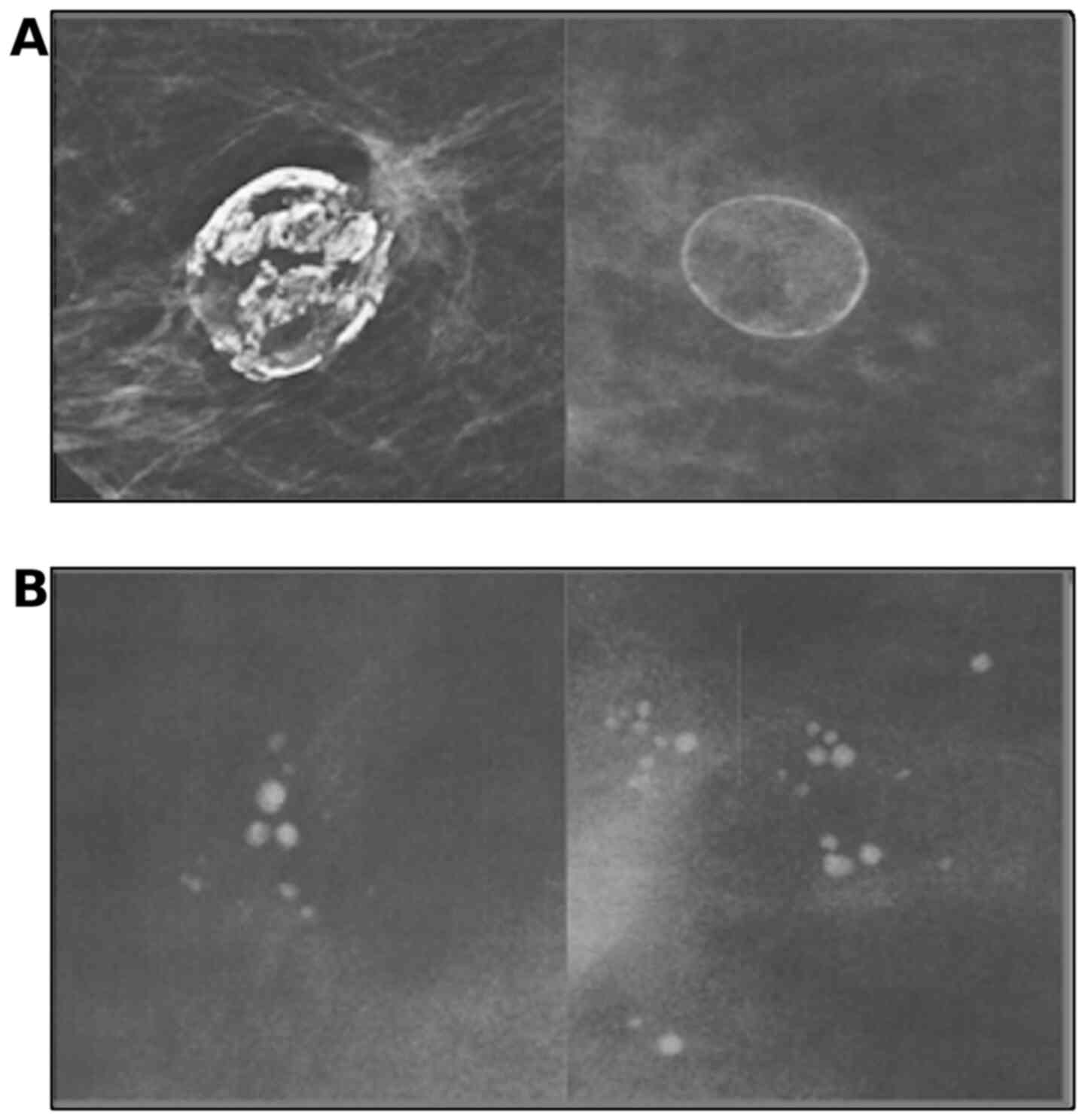
6. Sending MC specimens to the pathology
laboratory
It is crucial to obtain X-ray images of all
fragments obtained from breast biopsies for MC evaluation in order
to select those with MCs; the presence, size and morphology of the
MCs should match the mammography findings (Fig. 4A). Once the fragments containing
MCs are identified on X-ray, it is usually recommended to keep the
affected fragments in vials separate from the others. If possible,
it is advisable to send the original X-ray image taken from the
fragments along with the samples to the pathology laboratory. This
procedure is meant to help the pathologist identify MCs and
determine which lesions are associated with them (38).
