Cognitive frailty (CF) refers to a heterogeneous
clinical syndrome found in elderly individuals that excludes those
with AD and other types of dementia, and is characterized by
concurrent physical frailty and potentially reversible cognitive
impairment (1). CF includes
reversible and potentially reversible subtypes (2), and may represent a precursor to
neurodegenerative processes. Although studies regarding CF
biomarkers are scarce, the neuropathological processes overlap with
those in individuals with AD and/or other neurodegenerative
diseases, and the final outcomes of CF are AD or non-AD dementia.
Therefore, excluding biomarkers of physical frailty, other
biomarkers, such as amyloid-β (Aβ) accumulation, neurodegeneration
or neuronal injury, may be considered biomarkers for CF. Reversible
CF occurs in the later stages of preclinical AD or at the pre-mild
cognitive impairment (MCI) stage due to other causes, and can be
diagnosed based on subjective cognitive decline (SCD) and/or
positive biomarkers. Cognitive impairment in potentially reversible
CF is comparable to MCI.
Diagnosis of preclinical sporadic AD or other
suspected non-Alzheimer pathologies in reversible CF depends on the
evidence of pathophysiological alterations in the brain, as
demonstrated by established fluid and imaging biomarkers. Neuronal
injury or neurodegeneration-associated biomarkers offer chances to
predict cognitive impairment progression and prognosis, and to
evaluate outcomes of disease-modifying interventions in clinical
trials (3). However, there are
several challenges, including invasive or expensive detection
techniques, and time-consuming detection procedures for the
measurement of current biomarkers for disease-induced early
neuropathological alterations. The most important challenges
associated with current biomarkers are the measurement techniques;
for example, current standard enzyme-linked immunosorbent assay
(ELISA) methods are insensitive to very low concentrations of
biomarkers in cerebrospinal fluid (CSF) and blood (4). Therefore, blood- and urine-based
biomarkers may be more attractive biomarkers for the screening of
neuropathological alterations in AD and CF. The present study
systematically reviewed the advance of fluid biomarkers for the
pathological process of AD, which will likely aid in the discovery
of biomarkers for CF.
A reviewer scrutinized abstracts found by electronic
search in order to identify articles meriting a full review. Entire
articles were reviewed before data were extracted from pertinent
papers.
The inclusion criteria used for the review protocol
were as follows: i) Age ≥60 years, ii) diagnosis of AD according to
the criteria of the National Institute on Aging-Alzheimer's
Association (NIAAA) (7) or
diagnosis of MCI according to NIAAA criteria (8) with a confirmed progression to AD
assessed by clinical follow-up, and iii) suitable clinical
assessments of cognitive and functional impairment, quality of life
and clinical evaluations. The exclusion criteria were: i) No
English editing (as we lacked resources for translation), ii)
diagnosis of non-AD dementia, and iii) MCI that did not progress to
AD. No limits were defined on the grounds of disease duration or
drug treatment.
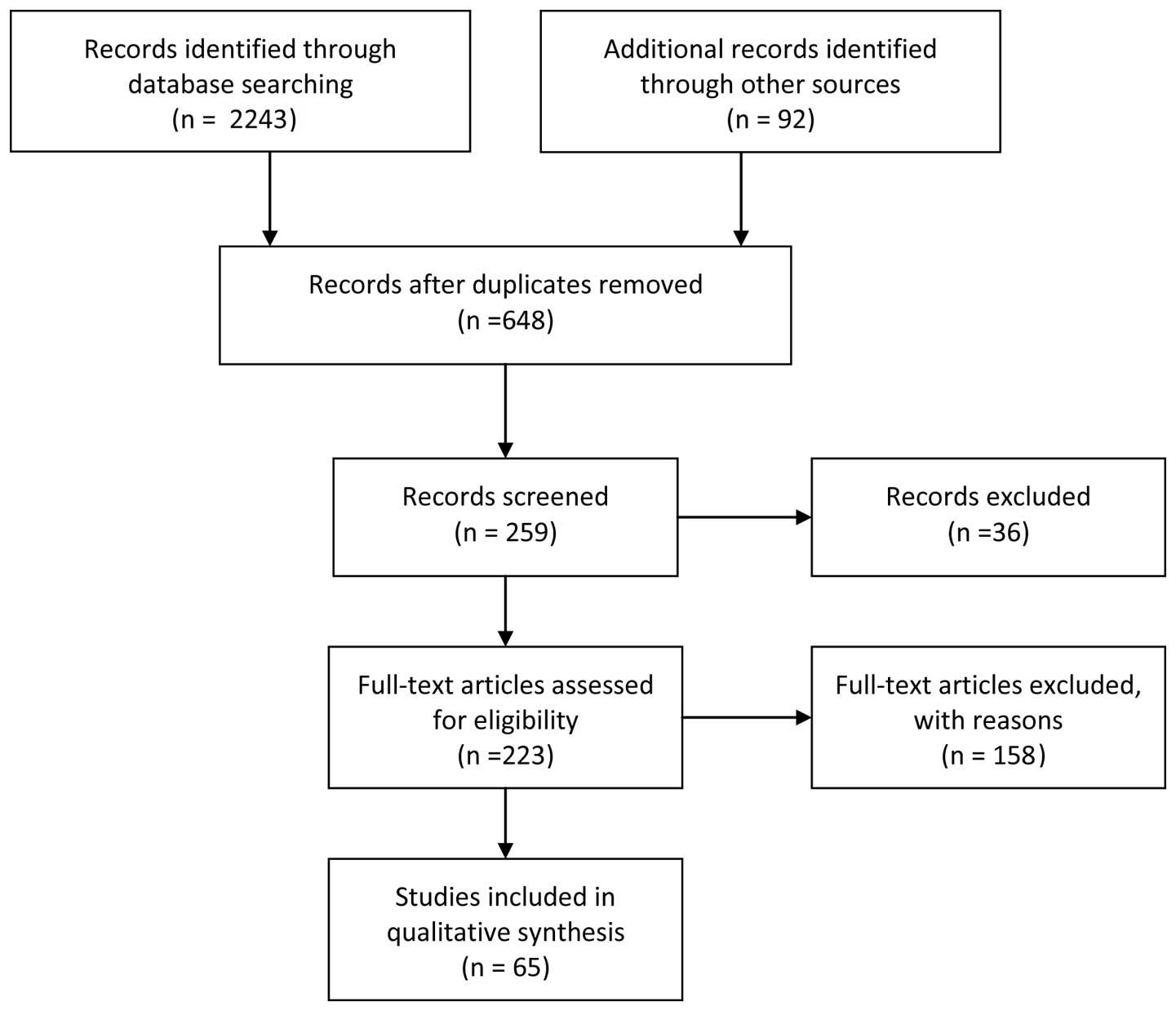
A total of 2,243 papers, and 92 additional articles
from recent reviews were found. After reviewing the abstracts, 648
papers were obtained on the basis of the aforementioned
inclusion/exclusion criteria and duplicates. After screening, 259
papers were reserved, of which 36 reviews and 158 full-text
articles were excluded after more in-depth examination, on the
basis of the same inclusion/exclusion criteria. Therefore, 65
published studies were considered eligible for the current review
(Fig. 1). Data extraction was
divided into four categories among the authors by expertise:
Potential blood-derived markers of AD and MCI, potential
CSF-derived markers of AD and MCI, potential urinary-derived
markers of AD and MCI, and cell-based techniques for analyzing tau
pathogenicity. Co-authors provided a detailed abstract of all
studies describing their strengths and weaknesses, as well as a
general evaluation of the category (9,10).
The quality of studies was assessed using the Standards for the
Reporting of Diagnostic Accuracy Studies in dementia (11).
