Introduction
Recently, the synchronous occurrence of primary
neoplasms has been studied with increasing frequency, which may be
due to the improved preoperative imaging capabilities. The
coexistence of gastrointestinal stromal tumors (GISTs) with other
gastrointestinal or non-gastrointestinal malignancies has also been
studied with increasing frequency, although the occurrence remains
rare (1). It has been identified
that the overall frequency of second tumors in different sites
among patients with GISTs ranges between 4.5 and 18.6%, with a mean
of 13% (2).
GISTs are the most common type of mesenchymal tumor
of the gastrointestinal tract, which most likely arise from
precursor interstitial cells of Cajal. The majority of GISTs occur
as a single lesion. They are common in the stomach (60–70% of all
cases) and small intestine (30%), while they rarely occur in the
rectum (5%), esophagus, colon, pancreas, appendix, omentum,
mesentery and retroperitoneum (3).
The best survival predictors are the size, location and mitotic
rate of the tumor.
Pancreatic cancer is a common gastrointestinal
malignancy. Ductal adenocarcinoma accounts for 80–85% of pancreatic
tumors, while adenosquamous carcinoma (ASC) of the pancreas is a
rare, aggressive variant of pancreatic carcinoma with a worse
prognosis. Its exact incidence is not known; however, autopsy and
surgical specimen findings suggest that this lesion accounts for
1–4% of all exocrine malignancies of the pancreas (4).
The uncinate process is a hook-like extension of the
lower part of the pancreatic head that projects medially and wraps
around the superior mesenteric vessels. Carcinoma in the uncinate
process of the pancreas (CUPP) appears to be less common than that
in other parts of the pancreas. Previous studies identify an
incidence rate of 2.5% (3/119) (5),
7.7% (39/506) (6) and 10.7% (6/56)
(7) of pancreatic malignancies.
To the best of our knowledge, only one case in the
literature demonstrated coexistence of ASC of the head of the
pancreas with GIST (8), and the
small GIST in this patient was only incidentally identified
following surgery. With approved patient consent, we report a case
of ASC of the uncinate process of the pancreas with the synchronous
occurrence of large symptomatic GIST. 1. The study was approved by
the Ethics Committee of The Second Affiliated Hospital, Zhejiang
University School of Medicine, Hangzhou, China.
Case report
A 62-year-old female presented with a chief
complaint of recurrent epigastric discomfort and progressively
worsening vomiting for two weeks. The patient had experienced
anorexia and weight loss for several months, but had no significant
past medical history. The patient’s family history was significant
for pancreatic cancer from her mother, but no other malignancies
were present in her other immediate family members. On admission,
the patient’s vital signs were stable and a mass of approximately
10 cm was palpated in the upper quadrant area of the abdomen. The
remainder of the examination was unremarkable.
The complete blood count identified a white cell
count of 6,900 cells/mm3 (73.4% neutrophils), hemoglobin
count of 135 g/dl and a platelet count of 181,000
platelets/mm3. The blood chemistry examination revealed
23.0 μmol/l total bilirubin, 9.6 μmol/l direct
bilirubin, 74 U/l aspartate transaminase (AST) and 102 U/l alanine
aminotransferase (ALT). The carbohydrate antigen 19-9 (CA19-9) was
slightly elevated to 78.4 U/l (normal range, 0–37 U/l), while
carcinoembryonic antigen (CEA), α-fetoprotein (AFP), carbohydrate
antigen 24-2 (CA24-2), blood glucose, calcium and amylase levels
were within normal ranges.
Computed tomography (CT) revealed a discrete mass
measuring 8×7 cm with notable enhancement in the body of stomach
(Fig. 1). It also revealed a 4×3-cm
lesion with an unclear boundary and mild enhancement in the
uncinate process of pancreas and close to the horizontal part of
the duodenum (Fig. 2).
Ultrasonography of the liver, pancreas, spleen and gallbladder
revealed no abnormality.
The initial impression from the CT scan was
emphasized on the gastric mass as the lesion in the uncinate
process of the pancreas was not well-defined. The gastric mass was
suspected to be a GIST (Fig. 1),
and the symptoms of bowel obstruction were suggested to be caused
by the presumed GIST in the patient’s stomach. However, an upper
gastrointestinal series with meglumine diatrizoate was consistent
with a partial bowel obstruction at the level of the third portion
of duodenum. Therefore, the case was discussed at the
multi-disciplinary team (MDT) conference, and it was recommended to
intraoperatively explore the pancreas in addition to the resection
of the gastric mass.