Pathological management and report of
MC-related lesions
In this setting, the pathologist will receive two
vials from the same breast lesion, one containing fragments with
MCs and the other containing the remaining fragments (supposedly
without MCs). These should be distinct paraffin-embedded blocks
with separate slides. It is important to remember that, although
the fragments are sent to the pathologist separately, they
originate from the same region or lesions and should be assessed as
a single lesion with a primary diagnosis. The findings are usually
combined in one conclusion, as there may be some confusion when
patients and, possibly, generalist physicians are confronted with
the dichotomy of two distinct (and sometimes opposite) findings in
the final report, since fragments without MCs often do not contain
morphological indications of any malignant lesion.
It is crucial to identify MCs and report their
presence in the pathology report, as it assures that the biopsied
area was the actual target of the examination. When possible, it
should be confirmed whether MCs are irregular or birefringent,
delicate MCs. When the fragments labeled as ‘with MCs’ are
microscopically analyzed, it may be the case that MCs are not
easily identifiable, as they may lie deeper in the paraffin block,
or they may be lost during sample processing, while certain
technical measures mentioned below may resolve this problem
(42).
Asking for subsequent sections of the block may be
recommended, particularly if the lesion appears to be benign or if
it must be ascertained that the area of the MCs was sampled
appropriately. For suspicious lesions, caution must be taken when
leveling the block, as some of the putative lesion may be lost, or
later immunohistochemical evaluation may be compromised (43).
Large cysts with fluid secretion and benign entities
commonly display irregular cavities, such as scar tissue and fat
necrosis secretions associated with MCs, that disappear on
histological examination. This may be due to the fact that they are
lost during histological section preparation, because the MCs may
not be rigidly attached to the tissues; therefore, after
sectioning, they may no longer be identifiable on hematoxylin and
eosin-stained slides. When even deeper levels fail to demonstrate
the remaining MCs in this scenario, an X-ray of the blocks may be
requested (Fig. 4B). The paraffin
block X-rays may reveal the MCs and ensure that the tissue sampled
and embedded on the block in question is the targeted one, and if
the paraffin block X-ray image does not reveal any MCs, the
conclusion is that they were likely lost during processing. A
caution note must be included in the report when this is the case,
so that clinicians can double-check by performing a post-procedure
mammogram to determine whether the targeted MCs were removed
entirely (38,39).
An alternative that may be very useful is to examine
the hematoxylin and eosin-stained slides obtained under polarized
light, which may reveal evidence of type I MCs. It is crucial to
remember that type I MCs are often associated with benign lesions,
and any suspicion of malignancy must be checked out by performing
detailed assessment and correlation with radiological aspects of
the MCs (6,8)
In addition, locating the MCs may not always be the
most significant challenge; instead, the challenge may lie with
defining lesions according to width. Pleomorphic calcifications may
be the only remaining feature of a previous DCIS lesion.
Occasionally, DCIS may undergo regression with fibrosis and
elastosis, and it may be challenging to locate viable epithelial
cells to achieve a definitive diagnosis (6,8).
Large fibrotic ducts with no apparent epithelial covering must be
interpreted as suspicious if associated with significant central
MCs. Subsequent levels of the block may reveal a suitable layer of
representative ductal cells and facilitate the assessment (6,8).