Tau proteins in the serum are potential biomarkers
for neuronal degeneration or damage. A novel ultrasensitive digital
immunoassay technology, which is referred to as a single-molecule
ELISA, is able to detect clinically relevant proteins in the serum
at concentrations <10−15 M (19). Compared with the classic ELISA,
this ultrasensitive technique is 1,000-fold more sensitive. The
lower limit of quantification is 0.02 pg/ml, which is 100 times
higher than the plasma levels of tau proteins (~5 pg/ml). This
ultrasensitive technique has detected dynamic changes in tau
protein in the serum after hypoxic brain injury, and a mean 2-fold
increase in AD individuals, however with some overlaps with the
levels in patients with MCI and the controls (20). However, rare protein isoforms that
result due to cleavage of the tau protein and disease-specific tau
phosphorylation are not recognized by currently available assays
(21).
Aberrant lipid metabolism is associated with the
pathophysiological processes in AD. Some plasma phospholipids may
therefore be considered biomarkers for AD. Reductions in the levels
of these phospholipids may accurately predict the progression of an
individual from normal cognition to MCI or AD within 2 years
(22,23). A biomarker panel that detected
decreases in the levels of 10 phospholipids in blood plasma that
reflect cell membrane integrity may be able to predict which
cognitively normal elderly adults will develop MCI and AD with
>90% accuracy (22). Early
studies have reported that phosphatidylcholine molecules in AD
brains are decreased and that their main metabolite,
glycerophosphocholine, is increased (23,24).
However, some phosphatidylcholines produced by the sequential
methylation of another phosphatide, such as
phosphatidylethanolamine, were increased in AD brains. It has
previously been demonstrated that three phosphatidylcholine
molecules were significantly diminished in patients with AD
compared with patients with MCI or age-matched individuals
(23).
A previous study measured the plasma levels of 27
vascular-related proteins using multiplex assays or ELISA in
patients with MCI or AD, and in healthy controls. The results
indicated that N-terminal pro-brain natriuretic peptide (NT-proBNT)
was significantly increased in patients with MCI or AD, and could
be considered a potential biomarker for AD diagnosis and prognosis
(25). Multiplex assays were used
to measure 26 previously discovered AD-associated plasma biomarkers
in plasma samples from patients with AD and MCI, and elderly
non-demented individuals from three multicenter cohorts. These
assays demonstrated that 10 proteins, namely transthyretin (TTR),
clusterin, cystatin C, alpha-1-acid glycoprotein, intercellular
adhesion molecule 1, complement C4, pigment epithelium-derived
factor (PEDF), alpha-1 antitrypsin, normal T cells, and expressed
and secreted Apolipoprotein C3, were strongly associated with the
severity and progression of AD. The 10 proteins, plus the
Apolipoproteina E (ApoE) genotype, had the greatest predictive
power for identifying dementia from prodromal disease (26). In addition, butyrylcholinesterase
K-variant alleles had synergistic effects with the APOE ε4 genotype
on the conversion of MCI to AD (27). Another study measured the levels of
146 plasma proteins at baseline and after 1 year using a multiplex
immunoassay panel; the results verified that the levels of eotaxin
3, pancreatic polypeptide and NT-proBNT were increased in subjects
with AD and MCI, which was similar to changes detected in the CSF,
and also demonstrated that the Apo ε3/ε4 or ε4/ε4 genotype depended
on the biochemical profile (28).
Another study quantified 1,001 proteins by SOMAscan, and
demonstrated that protein expression levels of prostate-specific
antigen complexed to α1-antichymotrypsin, pancreatic prohormone,
clusterin and fetuin B were the most strongly associated with AD.
Pancreatic prohormone was significantly associated with left
entorhinal cortex and hippocampus atrophy, whereas fetuin B was
only related to left entorhinal atrophy. Clusterin was
significantly related to the rate of cognitive decline (29).
Other potential blood-derived markers include
mitochondrial function indicator N-acetylaspartate (NAA),
neuroinflammatory indicator chitinase-3-like 1 (YKL-40), stress
protein heme oxygenase-1 (HO-1), nutritional biomarkers,
histone-binding protein RbAp48, plasma ketone body (KB), and a
cumulative risk index based on several pathways associated with
cognitive decline for blood-derived markers. NAA levels are coupled
to neuronal mitochondrial function and are correlated with Aβ42 in
patients with AD (30). The mean
plasma and CSF levels of YKL-40 were enhanced in individuals with a
clinical dementia rating between 0.5 and 1, and YKL-40 is
considered a potential fluid biomarker for preclinical AD (31). HO-1 protein levels in plasma and
CSF, and mRNA levels of lymphocyte HO-1 in individuals with
sporadic AD are decreased compared with in normal controls, and
other subjects with chronic neurological and medical disorders
(32). A previous study suggested
that plasma levels of α-/γ-tocopherols, or plasma levels of
γ-tocotrienols in combination with structural magnetic resonance
imaging (sMRI) measures, may be used to differentiate patients with
AD or MCI from cognitively healthy individuals, and predict the
conversion of MCI to AD after 1 year of follow-up (33). High levels of homocysteine, a risk
factor for microvascular impairment, have been associated with
alterations in electroencephalographic rhythms in mild AD, but not
in MCI subjects, including unselective increases in cortical delta,
theta and alpha rhythms (34).
Compared with control individuals, plasma levels of non-enzymatic
and enzymatic antioxidants were similarly decreased in patients
with MCI and AD (35). Baseline
higher levels of free copper may be used to predict severe
cognitive decline in AD, and a faster and more obvious progression
of disability at 1 year (36).
Patients with higher levels of free copper combined with
hyperlipidemia were also prone to severe cognitive impairment.
RbAp48 modifies histone acylation and is associated with
age-related memory impairment. Post-mortem measures demonstrated
that levels of RbAp48, which are associated with
hippocampus-dependent memory deficits in elderly individuals, were
decreased in the dentate gyrus. Similar memory deficits were also
observed in RbAp48-deficient transgenic mice (37). Unlike the amyloid cascade
hypothesis, which suggests that amyloid pathways are the main
therapeutic target, the interventions based on the mitochondrial
cascade hypothesis, which suggests that mitochondrial function
decline triggers AD pathophysiological cascade, are associated with
the restoration and maintenance of mitochondrial function. The
increase in plasma KB levels induced by ketone ester in several
animal models of AD may improve mitochondrial metabolism and
postpone the appearance of AD-like pathological alterations
(38). Therefore, low plasma KB
levels may be a potential biomarker for AD pathology in individuals
with preclinical sporadic AD or reversible CF. A cummulative risk
index, including blood-derived markers ApoE ε4 and Aβ42/40,
telomere length, blood glucose, cystatin, C-reactive protein,
interleukin (IL)-6 and albumin (39), may provide valuable predictive
information regarding future cognitive trajectories independent of
age and baseline cognitive status. It is a question worthy of
further research whether this same risk index could also predict
CF. In addition, the ApoE genotype, IL-6 receptor and clusterin
plasma levels, together with Auditory-Verbal Learning Test and
Trails B have been reported to be useful for predicting brain
amyloidosis and MCI progression to AD with modest accuracy
(40). In genetic analyses of
non-familial AD, the ApoE ε4 genotype contributes to the
heterogeneity of disease processes associated with sporadic AD
(41–43). In addition, alongside the ApoE
receptor, the low density lipoprotein receptor 5 repeated allele
has been reported to be associated with the risk of dementia, and
the correlation was more evident in individuals with mixed or
vascular dementia (VaD) compared with AD (44).
The potentially associated CSF-derived biomarkers
for AD and MCI are presented in Table III. A previous study reported
that the albumin ratio between CSF and serum is normal in patients
with AD independent of age, and is increased in patients with
cerebrovascular diseases (59).
However, an elevation in the ratio was associated with AD and VaD
in an 85-year-old population, and was associated with the
conversion from non-dementia to dementia across 3 years of
follow-up (60). A previous study
indicated that age-dependent elevation in the ratio could be
observed in ApoE ε4 allele carriers without cognitive impairment
(61). An elevation in the albumin
ratio was also closely associated with severity in patients with AD
with medial temporal atrophy (62). Another study demonstrated that an
age-dependent elevation in the ratio could only be detected in the
hippocampal CA1 and dentate gyrus regions of cognitively normal
subjects (63). Compared with
cognitively normal subjects, patients with MCI exhibited an
increase in the ratio and the levels of soluble platelet-derived
growth factor receptor-β. These biomarkers of neurovascular unit
damage appeared earlier than other biomarkers, including CSF Aβ42
and tau. Increased CSF β-secretase (BACE 1) activity in individuals
with sporadic AD may be involved in the amyloidogenic process and
axonal degeneration (64).