Intraoperatively, no liver metastasis or peritoneal
dissemination was identified. A solid, partially capsulated mass,
measuring approximately 8×7×7 cm, was identified in the body of the
stomach near the lesser curvature. Another solid mass was also
revealed in the uncinate process of the pancreas, which had
horizontally infiltrated part of duodenum and closely adhered to
the inferior vena cava for ∼4 cm (Fig.
2). A fine needle aspiration biopsy was conducted in the
uncinate process of the pancreas and revealed the adenocarcinoma.
Therefore, a pancreaticoduodenectomy (PD) was conducted, which
included resection of the gastric mass and partial resection of the
inferior vena cava.
The pathological specimen was composed of the head
of the pancreas, distal portion of the stomach, common bile duct,
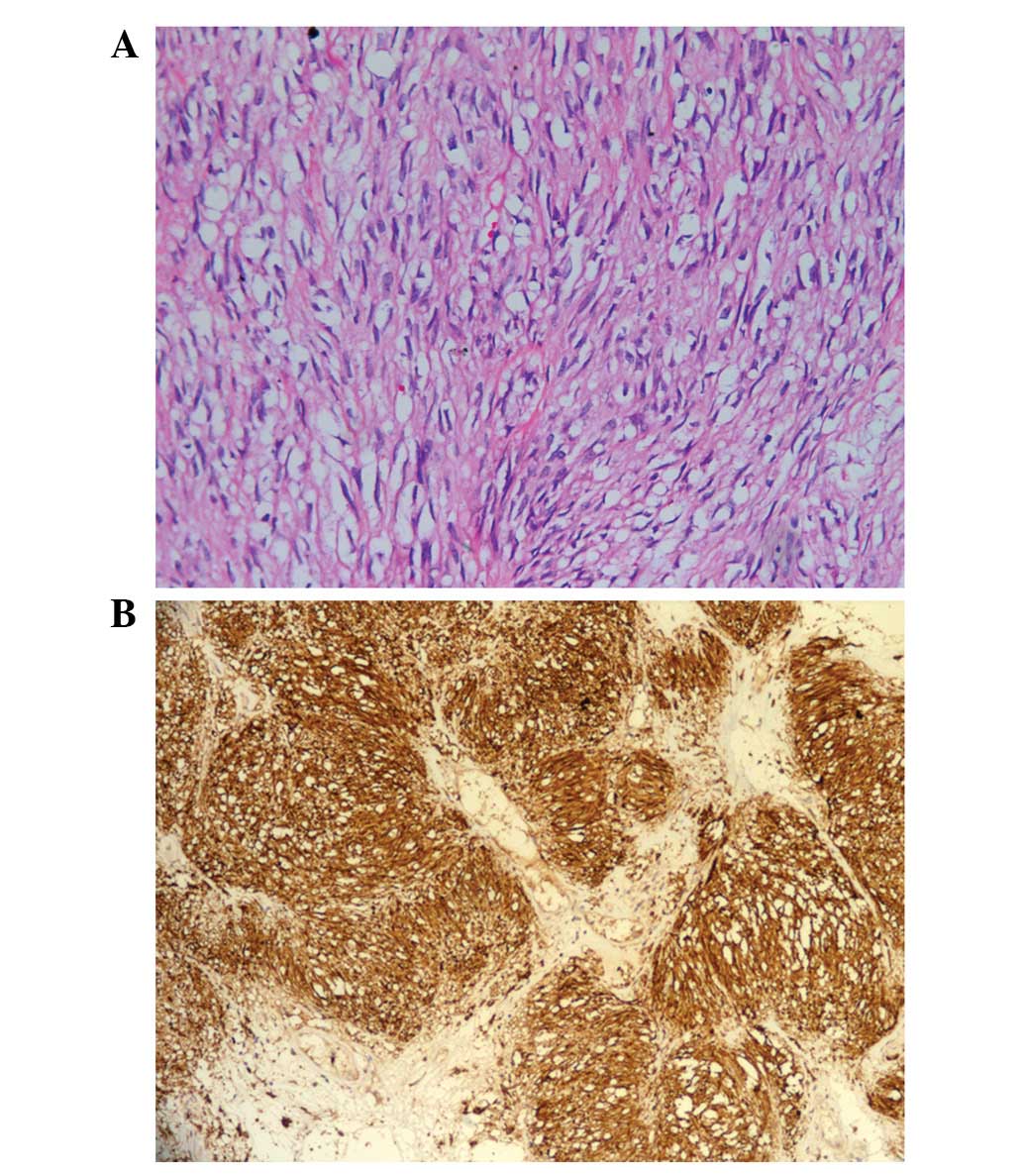
duodenum and gallbladder. Microscopically, the gastric tumor tissue