7. MCs in breast cancer
MCs are associated with premalignant and
proliferative breast disease, and their identification facilitates
the prevention of invasive disease. MCs may play a prognostic role
in invasive carcinomas. Carcinomas with MCs appear to have worse
outcomes compared with those without MCs (45). Furthermore, fine linear branching
MCs have been associated with worse outcomes compared with
non-linear MCs (3,31,42,43).
In invasive carcinomas, the presence of MCs confers
worse outcome in terms of parameters such as 8-year survival rate,
tumor width and lymph node involvement (45). Since Tabár et al (46) examined the possible prognostic role
of MCs in invasive breast cancer in 2000, several contributions
have accumulated robust evidence to suggest that the presence of
MCs, particularly those of the casting-type morphology in invasive
breast cancer, is associated with poor outcome, higher risk of
mortality, propensity for recurrence and HER-2-positive status.
Among these studies are robust meta-analyses pooling odds ratios
from more extensive series (47-49).
These concepts may shed light on the substantial
importance of identifying MCs within an invasive tumor on
pathological reports, even when doing so does not appear to be
relevant information in the context of an already invasive nodular
lesion. Since the presence, composition and type of MCs in breast
lesions may influence the outcome, it is crucial that the presence
and morphological characteristics of MCs are accurately reported to
direct appropriate treatment decision-making. Some challenging
prospective clinical studies in low-grade and intermediate-grade
DCIS (such as LORIS, LORD and COMET) are testing the hypothesis of
conservative treatment alternatives for such lesions (11,47-49).
8. MCs in specific clinical scenarios
MCs in high-density breast tissue
Diffusely dense breasts may be challenging to
analyze on mammography, and some efforts have been made to improve
the visualization of MCs on ultrasound imaging. However, the poor
reproducibility of this method and limitations inherent to
ultrasonic detection systems remain impediments to adequate
implementation (50).
MCs in young patients
As most screening guidelines generally exclude women
aged <40 years, few studies have verified the characteristics of
breast MCs in young patients. This is more frequent in Asia.
Fushimi et al (51)
reviewed 403 mammograms from patients younger than 40 years and
compared them to older patients (aged 40-74 years). Women aged
<40 years were more likely to be recalled for MCs rather than
for nodular lesions. The most frequent MC forms were small round
and segmental MCs.
MCs in male breasts
In men, breast lesions are usually radiographically
examined after the appearance of clinical symptoms and, therefore,
MCs are not the first sign as in screening mammograms in women.
Breast lesions in men were found to be associated with MC in 29% of
cases reported by Mathew et al (52). However, they are not typically the
main index of suspicion. In men, MCs are associated with benign as
well as malignant lesions and they are less numerous, coarser and
rounder compared with those in female breast tissue. Fat necrosis
after trauma is a common benign cause associated with dystrophic
MCs in men (52).
MCs in the neoadjuvant setting
Invasive carcinomas with and without in situ
components may contain MCs associated with the extension of the
original lesion; however, these are not a reliable source of
information regarding the amount of viable tumor tissue following
neoadjuvant therapy. According to the tumor response to neoadjuvant
treatment and the presence of necrosis and fibrosis, the number and
extent of MCs may remain stable, decrease, or sometimes even
increase (52,53). Previous studies concluded that the
pattern of MCs after neoadjuvant therapy on mammography and MRI
examination tended to overestimate the true extent of the remaining
pathological lesion (52,53).
Most authors have found no significant association
between complete pathological response and MC patterns following
neoadjuvant therapy. There is also evidence of MCs being associated
with benign changes in this setting (54). As a result, complete excision of
all indeterminate or suspicious calcifications remains the standard
practice (55).
9. Conclusions
The importance of MCs in cancer detection has become
apparent over the last 20 years. With novel digital and
technological detection methods being made available, the
percentage of detected cases bearing MCs has increased. Currently,
30-50% of non-palpable breast cancers are detected solely by MC
identification on mammography (2-4).