Elevated BACE 1 activity in subjects with AD and MCI has been shown
to be associated with the ApoE ε4 genotype, and decreased levels of
Aβ42 were only observed in ApoE ε4 carriers with MCI (65). CSF levels of the soluble amyloid
precursor proteins (sAPP) α and β were similar between AD and
healthy controls; however, sAPP β levels were significantly higher
in patients with MCI compared with healthy controls (66). Significantly higher levels of sAPP
in the CSF were superior to significantly lower levels of CSF Aβ42
with regards to early prediction of the progression from MCI to AD,
and the differential diagnosis of AD from MCI and frontotemporal
dementia (67). Compared with the
stable MCI group and the control group, the levels of sAPP α and β
were significantly higher in the AD group and the MCI progression
to AD group; the ApoE ε4 allele had no effects on the levels of
sAPP α and β (68). CSF Aβ42/Aβ40
values were more sensitive than CSF levels of Aβ42 for the
identification of incipient AD in MCI individuals (69). Soluble Aβ oligomers are potential
biomarkers for AD; however, compared with the changes in CSF Aβ42
or tau, changes in the levels of soluble oligomers were not
superior for the discrimination of AD from controls (70,71).
In a comparative study of brain expression of soluble Aβ oligomers,
Aβx56, and Aβ trimers and dimers, it was demonstrated that levels
of Aβ dimers were highest in subjects with probable AD, and the
levels of Aβx56 and Aβ trimers were lowest when compared with
age-matched unimpaired and young unimpaired subjects (72). Furthermore, only Aβx56 was
correlated with pathological tau proteins and postsynaptic
proteins. These results suggested that Aβx56 may contribute to the
very early stages of AD pathogenesis. Savage et al reported
that higher Aβ oligomer levels predicted more severe dementia
(73). However, analogous to the
detection of various monomer forms, including Aβ40 and Aβ42,
developing even more specific assays to measure the precise nature
of oligomers via more sensitive amplification platforms will
improve the early diagnostic potential of these biomarkers
(74). The amide I band reflects
the structural destruction of all types of Aβ peptides. Its
downshift in CSF and blood has been detected in patients with MCI
that progressed to AD, and its downshift frequency was superior to
a single Aβ misfold or the level of specific oligomers (75).
Synaptic biomarkers in the CSF are potential early
biomarkers for AD. Neurogranin, which is mainly located in
dendritic spines, is associated with long-term potentiation and
memory consolidation. CSF neurogranin is composed of a series of
C-terminal peptides. All neurogranin peptides detected by the ELISA
method suggest that CSF neurogranin may be used to monitor synaptic
degeneration and reflect the rate of cognitive decline in
individuals with prodromal AD (76). Even if it is very rare in CSF, the
levels of CSF neurogranin peptide 48–76 exhibit the most obvious
increase in patients with AD. A progressive decline in CSF levels
of neurogranin could be observed from individuals with AD, MCI that
progressed to AD, stable MCI to controls (77). Patients with AD or MCI that
progressed to AD demonstrated significantly higher baseline CSF
levels of neurogranin compared with stable MCI or controls
(77,78). CSF levels of the cytoskeleton light
neurofilament protein were significantly higher in patients with
late-onset AD or frontotemporal dementia compared with controls
(79). In addition, alterations in
the CSF levels of axonal growth-associated protein-43 were
associated with changes in CSF tau and sAPP levels, and patients
with AD exhibited a significant increase compared with controls
(80). However, the detection of
specific peptides and other biomarkers for synaptic dysfunction
will benefit from the development of novel ultrasensitive
assays.
The onset of cognitive decline is estimated to lag
AD pathology by 10–15 years. By the time of the appearance of
clinically detectable cognitive impairment, substantial neuronal
loss has occurred. As a marker of neuronal damage, the
AD-associated neuronal thread protein AD7c-NTP is a ~41 kD
membrane-spanning phosphoprotein. The increase in immunoreactive
AD7c-NTP in the brain is associated with the increase in
p-tau-immunoreactive cytoskeletal lesions, but not the increase in
Aβ accumulation. The protein may be involved in neuronal apoptosis
and neurite sprouting, and in the pathological alterations of AD.
Dying cells in the brain are able to secrete or release the protein
into the CSF. Post-mortem CSF levels of AD7c-NTP in AD were
significantly higher compared with in age-matched controls. The CSF
levels of patients with probable AD were also significantly higher
compared with controls or other neurological disease controls, and
were associated with the severity of cognitive impairment (81). The CSF levels of visinin-like
protein-1 (VILIP-1) and the ratios of VILIP-1/Aβ42, similar to tau
and tau/Aβ, may predict future cognitive decline in cognitively
normal subjects, differentiate patients with AD from non-AD
dementia and healthy controls (82), and predict rates of global
cognitive decline in individuals with early AD (83). CSF VILIP-1 levels may also predict
rates of whole-brain and regional atrophy with a similar power to
CSF levels of tau and p-tau181 in individuals with very mild AD or
preclinical AD (84). Longitudinal
CSF biomarker patterns, including low Aβ42 in early middle age,
markedly increased t-tau, p-tau and VILIP-1 in mid- and late middle
age, and increased levels of the neuroinflammatory marker YKL-40
throughout middle age, were useful for screening middle-aged,
asymptomatic individuals with AD (85).
Systematic analysis of metabolite profiling of the
CSF by magnetic resonance spectroscopy demonstrated that increased
cortisol and cysteine levels, and decreased uridine levels, may be
involved in the progression of AD. Individuals with severe AD
exhibited increased cortisol levels, and individuals with mild AD
[Mini Mental State Examination (MMSE)>22] exhibited increased
cysteine and decreased uridine levels. Specificity and sensitivity
>75% could be obtained for the paired combination of cysteine
and uridine to identify mild AD (86). Lactate is a product of glycolytic
metabolism; CSF levels of lactate in patients with AD were
significantly higher compared with in controls and VaD controls
(87). Patients with mild AD
exhibited higher lactate levels compared with in moderate and
severe AD, and higher lactate levels corresponded with lower levels
of t-tau and p-tau. A biomarker panel that analyzed the levels of
seven proteins in the CSF by proteomic analysis and mass
spectroscopy was able to classify AD individuals from controls with
an accuracy of 84.5% (sensitivity 93.3%, specificity 75.7%)
(88). Target proteomic analysis
detected another four proteins that could reflect obvious
longitudinally dynamic alterations during AD progression (89). Other potential CSF-derived markers
include α-synuclein, heart fatty acid binding protein (HFABP),
PEDF, complexed prostaglandin-d-synthase (PDS) and TTR, isoprostane
and ferritin. CSF α-synuclein levels were not only significantly
increased in patients with MCI and AD compared with controls, the
increase in CSF α-synuclein levels was also significantly
associated with the decrease in MMSE scores (90). CSF α-synuclein levels only offered
modest sensitivity and specificity as a diagnostic marker of AD.
Significantly increased CSF levels of HFABP were detected in
patients with AD compared with controls, and in patients with MCI
that progressed to AD or VaD when compared with individuals with
stable MCI (91). However, HFABP
had a lower predictive value than Aβ42, t-tau and p-tau in
identifying the progression of MCI to AD and VaD. Cortical neurons
and astrocytes in AD brains demonstrated strong immunostaining of
PEDF, and CSF PEDF as a biomarker may improve the diagnosis of AD
(92). Complexed PDS/TTR exhibited
a significant increase in post-mortem ventricular CSF in MCI and
late-stage AD compared with diseased control subjects, and lumbar
CSF levels of the complex showed a six-fold increase in living
subjects with probable AD compared with normal control subjects
(93). CSF levels of isoprostane
were shown to possess robust longitudinal effects on the
progression of MCI to AD. The annual rate of isoprostane was
significantly different in the following order: MCI that progressed
to AD group>stable MCI group>controls (94). The elevated CSF levels of ferritin
were not only associated with cognitive performance but could also
predict AD progression (95).