was comprised of spindle cells with coagulative necrosis and a
mitotic rate of ≤5/50 within a high power field (HPF; Fig. 3A). The tumor cells were
immunoreactive for CD117 (Fig. 3B),
supporting the diagnosis of GIST. The Union for International
Cancer Control tumor-node-metastasis (UICC TNM) pathological
staging of this GIST was pT3 (stage IB), and its National Institute
of Health (NIH) risk stratification was intermediate. The
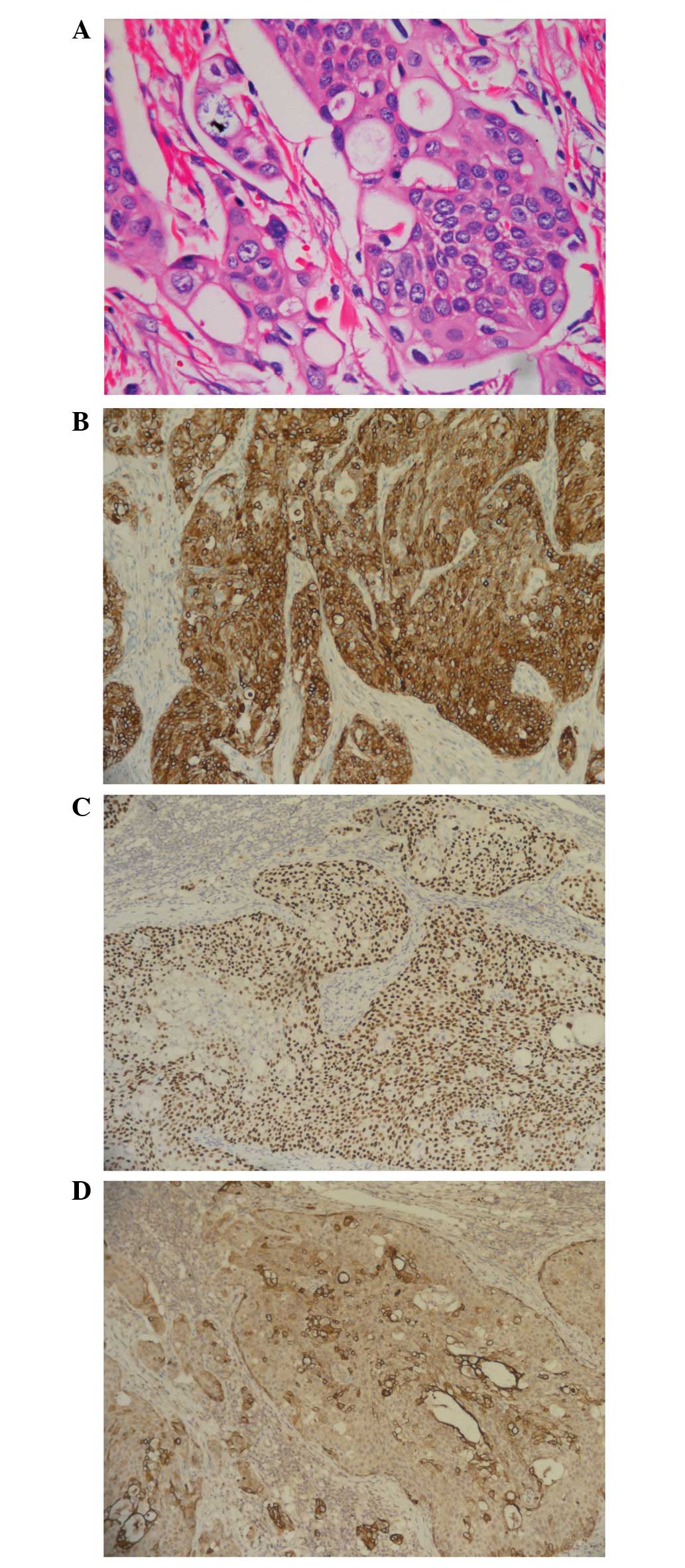
pancreatic tumor was comprised of poorly differentiated cells with
vascular and perineural invasion and infiltrating submucosa of
duodenum (Fig. 4A). The tumor cells
in the pancreas were immunoreactive for cytokeratin 5/6 (CK5/6),
p63 and CAM5.2, supporting the diagnosis of ASC (Fig. 4B–D). None of the nine peripancreatic
lymph nodes were involved. Ultimately, the pathological TNM staging
was pT3N0M0.