However, MCs represent a challenge regarding detection and
interpretation. Therefore, radiological and pathological
evaluations and expertise in pathoradiological correlations are
crucial for accurately diagnosing these lesions. Contributions in
this field are crucial to enhance the accuracy of the
interpretation of radiological and pathological findings. The type
and composition of MCs, including determination of their
biochemical nature, could improve their predictive value. Novel
potential markers of malignancy in breast lesions may be uncovered
from the MC profile in the future.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
AFL designed the study and wrote the manuscript.
KCKP and CCBAN contributed to manuscript writing, images and
tables. AFVF critically reviewed the manuscript for important
intellectual content. MSDAC edited the information regarding the
association of the context of the radiological reports. All the
authors have read and approved the final version of the manuscript.
AFL and AFVF confirm the authenticity of all the raw data of the
paper.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Salomon A: Beiträge zur Pathologie und
Klinik der Mammo-karzinome (In German). Arch Klin Chir.
101:573–668. 1913.
|
|
2
|
Leborgne R: Diagnosis of tumors of the
breast by simple roentgenography; calcifications in carcinomas. Am
J Roentgenol Radium Ther. 65:1–11. 1951.PubMed/NCBI
|
|
3
|
Gülsün M, Demirkazik FB and Ariyürek M:
Evaluation of breast microcalcifications according to Breast
Imaging Reporting and Data System criteria and Le Gal's
classification. Eur J Radiol. 47:227–231. 2003.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Venkatesan A, Chu P, Kerlikowske K,
Sickles EA and Smith-bindman R: Positive predictive value of
specific mammographic findings according to reader and patient va
riables. Radiology. 250:648–657. 2009.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Rominger M, Wisgickl C and Timmesfeld N:
Breast microcalcifications as type descriptors to stratify risk of
malignancy: A systematic review and meta-analysis of 10665 cases
with special focus on round/punctate microcalcifications. Rofo.
184:1144–1152. 2012.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Sharma T, Radosevich JA, Pachori G and
Mandal CC: A Molecular View of Pathological Microcalcification in
Breast Cancer. J Mammary Gland Biol Neoplasia. 21:25–40.
2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Henrot P, Leroux A, Barlier C and Génin P:
Breast microcalcifications: The lesions in anatomical pathology.
Diagn Interv Imaging. 95:141–152. 2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Frappart L, Boudeulle M, Boumendil J, Lin
HC, Martinon I, Palayer C, Mallet-Guy Y, Raudrant D, Bremond A,
Rochet Y, et al: Structure and composition of microcalcifications
in benign and malignant lesions of the breast: Study by light
microscopy, transmission and scanning electron microscopy,
microprobe analysis, and X-ray diffraction. Hum Pathol. 15:880–889.
1984.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Haka AS, Shafer-Peltier KE, Fitzmaurice M,
Crowe J, Dasari RR and Feld MS: Identifying microcalcifications in
benign and malignant breast lesions by probing differences in their
chemical composition using Raman spectroscopy. Cancer Res.
62:5375–5380. 2002.PubMed/NCBI
|
|
10
|
Trop I, David J, El Khoury M, Gautier N,
Gaboury L and Lalonde L: Microcalcifications around a
collagen-based breast biopsy marker: Complication of biopsy with a
percutaneous marking system. AJR Am J Roentgenol. 197:W353–357.
2011.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Liberman L, Smolkin JH, Dershaw DD, Morris
EA, Abramson AF and Rosen PP: Calcification retrieval at
stereotactic, 11-gauge, directional, vacuum-assisted breast biopsy.
Radiology. 208:251–260. 1998.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Castellaro AM, Tonda A, Cejas HH, Ferreyra
H, Caputto BL, Pucci OA and Gil GA: Oxalate induces breast cancer.
BMC Cancer. 15(761)2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Radi MJ: Calcium oxalate crystals in
breast biopsies. An overlooked form of microcalcification
associated with benign breast disease. Arch Pathol Lab Med.