Oxidative stress and oxidative DNA damage have
important roles in the process of AD. A major product of oxidative
DNA damage is 8-hydroxy-2′-deoxyguanosine (8-OHdG). The antioxidant
enzyme paraoxonase 1 (PON1) is able to prevent the oxidation of
low-density lipoproteins. Patients with AD exhibited significantly
elevated levels of 8-OHdG in urine and significantly decreased PON1
activity in serum, as compared with in healthy elderly volunteers
(100). Isoprostanes, which are
products of arachidonic acid peroxidation by free radicals, are
also biomarkers for oxidative injury. Urinary levels of
F2-isoprostanes are significantly elevated in AD subjects (101). In addition, 3-hydroxypropyl
mercapturic acid/creatinine reduction in urine is not only
associated with stroke but is also an ideal biomarker for
differentiating patients with AD from patients with MCI (102). Furthermore, high levels of
urinary polyphenols may exert protective effects of polyphenol
intake against cognitive impairment, and are associated with a
lower risk of obvious cognitive decline in elderly individuals over
a 3-year follow-up period (103).
Recently, two novel methods to detect tau
pathogenicity have been developed. One method detects tau seeding
activity in various AD brain lysates using a cell-based biosensor
assay. In vitro studies have reported that pathogenic tau
oligomers can move between cells similar to mechanisms of prion
pathogenesis, this is referred to as transcellular spread (104). Briefly, biosensor cells are
generated to express human tau proteins fused with cyan fluorescent
protein (CFP) or yellow fluorescent protein (YFP); when pathogenic
tau from AD samples is added to a culture of biosensor cells, which
contain tau proteins fused with CFP or YFP, pathogenic tau promotes
the aggregation of two fused proteins and results in a positive
fluorescence resonance energy transfer signal (105). The signal intensity reflects the
pathogenic tau seeding activity of the AD sample. Detection of
pathogenic tau seeding activity from human brain samples could
reliably differentiate AD from Huntington's disease and aged
controls (106). In addition,
P301S tau transgenic mice demonstrated that tau seeding activity is
an ideal biomarker of tauopathy. Increases in tau seeding activity
occurred 1.5 months earlier than tau deposition. Future
verification of pathogenic tau seeding activity in human CSF or
blood will improve the diagnostic accuracy of tauopathies in a
clinical setting, and provide a noninvasive biomarker to evaluate
the therapeutic efficacy of tau-modifying agents in future clinical
trials.
The second method quantitatively detects tau
pathogenicity in biological samples using monoclonal antibodies
against seeding tau. The antibodies can also be used as an
immunotherapy that traps pathogenic tau and prevents transcellular
spread. Anti-pathogenic tau antibodies that inhibit the ability for
tau pathogenicity in vitro could markedly reduce the levels
of p-tau, aggregated and insoluble tau, and inhibit microglial
activation and improve cognition in P301S tau transgenic mice
(107). If these antibodies can
be used to quantify tau pathogenicity in CSF and blood from
different individuals, they may be considered potentially
noninvasive biomarkers for detecting tau pathology.
Aging-related major neurocognitive disorders,
particularly AD-induced neurodegeneration, can progress over
decades before clinical symptoms become apparent. Biomarkers for
brain pathological processes allow for their early diagnosis in
preclinical stages and for the development of objective prognostic
assessments in clinical intervention trials. Some fluid biomarkers,
including Aβ42, t-tau and p-tau, have been widely used in clinical
practice and clinical trials. The development of novel measurement
techniques greatly promotes the production of novel biomarkers and
improves the accuracy of old biomarkers (19,20,73,74).
Several novel biomarkers associated with different aspects of AD
neuropathology are being developed, including those related to
synaptic dysfunction, neuronal damage and apoptosis, neuronal
activity alteration, neuroinflammation, oxidative stress,
metabolites, mitochondrial function and aberrant lipid metabolism.
A bioinformatics approach for identifying specific single
nucleotide polymorphisms (108–110) and epigenetic markers, including
microRNAs (111) in the CSF or
blood of patients with MCI, AD or non-AD dementia may also be
useful for AD diagnosis and differentiation.
Based on the ordering of AD biomarkers, particularly
CSF biomarkers (Aβ42, t-tau and p-tau), and AD-associated
biomarkers, such as neural injury and neuroinflammation biomarkers,
we classified which one was the earliest event resulting in the
heterogeneity of cognitive impairment. These biomarkers may be
helpful for the diagnosis of CF and the differential diagnosis of
cognitive impairment from CF, including AD or VaD. CF consists of
reversible and potentially reversible cognitive impairment subtypes
(112). The former is based on
SCD, and the latter is comparable to MCI. The most common cause of
cognitive impairment of CF is AD. The severity of SCD has been
associated with biomarkers for AD in subjects with MCI, including
low CSF Aβ42 and high CSF tau or p-tau levels (46). Longitudinal CSF biomarkers, such as
Aβ42 reductions in early middle age; markedly increased tau, p-tau
and VILIP-1 in mid- and late middle age, and increases in YKL-40
throughout middle age were associated with the severity of
cognitive impairment in prelinical AD (85). The combination of fluid biomarkers
and imaging biomarkers could further improve diagnostic accuracy of
cognitive impairment. In addition, physical frailty and AD may
share similar pathophysiological mechanisms. Certain AD-associated
fluid biomarkers, such as oxidative stress and inflammatory
markers, may also contribute to the screening of physical frailty
in CF subjects (112,113). Furthermore, the dynamic changes
of AD-specific and AD-associated fluid biomarkers may be helpful
for the screening of candidate drugs that affect cognitive
impairment and physical frailty.
The present study was supported by grants from the
Shanghai Hospital Development Center (grant no. SHDC12014221) and
the Shanghai Key Laboratory of Clinical Geriatric Medicine (grant
no. 13dz2260700).
|
1
|
Kelaiditi E, Cesari M, Canevelli M, van
Kan GA, Ousset PJ, Gillette-Guyonnet S, Ritz P, Duveau F, Soto ME,
Provencher V, et al: Cognitive frailty: Rational and definition
from an (I.A.N.A./I.A.G.G.) international consensus group. J Nutr
Health Aging. 17:726–734. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ruan Q, Yu Z, Chen M, Bao Z, Li J and He
W: Cognitive frailty, a novel target for the prevention of elderly
dependency. Ageing Res Rev. 20:1–10. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Buerger K, Frisoni G, Uspenskaya O, Ewers
M, Zetterberg H, Geroldi C, Binetti G, Johannsen P, Rossini PM,
Wahlund LO, et al: Validation of Alzheimer's disease CSF and plasma
biological markers: The multicentre reliability study of the pilot
European Alzheimer's disease neuroimaging initiative (E-ADNI). Exp
Gerontol. 44:579–585. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yang T, Hong S, O'Malley T, Sperling RA,
Walsh DM and Selkoe DJ: New ELISAs with high specificity for
soluble oligomers of amyloid β-protein detect natural Aβ oligomers
in human brain but not CSF. Alzheimers Dement. 9:99–112. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Dixon-Woods M, Agarwal S, Jones D, Young B
and Sutton A: Synthesising qualitative and quantitative evidence: A
review of possible methods. J Health Serv Res Policy. 10:45–53.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hannes K and Macaitis K: A move to more
systematic and transparent approaches in qualitative evidence
synthesis: Update on a review of published papers. Qual Res.
12:402–442. 2012. View Article : Google Scholar
|
|
7
|
McKhann GM, Knopman DS, Chertkow H, Hyman
BT, Jack CR Jr, Kawas CH, Klunk WE, Koroshetz WJ, Manly JJ, Mayeux
R, et al: The diagnosis of dementia due to Alzheimer's disease:
Recommendations from the national institute on Aging-Alzheimer's
association workgroups on diagnostic guidelines for Alzheimer's
disease. Alzheimers Dement. 7:263–269. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Albert MS, DeKosky ST, Dickson D, Dubois
B, Feldman HH, Fox NC, Gamst A, Holtzman DM, Jagust WJ, Petersen
RC, et al: The diagnosis of mild cognitive impairment due to
Alzheimer's disease: Recommendations from the national institute on
Aging-Alzheimer's association workgroups on diagnostic guidelines
for Alzheimer's disease. Alzheimers Dement. 7:270–279. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Barnett-Page E and Thomas J: Methods for
the synthesis of qualitative research: A critical review. BMC Med
Res Methodol. 9:592009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Grant MJ and Booth A: A typology of
reviews: An analysis of 14 review types and associated
methodologies. Health Info Libr J. 26:91–108. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Noel-Storr AH, McCleery JM, Richard E,
Ritchie CW, Flicker L, Cullum SJ, Davis D, Quinn TJ, Hyde C, Rutjes
AW, et al: Reporting standards for studies of diagnostic test
accuracy in dementia: The STARDdem Initiative. Neurology.
83:364–373. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Padovani A, Borroni B, Colciaghi F,
Pettenati C, Cottini E, Agosti C, Lenzi GL, Caltagirone C,
Trabucchi M, Cattabeni F and Di Luca M: Abnormalities in the
pattern of platelet amyloid precursor protein forms in patients
with mild cognitive impairment and Alzheimer disease. Arch Neurol.
59:71–75. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Borroni B, Colciaghi F, Caltagirone C,
Rozzini L, Broglio L, Cattabeni F, Di Luca M and Padovani A:
Platelet amyloid precursor protein abnormalities in mild cognitive
impairment predict conversion to dementia of Alzheimer type: A
2-year follow-up study. Arch Neurol. 60:1740–1744. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Baskin F, Rosenberg RN, Iyer L, Hynan L
and Cullum CM: Platelet APP isoform ratios correlate with declining
cognition in AD. Neurology. 54:1907–1909. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Prodan CI, Ross ED, Stoner JA, Cowan LD,
Vincent AS and Dale GL: Coated-platelet levels and progression from
mild cognitive impairment to Alzheimer disease. Neurology.
76:247–252. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lewczuk P, Kornhuber J, Vanmechelen E,
Peters O, Heuser I, Maier W, Jessen F, Bürger K, Hampel H, Frölich
L, et al: Amyloid beta peptides in plasma in early diagnosis of
Alzheimer's disease: A multicenter study with multiplexing. Exp
Neurol. 223:366–370. 2010. View Article : Google Scholar
|
|
17
|
Gurol ME, Irizarry MC, Smith EE, Raju S,
Diaz-Arrastia R, Bottiglieri T, Rosand J, Growdon JH and Greenberg
SM: Plasma beta-amyloid and white matter lesions in AD, MCI, and
cerebral amyloid angiopathy. Neurology. 66:23–29. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lopez OL, Kuller LH, Mehta PD, Becker JT,
Gach HM, Sweet RA, Chang YF, Tracy R and DeKosky ST: Plasma amyloid
levels and the risk of AD in normal subjects in the cardiovascular
health study. Neurology. 70:1664–1671. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Rissin DM, Kan CW, Campbell TG, Howes SC,
Fournier DR, Song L, Piech T, Patel PP, Chang L, Rivnak AJ, et al:
Single-molecule enzyme-linked immunosorbent assay detects serum
proteins at subfemtomolar concentrations. Nat Biotechnol.
28:595–599. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zetterberg H, Wilson D, Andreasson U,
Minthon L, Blennow K, Randall J and Hansson O: Plasma tau levels in
Alzheimer's disease. Alzheimers Res Ther. 5:92013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhang Z, Song M, Liu X, Kang SS, Kwon IS,
Duong DM, Seyfried NT, Hu WT, Liu Z, Wang JZ, et al: Cleavage of
tau by asparagine endopeptidase mediates the neurofibrillary
pathology in Alzheimer's disease. Nat Med. 20:1254–1262. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mapstone M, Cheema AK, Fiandaca MS, Zhong
X, Mhyre TR, MacArthur LH, Hall WJ, Fisher SG, Peterson DR, Haley
JM, et al: Plasma phospholipids identify antecedent memory
impairment in older adults. Nat Med. 20:415–418. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Whiley L, Sen A, Heaton J, Proitsi P,
García-Gómez D, Leung R, Smith N, Thambisetty M, Kloszewska I,
Mecocci P, et al: Evidence of altered phosphatidylcholine
metabolism in Alzheimer's disease. Neurobiol Aging. 35:271–278.
2014. View Article : Google Scholar
|
|
24
|
Nitsch RM, Blusztajn JK, Pittas AG, Slack
BE, Growdon JH and Wurtman RJ: Evidence for a membrane defect in
Alzheimer disease brain. Proc Natl Acad Sci USA. 89:1671–1675.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Marksteiner J, Imarhiagbe D, Defrancesco
M, Deisenhammer EA, Kemmler G and Humpel C: Analysis of 27
vascular-related proteins reveals that NT-proBNP is a potential
biomarker for Alzheimer's disease and mild cognitive impairment: A
pilot-study. Exp Gerontol. 50:114–121. 2014. View Article : Google Scholar
|
|
26
|
Hye A, Riddoch-Contreras J, Baird AL,
Ashton NJ, Bazenet C, Leung R, Westman E, Simmons A, Dobson R,
Sattlecker M, et al: Plasma proteins predict conversion to dementia
from prodromal disease. Alzheimers Dement. 10:799–807.e2. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lane R, Feldman HH, Meyer J, He Y, Ferris
SH, Nordberg A, Darreh-Shori T, Soininen H, Pirttilä T, Farlow MR,
et al: Synergistic effect of apolipoprotein E epsilon4 and
butyrylcholinesterase K-variant on progression from mild cognitive
impairment to Alzheimer's disease. Pharmacogenet Genomics.
18:289–298. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Soares HD, Potter WZ, Pickering E, Kuhn M,
Immermann FW, Shera DM, Ferm M, Dean RA, Simon AJ, Swenson F, et
al: Plasma biomarkers associated with the apolipoprotein E genotype
and Alzheimer disease. Arch Neurol. 69:1310–1317. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sattlecker M, Kiddle SJ, Newhouse S,
Proitsi P, Nelson S, Williams S, Johnston C, Killick R, Simmons A,
Westman E, et al: Alzheimer's disease biomarker discovery using
SOMAscan multiplexed protein technology. Alzheimers Dement.
10:724–734. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Jessen F, Lewczuk P, Gür O, Block W, Ende
G, Frölich L, Hammen T, Arlt S, Kornhuber J, Kucinski T, et al:
Association of N-acetylaspartate and cerebrospinal fluid Aβ42 in
dementia. J Alzheimers Dis. 27:393–399. 2011.
|
|
31
|
Craig-Schapiro R, Perrin RJ, Roe CM, Xiong
C, Carter D, Cairns NJ, Mintun MA, Peskind ER, Li G, Galasko DR, et
al: YKL-40: A novel prognostic fluid biomarker for preclinical
Alzheimer's disease. Biol Psychiatry. 68:903–912. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Schipper HM, Chertkow H, Mehindate K,
Frankel D, Melmed C and Bergman H: Evaluation of heme oxygenase-1
as a systemic biological marker of sporadic AD. Neurology.
54:1297–1304. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Mangialasche F, Westman E, Kivipelto M,
Muehlboeck JS, Cecchetti R, Baglioni M, Tarducci R, Gobbi G,
Floridi P, Soininen H, et al: Classification and prediction of
clinical diagnosis of Alzheimer's disease based on MRI and plasma
measures of α-/γ-tocotrienols and γ-tocopherol. J Intern Med.
273:602–621. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Babiloni C, Bosco P, Ghidoni R, Del Percio
C, Squitti R, Binetti G, Benussi L, Ferri R, Frisoni G, Lanuzza B,
et al: Homocysteine and electroencephalographic rhythms in
Alzheimer disease: A multicentric study. Neuroscience. 145:942–954.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Rinaldi P, Polidori MC, Metastasio A,
Mariani E, Mattioli P, Cherubini A, Catani M, Cecchetti R, Senin U
and Mecocci P: Plasma antioxidants are similarly depleted in mild
cognitive impairment and in Alzheimer's disease. Neurobiol Aging.