113:1367–1369. 1989.PubMed/NCBI
|
|
14
|
Shih C, Padhy LC, Murray M and Weinberg
RA: Transforming genes of carcinomas and neuroblastomas introduced
into mouse fibroblasts. Nature. 290:261–264. 1981.PubMed/NCBI View
Article : Google Scholar
|
|
15
|
Scimeca M, Giannini E, Antonacci C,
Pistolese CA, Spagnoli LG and Bonanno E: Microcalcifications in
breast cancer: An active phenomenon mediated by epithelial cells
with mesenchymal characteristics. BMC Cancer.
14(286)2014.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Morgan MP, Cooke MM and McCarthy GM:
Microcalcifications associated with breast cancer: An epiphenomenon
or biologically significant feature of selected tumors? J Mammary
Gland Biol Neoplasia. 10:181–187. 2005.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Owen TA, Aronow M, Shalhoub V, Barone LM,
Wilming L, Tassinari MS, Kennedy MB, Pockwinse S, Lian JB and Stein
GS: Progressive development of the rat osteoblast phenotype in
vitro: Reciprocal relationships in expression of genes associated
with osteoblast proliferation and differentiation during formation
of the bone extracellular matrix. J Cell Physiol. 143:420–430.
1990.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Huang W, Yang S, Shao J and Li YP:
Signaling and transcriptional regulation in osteoblast commitment
and differentiation. Front Biosci. 12:3068–3092. 2007.PubMed/NCBI View
Article : Google Scholar
|
|
19
|
Hassan MQ, Maeda Y, Taipaleenmaki H, Zhang
W, Jafferji M, Gordon JA, Li Z, Croce CM, van Wijnen AJ, Stein JL,
et al: miR-218 directs a Wnt signaling circuit to promote
differentiation of osteoblasts and osteomimicry of metastatic
cancer cells. J Biol Chem. 287:42084–42092. 2012.PubMed/NCBI View Article : Google Scholar
|
|
20
|
O'Grady S and Morgan MP:
Microcalcifications in breast cancer: From pathophysiology to
diagnosis and prognosis. Biochim Biophys Acta Rev Cancer.
1869:310–320. 2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Menck K, Scharf C, Bleckmann A, Dyck L,
Rost U, Wenzel D, Dhople VM, Siam L, Pukrop T, Binder C, et al:
Tumor-derived microvesicles mediate human breast cancer invasion
through differentially glycosylated EMMPRIN. J Mol Cell Biol.
7:143–153. 2015.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Abate-Shen C: Deregulated homeobox gene
expression in cancer: Cause or consequence? Nat Rev Cancer.
2:777–785. 2002.PubMed/NCBI View
Article : Google Scholar
|
|
23
|
Davies SR, Watkins G, Douglas-Jones A,
Mansel RE and Jiang WG: Bone morphogenetic proteins 1 to 7 in human
breast cancer, expression pattern and clinical/prognostic
relevance. J Exp Ther Oncol. 7:327–338. 2008.PubMed/NCBI
|
|
24
|
Jin H, Pi J, Huang X, Huang F, Shao W, Li
S, Chen Y and Cai J: BMP2 promotes migration and invasion of breast
cancer cells via cytoskeletal reorganization and adhesion decrease:
An AFM investigation. Appl Microbiol Biotechnol. 93:1715–1723.
2012.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Liu F, Bloch N, Bhushan KR, De Grand AM,
Tanaka E, Solazzo S, Mertyna PM, Goldberg N, Frangioni JV and
Lenkinski RE: Humoral bone morphogenetic protein 2 is sufficient
for inducing breast cancer microcalcification. Mol Imaging.
7:175–186. 2008.PubMed/NCBI
|
|
26
|
Bellahcène A, Merville MP and Castronovo
V: Expression of bone sialoprotein, a bone matrix protein, in human
breast cancer. Cancer Res. 54:2823–2826. 1994.PubMed/NCBI
|
|
27
|
Bellahcène A and Castronovo V: Increased
expression of osteonectin and osteopontin, two bone matrix
proteins, in human breast cancer. Am J Pathol. 146:95–100.