24:915–919. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Squitti R, Bressi F, Pasqualetti P,
Bonomini C, Ghidoni R, Binetti G, Cassetta E, Moffa F, Ventriglia
M, Vernieri F and Rossini PM: Longitudinal prognostic value of
serum 'free' copper in patients with Alzheimer disease. Neurology.
72:50–55. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Pavlopoulos E, Jones S, Kosmidis S, Close
M, Kim C, Kovalerchik O, Small SA and Kandel ER: Molecular
mechanism for age-related memory loss: The histone-binding protein
RbAp48. Sci Transl Med. 5:200ra1152013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Hertz L, Chen Y and Waagepetersen HS:
Effects of ketone bodies in Alzheimer's disease in relation to
neural hypometabolism, β-amyloid toxicity, and astrocyte function.
J Neurochem. 134:7–20. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Nettiksimmons J, Ayonayon H, Harris T,
Phillips C, Rosano C, Satterfield S and Yaffe K; Health ABC Study:
Development and validation of risk index for cognitive decline
using blood-derived markers. Neurology. 84:696–702. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Apostolova LG, Hwang KS, Avila D, Elashoff
D, Kohannim O, Teng E, Sokolow S, Jack CR, Jagust WJ, Shaw L, et
al: Brain amyloidosis ascertainment from cognitive, imaging, and
peripheral blood protein measures. Neurology. 84:729–737. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Smits LL, Pijnenburg YA, van der Vlies AE,
Koedam EL, Bouwman FH, Reuling IE, Scheltens P and van der Flier
WM: Early onset APOE E4-negative Alzheimer's disease patients show
faster cognitive decline on non-memory domains. Eur
Neuropsychopharmacol. 25:1010–1017. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Michaelson DM: APOE ε4: The most prevalent
yet understudied risk factor for Alzheimer's disease. Alzheimers
Dement. 10:861–868. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Lautner R, Palmqvist S, Mattsson N,
Andreasson U, Wallin A, Pålsson E, Jakobsson J, Herukka SK, Owenius
R, Olsson B, et al: Apolipoprotein E genotype and the diagnostic
accuracy of cerebrospinal fluid biomarkers for Alzheimer disease.
JAMA Psychiatry. 71:1183–1191. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Helbecque N, Berr C, Cottel D,
Fromentin-David I, Sazdovitch V, Ricolfi F, Ducimetière P, Di Menza
C and Amouyel P: VLDL receptor polymorphism, cognitive impairment,
and dementia. Neurology. 56:1183–1188. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Riemenschneider M, Lautenschlager N,
Wagenpfeil S, Diehl J, Drzezga A and Kurz A: Cerebrospinal fluid
tau and beta-amyloid 42 proteins identify Alzheimer disease in
subjects with mild cognitive impairment. Arch Neurol. 59:1729–1734.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Wolfsgruber S, Jessen F, Koppara A,
Kleineidam L, Schmidtke K, Frölich L, Kurz A, Schulz S, Hampel H,
Heuser I, et al: Subjective cognitive decline is related to CSF
biomarkers of AD in patients with MCI. Neurology. 84:1261–1268.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Ewers M, Mattsson N, Minthon L, Molinuevo
JL, Antonell A, Popp J, Jessen F, Herukka SK, Soininen H, Maetzler
W, et al: CSF biomarkers for the differential diagnosis of
Alzheimer's disease: A large-scale international multicenter study.
Alzheimers Dement. 11:1306–1315. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Landau SM, Lu M, Joshi AD, Pontecorvo M,
Mintun MA, Trojanowski JQ, Shaw LM and Jagust WJ; Alzheimer's
Disease Neuroimaging Initiative: Comparing positron emission
tomography imaging and cerebrospinal fluid measurements of
β-amyloid. Ann Neurol. 74:826–836. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Nettiksimmons J, Harvey D, Brewer J,
Carmichael O, DeCarli C, Jack CR Jr, Petersen R, Shaw LM,
Trojanowski JQ, Weiner MW, et al: Subtypes based on cerebrospinal
fluid and magnetic resonance imaging markers in normal elderly
predict cognitive decline. Neurobiol Aging. 31:1419–1428. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Okonkwo OC, Alosco ML, Griffith HR, Mielke
MM, Shaw LM, Trojanowski JQ and Tremont G; Alzheimer's Disease
Neuroimaging Initiative: Cerebrospinal fluid abnormalities and rate
of decline in everyday function across the dementia spectrum:
Normal aging, mild cognitive impairment and Alzheimer disease. Arch
Neurol. 67:688–696. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Mattsson N, Zetterberg H, Hansson O,
Andreasen N, Parnetti L, Jonsson M, Herukka SK, van der Flier WM,
Blankenstein MA, Ewers M, et al: CSF biomarkers and incipient
Alzheimer disease in patients with mild cognitive impairment. JAMA.
302:385–393. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Landau SM, Harvey D, Madison CM, Reiman
EM, Foster NL, Aisen PS, Petersen RC, Shaw LM, Trojanowski JQ, Jack
CR Jr, et al: Comparing predictors of conversion and decline in
mild cognitive impairment. Neurology. 75:230–238. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Van Rossum IA, Vos SJ, Burns L, Knol DL,
Scheltens P, Soininen H, Wahlund LO, Hampel H, Tsolaki M, Minthon
L, et al: Injury markers predict time to dementia in subjects with
MCI and amyloid pathology. Neurology. 79:1809–1816. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Vemuri P, Wiste HJ, Weigand SD, Shaw LM,
Trojanowski JQ, Weiner MW, Knopman DS, Petersen RC and Jack CR Jr;
Alzheimer's Disease Neuroimaging Initiative: MRI and CSF biomarkers
in normal, MCI, and AD subjects: Predicting future clinical change.
Neurology. 73:294–301. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Eckerström C, Olsson E, Bjerke M, Malmgren
H, Edman A, Wallin A and Nordlund A: A combination of
neuropsychological, neuroimaging, and cerebrospinal fluid markers
predicts conversion from mild cognitive impairment to dementia. J
Alzheimers Dis. 36:421–431. 2013.PubMed/NCBI
|
|
56
|
Shaffer JL, Petrella JR, Sheldon FC,
Choudhury KR, Calhoun VD, Coleman RE and Doraiswamy PM; Alzheimer's
Disease Neuroimaging Initiative: Predicting cognitive decline in
subjects at risk for Alzheimer disease by using combined
cerebrospinalfluid, MR imaging, and PET biomarkers. Radiology.
266:583–591. 2013. View Article : Google Scholar :
|
|
57
|
Ewers M, Walsh C, Trojanowski JQ, Shaw LM,
Petersen RC, Jack CR Jr, Feldman HH, Bokde AL, Alexander GE,
Scheltens P, et al: Prediction of conversion from mild cognitive
impairment to Alzheimer's disese dementia based upon biomarkers and
neuropsychological test performance. Neurobiol Aging. 33:1203–1214.
2012. View Article : Google Scholar
|
|
58
|
Vemuri P, Wiste HJ, Weigand SD, Knopman
DS, Trojanowski JQ, Shaw LM, Bernstein MA, Aisen PS, Weiner M,
Petersen RC, et al: Serial MRI and CSF biomarkers in normal aging,
MCI, and AD. Neurology. 75:143–151. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Blennow K, Wallin A, Fredman P, Karlsson
I, Gottfries CG and Svennerholm L: Blood-brain barrier disturbance
in patients with Alzheimer's disease is related to vascular
factors. Acta Neurol Scand. 81:323–326. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Skoog I, Wallin A, Fredman P, Hesse C,
Aevarsson O, Karlsson I, Gottfries CG and Blennow K: A population
study on blood-brain barrier function in 85-year-olds: Relation to
Alzheimer's disease and vascular dementia. Neurology. 50:966–971.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Halliday MR, Pomara N, Sagare AP, Mack WJ,
Frangione B and Zlokovic BV: Relationship between cyclophilin a
levels and matrix metalloproteinase 9 activity in cerebrospinal
fluid of cognitively normal apolipoprotein e4 carriers and
blood-brain barrier breakdown. JAMA Neurol. 70:1198–1200. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Matsumoto Y, Yanase D, Noguchi-Shinohara
M, Ono K, Yoshita M and Yamada M: Blood-brain barrier permeability
correlates with medial temporal lobe atrophy but not with
amyloid-beta protein transport across the blood-brain barrier in
Alzheimer's disease. Dement Geriatr Cogn Disord. 23:241–245. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Montagne A, Barnes SR, Sweeney MD,
Halliday MR, Sagare AP, Zhao Z, Toga AW, Jacobs RE, Liu CY, Amezcua
L, et al: Blood-brain barrier breakdown in the aging human
hippo-campus. Neuron. 85:296–302. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Zetterberg H, Andreasson U, Hansson O, Wu
G, Sankaranarayanan S, Andersson ME, Buchhave P, Londos E, Umek RM,
Minthon L, et al: Elevated cerebrospinal fluid BACE1 activity in
incipient Alzheimer disease. Arch Neurol. 65:1102–1107. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Ewers M, Zhong Z, Bürger K, Wallin A,
Blennow K, Teipel SJ, Shen Y and Hampel H: Increased CSF-BACE 1
activity is associated with ApoE-epsilon 4 genotype in subjects
with mild cognitive impairment and Alzheimer's disease. Brain.
131:1252–1258. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Olsson A, Höglund K, Sjögren M, Andreasen
N, Minthon L, Lannfelt L, Buerger K, Möller HJ, Hampel H, Davidsson
P and Blennow K: Measurement of alpha- and beta-secretase cleaved
amyloid precursor protein in cerebrospinal fluid from Alzheimer
patients. Exp Neurol. 183:74–80. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Perneczky R, Tsolakidou A, Arnold A,
Diehl-Schmid J, Grimmer T, Förstl H, Kurz A and Alexopoulos P: CSF
soluble amyloid precursor proteins in the diagnosis of incipient
Alzheimer disease. Neurology. 77:35–38. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Lewczuk P, Popp J, Lelental N, Kölsch H,
Maier W, Kornhuber J and Jessen F: Cerebrospinal fluid soluble
amyloid-β protein precursor as a potential novel biomarkers of
Alzheimer's disease. J Alzheimers Dis. 28:119–125. 2012.
|
|
69
|
Hansson O, Zetterberg H, Buchhave P,
Andreasson U, Londos E, Minthon L and Blennow K: Prediction of
Alzheimer's disease using the CSF Abeta42/Abeta40 ratio in patients
with mild cognitive impairment. Dement Geriatr Cogn Disord.
23:316–320. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Hölttä M, Hansson O, Andreasson U, Hertze
J, Minthon L, Nägga K, Andreasen N, Zetterberg H and Blennow K:
Evaluating amyloid-β oligomers in cerebrospinal fluid as a
biomarker for Alzheimer's disease. PLoS One. 8:e663812013.
View Article : Google Scholar
|
|
71
|
Herskovits AZ, Locascio JJ, Peskind ER, Li
G and Hyman BT: A Luminex assay detects amyloid β oligomers in
Alzheimer's disease cerebrospinal fluid. PLoS One. 8:e678982013.
View Article : Google Scholar
|
|
72
|
Lesne SE, Sherman MA, Grant M, Kuskowski
M, Schneider JA, Bennett DA and Ashe KH: Brain amyloid-β oligomers
in ageing and Alzheimer's disease. Brain. 136:1383–1398. 2013.
View Article : Google Scholar
|
|
73
|
Savage MJ, Kalinina J, Wolfe A, Tugusheva
K, Korn R, Cash-Mason T, Maxwell JW, Hatcher NG, Haugabook SJ, Wu
G, et al: A sensitive aβ oligomer assay discriminates Alzheimer's
and aged control cerebrospinal fluid. J Neurosci. 34:2884–2897.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Yang T, O'Malley TT, Kanmert D, Jerecic J,
Zieske LR, Zetterberg H, Hyman BT, Walsh DM and Selkoe DJ: A highly
sensitive novel immunoassay specifically detects low levels of
soluble Aβ oligomers in human cerebrospinal fluid. Alzheimers Res
Ther. 7:142015. View Article : Google Scholar
|
|
75
|
Nabers A, Ollesch J, Schartner J, Kötting
C, Genius J, Hafermann H, Klafki H, Gerwert K and Wiltfang J:
Amyloid-β-secondary structure distribution in cerebrospinal fluid
and blood measured by an immune-infrared-sensor: A biomarker
candidate for Alzheimer's disease. Anal Chem. 88:2755–2762. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Kvartsberg H, Duits FH, Ingelsson M,
Andreasen N, Öhrfelt A, Andersson K, Brinkmalm G, Lannfelt L,
Minthon L, Hansson O, et al: Cerebrospinal fluid levels of the
synaptic protein neurogranin correlates with cognitive decline in
prodromal Alzheimer's disease. Alzheimers Dement. 11:1180–1190.
2015. View Article : Google Scholar
|
|
77
|
Portelius E, Zetterberg H, Skillbäck T,
Törnqvist U, Andreasson U, Trojanowski JQ, Weiner MW, Shaw LM,
Mattsson N and Blennow K; Alzheimer's Disease Neuroimaging
Initiative: Cerebrospinal fluid neurogranin: Relation to cognition
and neurodegeneration in Alzheimer's disease. Brain. 138:3373–3385.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Kester MI, Teunissen CE, Crimmins DL,
Herries EM, Ladenson JH, Scheltens P, van der Flier WM, Morris JC,
Holtzman DM and Fagan AM: Neurogranin as a cerebrospinal fluid
biomarker for synaptic loss in symptomatic Alzheimer disease. JAMA
Neurol. 72:1275–1280. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Sjögren M, Rosengren L, Minthon L,
Davidsson P, Blennow K and Wallin A: Cytoskeleton proteins in CSF
distinguish frontotemporal dementia from AD. Neurology.
54:1960–1964. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Sjögren M, Davidsson P, Gottfries J,
Vanderstichele H, Edman A, Vanmechelen E, Wallin A and Blennow K:
The cerebrospinal fluid levels of tau, growth-associated protein-43
and soluble amyloid precursor proteincorrelate in Alzheimer's
disease, reflecting a common pathophysiological process. Dement
Geriatr Cogn Disord. 12:257–264. 2001. View Article : Google Scholar
|
|
81
|
de la Monte SM, Ghanbari K, Frey WH,
Beheshti I, Averback P, Hauser SL, Ghanbari HA and Wands JR:
Characterization of the AD7C-NTP cDNA expression in Alzheimer's
disease and measurement of a 41-kDprotein in cerebrospinal fluid. J
Clin Invest. 100:3093–3104. 1997. View Article : Google Scholar
|
|
82
|
Tarawneh R, D'Angelo G, Macy E, Xiong C,
Carter D, Cairns NJ, Fagan AM, Head D, Mintun MA, Ladenson JH, et
al: Visinin-like protein-1: Diagnostic and prognostic biomarker in
Alzheimer disease. Ann Neurol. 70:274–285. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Tarawneh R, Lee JM, Ladenson JH, Morris JC
and Holtzman DM: CSF VILIP-1 predicts rates of cognitive decline in
early Alzheimer disease. Neurology. 78:709–719. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Tarawneh R, Head D, Allison S, Buckles V,
Fagan AM, Ladenson JH, Morris JC and Holtzman DM: Cerebrospinal
fluid markers of neurodegeneration and rates of brain atrophy in
early Alzheimer disease. JAMA Neurol. 72:656–665. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Sutphen CL, Jasielec MS, Shah AR, Macy EM,
Xiong C, Vlassenko AG, Benzinger TL, Stoops EE, Vanderstichele HM,
Brix B, et al: Longitudinal cerebrospinal fluid biomarker changes
in preclinical Alzheimer disease during middle age. JAMA Neurol.