1995.PubMed/NCBI
|
|
28
|
Barman I, Dingari NC, Saha A, McGee S,
Galindo LH, Liu W, Plecha D, Klein N, Dasari RR and Fitzmaurice M:
Application of Raman spectroscopy to identify microcalcifications
and underlying breast lesions at stereotactic core needle biopsy.
Cancer Res. 73:3206–3215. 2013.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Saha A, Barman I, Dingari NC, McGee S,
Volynskaya Z, Galindo LH, Liu W, Plecha D, Klein N, Dasari RR, et
al: Raman spectroscopy: A real-time tool for identifying
microcalcifications during stereotactic breast core needle
biopsies. Biomed Opt Express. 2:2792–2803. 2011.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Cox R: Cellular and molecular basis of
mammary microcalcifications. PhD dissertation, Royal College of
Surgeons in Ireland. https://doi.org/10.25419/rcsi.10804970.v1, 2011.
|
|
31
|
Cox RF and Morgan MP: Microcalcifications
in breast cancer: Lessons from physiological mineralization. Bone.
53:437–450. 2013.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Wilkinson L, Thomas V and Sharma N:
Microcalcification on mammography: Approaches to interpretation and
biopsy. Br J Radiol. 90(20160594)2017.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Sickles EA, D'Orsi CJ and Bassett LW: ACR
BI-RADS Mammography. In: ACR BI-RADS Atlas, Breast Imaging
Reporting and Data System. 5th Edition. American College of
Radiology, Reston, VA, pp134-136, 2013.
|
|
34
|
Uematsu T, Yuen S, Kasami M and Uchida Y:
Dynamic contrast-enhanced MR imaging in screening detected
microcalcification lesions of the breast: Is there any value?
Breast Cancer Res Treat. 103:269–281. 2007.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Bazzocchi M, Zuiani C, Panizza P, Del
Frate C, Soldano F, Isola M, Sardanelli F, Giuseppetti GM,
Simonetti G, Lattanzio V, et al: Contrast-enhanced breast MRI in
patients with suspicious microcalcifications on mammography:
Results of a multicenter trial. AJR Am J Roentgenol. 186:1723–1732.
2006.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Cilotti A, Iacconi C, Marini C, Moretti M,
Mazzotta D, Traino C, Naccarato AG, Piagneri V, Giaconi C,
Bevilacqua G and Bartolozzi C: Contrast-enhanced MR imaging in
patients with BI-RADS 3-5 microcalcifications. Radiol Med.
112:272–286. 2007.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Pfarl G, Helbich TH, Riedl CC, Wagner T,
Gnant M, Rudas M and Liberman L: Stereotactic 11-gauge
vacuum-assisted breast biopsy: A validation study. AJR Am J
Roentgenol. 179:1503–1507. 2002.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Esen G, Tutar B, Uras C, Calay Z, İnce Ü
and Tutar O: Vacuum-assisted stereotactic breast biopsy in the
diagnosis and management of suspicious microcalcifications. Diagn
Interv Radiol. 22:326–333. 2016.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Meyer JE, Smith DN, DiPiro PJ, Denison CM,
Frenna TH, Harvey SC and Ko WD: Stereotactic breast biopsy of
clustered microcalcifications with a directional, vacuum-assisted
device. Radiology. 204:575–576. 1997.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Badan GM, Roveda Júnior D, Piato S, Fleury
EF, Campos MS, Pecci CA, Ferreira FA and D'Ávila C: Diagnostic
underestimation of atypical ductal hyperplasia and ductal carcinoma
in situ at percutaneous core needle and vacuum-assisted biopsies of
the breast in a Brazilian reference institution. Radiol Bras.