72:1029–1042. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Czech C, Berndt P, Busch K, Schmitz O,
Wiemer J, Most V, Hampel H, Kastler J and Senn H: Metabolite
profiling of Alzheimer's disease cerebrospinal fluid. PLoS One.
7:e315012012. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Liguori C, Stefani A, Sancesario G,
Sancesario GM, Marciani MG and Pierantozzi M: CSF lactate levels, τ
proteins, cognitive decline: A dynamic relationship in Alzheimer's
disease. J Neurol Neurosurg Psychiatry. 86:655–659. 2015.
View Article : Google Scholar
|
|
88
|
Vafadar-Isfahani B, Ball G, Coveney C,
Lemetre C, Boocock D, Minthon L, Hansson O, Miles AK, Janciauskiene
SM, Warden D, et al: Identification of SPARC-like 1 protein as part
of a biomarker panel for Alzheimer's disease in cerebrospinal
fluid. J Alzheimers Dis. 28:625–636. 2012.
|
|
89
|
Wildsmith KR, Schauer SP, Smith AM, Arnott
D, Zhu Y, Haznedar J, Kaur S, Mathews WR and Honigberg LA:
Identification of longitudinally dynamic biomarkers in Alzheimer's
disease cerebrospinal fluid by targeted proteomics. Mol
Neurodegener. 9:222014. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Korff A, Liu C, Ginghina C, Shi M and
Zhang J; Alzheimer's Disease Neuroimaging Initiative: α-Synuclein
in cerebrospinal fluid of Alzheimer's disease and mild cognitive
impairment. J Alzheimers Dis. 36:679–688. 2013.
|
|
91
|
Olsson B, Hertze J, Ohlsson M, Nägga K,
Höglund K, Basun H, Annas P, Lannfelt L, Andreasen N, Minthon L, et
al: Cerebrospinal fluid levels of heart fatty acid binding protein
are elevated prodromally in Alzheimer's disease and vascular
dementia. J Alzheimers Dis. 34:673–679. 2013.
|
|
92
|
Yamagishi S, Inagaki Y, Takeuchi M and
Sasaki N: Is pigment epithelium-derived factor level in
cerebrospinal fluid a promising biomarker for early diagnosis of
Alzheimer's disease? Med Hypotheses. 63:115–117. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Lovell MA, Lynn BC, Xiong S, Quinn JF,
Kaye J and Markesbery WR: An aberrant protein complex in CSF as a
biomarker of Alzheimer disease. Neurology. 70:2212–2218. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Brys M, Pirraglia E, Rich K, Rolstad S,
Mosconi L, Switalski R, Glodzik-Sobanska L, De Santi S, Zinkowski
R, Mehta P, et al: Prediction and longitudinal study of CSF
biomarkers in mild cognitive impairment. Neurobiol Aging.
30:682–690. 2009. View Article : Google Scholar :
|
|
95
|
Ayton S, Faux NG and Bush AI; Alzheimer's
Disease Neuroimaging Initiative: Ferritin levels in the
cerebrospinal fluid predict Alzheimer's disease outcomes and are
regulated by APOE. Nat Commun. 6:67602015. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Ghanbari H, Ghanbari K, Beheshti I, Munzar
M, Vasauskas A and Averback P: Biochemical assay for AD7C-NTP in
urine as an Alzheimer's disease marker. J Clin Lab Anal.
12:285–288. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Goodman I, Golden G, Flitman S, Xie K,
McConville M, Levy S, Zimmerman E, Lebedeva Z, Richter R, Minagar A
and Averback P: A multi-center blinded prospective study of urine
neural thread protein measurements in patients with suspected
Alzheimer's disease. J Am Med Dir Assoc. 8:21–30. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
de la Monte SM and Wands JR: The AD7c-ntp
neuronal thread protein biomarker for detecting Alzheimer's
disease. Front Biosci. 7:d989–d996. 2002.PubMed/NCBI
|
|
99
|
Ma L, Chen J, Wang R, Han Y, Zhang J, Dong
W, Zhang X, Wu Y and Zhao Z: The level of Alzheimer-associated
neuronal thread protein in urine may be an important biomarker of
mild cognitive impairment. J Clin Neurosci. 22:649–652. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Zengi O, Karakas A, Ergun U, Senes M, Inan
L and Yucel D: Urinary 8-hydroxy-2′-deoxyguanosine level and plasma
paraoxonase 1 activity withAlzheimer's disease. Clin Chem Lab Med.
50:529–534. 2011.PubMed/NCBI
|
|
101
|
Kim KM, Jung BH, Paeng KJ, Kim I and Chung
BC: Increased urinary F(2) isoprostanes levels in the patients with
Alzheimer's disease. Brain Res Bull. 64:47–51. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Yoshida M, Higashi K, Kuni K, Mizoi M,
Saiki R, Nakamura M, Waragai M, Uemura K, Toida T, Kashiwagi K and
Igarashi K: Distinguishing mild cognitive impairment from
Alzheimer's disease with acrolein metabolites and creatinine in
urine. Clin Chim Acta. 441:115–121. 2015. View Article : Google Scholar
|
|
103
|
Rabassa M, Cherubini A, Zamora-Ros R,
Urpi-Sarda M, Bandinelli S, Ferrucci L and Andres-Lacueva C: Low
levels of a urinary biomarker of dietary polyphenol are associated
with substantial cognitive decline over a 3-year period in older
adults: The invecchiare in chianti study. J Am Geriatr Soc.
63:938–946. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Cook CN, Murray ME and Petrucelli L:
Understanding biomarkers of neurodegeneration: Novel approaches to
detecting tau pathology. Nat Med. 21:219–220. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Kfoury N, Holmes BB, Jiang H, Holtzman DM
and Diamond MI: Trans-cellular propagation of Tau aggregation by
fibrillar species. J Biol Chem. 287:19440–19451. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Holmes BB, Furman JL, Mahan TE, Yamasaki
TR, Mirbaha H, Eades WC, Belaygorod L, Cairns NJ, Holtzman DM and
Diamond MI: Proteopathic tau seeding predicts tauopathy in vivo.
Proc Natl Acad Sci USA. 111:E4376–E4385. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Yanamandra K, Kfoury N, Jiang H, Mahan TE,
Ma S, Maloney SE, Wozniak DF, Diamond MI and Holtzman DM: Anti-tau
antibodies that block tau aggregate seeding in vitro markedly
decrease pathology and improve cognition in vivo. Neuron.
80:402–414. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Kong D, Giovanello KS, Wang Y, Lin W, Lee
E, Fan Y, Murali Doraiswamy P and Zhu H: Predicting Alzheimer's
disease using combined imaging-whole genome SNP data. J Alzheimers
Dis. 46:695–702. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Sun Y, Bresell A, Rantalainen M, Höglund
K, Lebouvier T and Salter H; Alzheimer Disease Neuroimaging
Initiative: An integrated bioinformatics approach for identifying
genetic markers that predict cerebrospinal fluid biomarker
p-tau181/Aβ1-42 ratio in ApoE4-negative mild cognitive impairment
patients. J Alzheimers Dis. 45:1061–1076. 2015.
|
|
110
|
Castro-Chavira SA, Fernandez T, Nicolini
H, Diaz-Cintra S and Prado-Alcala RA: Genetic markers in biological
fluids for aging-related major neurocognitive disorder. Curr
Alzheimer Res. 12:200–209. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Femminella GD, Ferrara N and Rengo G: The
emerging role of microRNAs in Alzheimer's disease. Front Physiol.
6:402015. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Namioka N, Hanyu H, Hirose D, Hatanaka H,
Sato T and Shimizu S: Oxidative stress and inflammation are
associated with physical frailty in patients with Alzheimer's
disease. Geriatr Gerontol Int. Jun 14–2016.Epub ahead of print.
View Article : Google Scholar
|
|
113
|
Panza F, Solfrizzi V, Barulli MR,
Santamato A, Seripa D, Pilotto A and Logroscino G: Cognitive
Frailty: A systematic review of epidemiological and neurobiological
evidence of an age-related clinical condition. Rejuvenation Res.
18:389–412. 2015. View Article : Google Scholar : PubMed/NCBI
|