49:6–11. 2016.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Houssami N, Ciatto S, Ellis I and
Ambrogetti D: Underestimation of malignancy of breast core-needle
biopsy: Concepts and precise overall and category-specific
estimates. Cancer. 109:487–495. 2007.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Tornos C, Silva E, el-Naggar A and
Pritzker KP: Calcium oxalate crystals in breast biopsies. The
missing microcalcifications. Am J Surg Pathol. 14:961–968.
1990.PubMed/NCBI View Article : Google Scholar
|
|
43
|
D'Orsi CJ, Reale FR, Davis MA and Brown
VJ: Is calcium oxalate an adequate explanation for nonvisualization
of breast specimen calcifications? Radiology. 182:801–803.
1992.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Ling H, Liu ZB, Xu LH, Xu XL, Liu GY and
Shao ZM: Malignant calcification is an important unfavorable
prognostic factor in primary invasive breast cancer. Asia Pac J
Clin Oncol. 9:139–145. 2013.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Bonfiglio R, Scimeca M, Urbano N, Bonanno
E and Schillaci O: Breast microcalcifications: Biological and
diagnostic perspectives. Future Oncol. 14:3097–3099.
2018.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Tabár L, Chen HH, Duffy SW, Yen MF, Chiang
CF, Dean PB and Smith RA: A novel method for prediction of
long-term outcome of women with T1a, T1b, and 10-14 mm invasive
breast cancers: A prospective study. Lancet. 355:429–433.
2000.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Elias SG, Adams A, Wisner DJ, Esserman LJ,
van't Veer LJ, Mali WP, Gilhuijs KG and Hylton NM: Imaging features
of HER2 overexpression in breast cancer: A systematic review and
meta-analysis. Cancer Epidemiol Biomarkers Prev. 23:1464–1483.
2014.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Nyante SJ, Lee SS, Benefield TS, Hoots TN
and Henderson LM: The association between mammographic
calcifications and breast cancer prognostic factors in a
population-based registry cohort. Cancer. 123:219–227.
2017.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Zheng K, Tan JX, Li F, Wei YX, Yin XD, Su
XL, Li HY, Liu QL, Ma BL, Ou JH, et al: Relationship between
mammographic calcifications and the clinicopathologic
characteristics of breast cancer in Western China: A retrospective
multi-center study of 7317 female patients. Breast Cancer Res
Treat. 166:569–582. 2017.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Ouyang YL, Zhou ZH, Wu WW, Tian J, Xu F,
Wu SC and Tsui PH: A review of ultrasound detection methods for
breast microcalcification. Math Biosci Eng. 16:1761–1785.
2019.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Fushimi A, Fukushima N, Suzuki T, Kudo R
and Takeyama H: Features of microcalcifications on screening
mammography in young women. Asian Pac J Cancer Prev. 19:3591–3596.
2018.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Mathew J, Perkins GH, Stephens T,
Middleton LP and Yang WT: Primary breast cancer in men: Clinical,
imaging, and pathologic findings in 57 patients. AJR Am J
Roentgenol. 191:1631–1639. 2008.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Weiss A, Lee KC, Romero Y, Ward E, Kim Y,
Ojeda-Fournier H, Einck J and Blair SL: Calcifications on mammogram
do not correlate with tumor size after neoadjuvant chemotherapy.
Ann Surg Oncol. 21:3310–3316. 2014.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Adrada BE, Huo L, Lane DL, Arribas EM,
Resetkova E and Yang W: Histopathologic correlation of residual
mammographic microcalcifications after neoadjuvant chemotherapy for
locally advanced breast cancer. Ann Surg Oncol. 22:1111–1117.
2015.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Feliciano Y, Mamtani A, Morrow M, Stempel
MM, Patil S and Jochelson MS: Do Calcifications Seen on Mammography
After Neoadjuvant Chemotherapy for Breast Cancer Always Need to Be
Excised? Ann Surg Oncol. 24:1492–1498. 2017.PubMed/NCBI View Article : Google Scholar
|