The postoperative course was uneventful. The patient
declined any further adjuvant therapy, and 6 months following
therapy the patient remains healthy and has experienced no tumor
recurrence.
Discussion
GISTs are the most common type of mesenchymal
neoplasm of the gastrointestinal tract. Primary GISTs are usually
solitary, but may occur in groups, e.g. Carney’s triad or when
associated with neurofibromatosis. Without the presence of Carney’s
triad or neurofibromatosis syndromes, synchronous occurrence of a
GIST with a tumor of different histological type is rare and has
been documented in the literature mainly in the form of case
reports. Malignances of the gastrointestinal tract are the most
commonly accompanied neoplasms; however, there are few previous
studies concerning synchronous pancreatic cancer and GIST in the
stomach (8,9). Liu et al reported that the most
common epithelial tumors associated with GIST in their series were
esophageal squamous cell carcinomas (1.13%), followed by gastric
(0.53%), pancreatic (0.38%) and colorectal (0.03%) adenocarcinomas
(9).
Compared with a GIST alone, synchronous GISTs have
various clinical manifestations. Agaimy and Wuensch analyzed a
series of 97 cases of surgically resected GIST and revealed that
the majority of GISTs in their series were benign or low-risk and
appeared to be innocent bystanders (2). Liszka et al identified that
these GISTs tended to be an incidental findings during surgery, and
were most commonly localized in the small intestine (10). In our case, the GIST was associated
with an intermediate risk and located in the stomach.
ASC of the pancreas is also referred to as
adenoacanthoma, mixed squamous adenocarcinoma and mucoepidermoid
carcinoma. Radiographically, ASC cannot be distinguished from
adenocarcinoma (11); thus, a
pathological diagnosis may be made through biopsy or during
surgery. Few patients undergo surgical resection as the majority of
patients have stage IV disease at the time of presentation. When
resected, ASC is frequently associated with positive lymph nodes,
vascular and perineural invasion and poor tumor cell
differentiation (12).
Patients with ASC have a worse survival rate
compared with those with adenocarcinoma. Smit et al
demonstrated that the average survival of 72 patients with ASC of
the pancreas was 5.7 months, and only five patients survived for
longer than one year (13). Kardon
et al identified that the overall survival was 12.5 months
in patients treated with curative resection and adjuvant
chemotherapy, and was 3.0 months in patients who received no
chemotherapy or received palliative chemotherapy (14). To date, surgical resection offers
the only chance for a cure. Boyd et al recently revealed
that the resectability is the strongest predictor of survival in
ASC (15). Katz et al
demonstrated an improvement in survival with the use of palliative
radiation and chemotherapy; however, the benefit of adjuvant
chemoradiation was not supported by this study (16). There is no current standard of
chemotherapy regimens for patients with ASC, but it has been
suggested that ASC of the pancreas is sensitive to
platinum-containing chemotherapy regimens (17,18).
The preoperative pathological diagnosis of ASC is
often difficult. The carcinoma arising from the uncinate process
has unique clinical manifestations due to its anatomical location,
and the clinical presentation of CUPP is often late as a result of
the lack of obstructive jaundice as a presenting feature. More
common symptoms including abdominal pain and weight loss occur in
up to 70% of all cases. Due to its tendency to cause duodenal
obstruction, vomiting, as observed in our patient, is also a common
clinical presentation. Due to the anatomical position of the
uncinate process, ultrasound imaging of this area is likely to be
obscured by the overlying bowel; therefore, CT is the main
diagnostic method (6).
Additionally, CUPP commonly involves superior mesentery vessels,
making it unresectable or leading to margin-positive resection.
The overall survival in CUPP is less than that of
the adenocarcinoma in the head of the pancreas. Ye et al
identified a one-year survival rate of 37.7% and a 5-year survival
rate of 5.6% for all stages of CUPP (19). Li et al revealed that
resected CUPPs had a median survival of 17 months. Those patients
who did not have venous resection had a median survival of 19
months, while those with venous resection had a median survival of
13 months (20). Thus, a delay in
clinical presentation and the anatomical location of CUPP in
relation to the retroperitoneum and mesenteric vessels appears to
account for lower resection rates and reduced overall survival.
Contrary to the majority of previous cases of
synchronous GISTs and other malignancies (9,10), and
the other case report of synchronous GIST and pancreatic
adenocarcinoma (8), in our case,
GIST was not an incidental finding. Our initial impression was a
symptomatic GIST; however, following reevaluation via a CT scan
with a multidisciplinary approach, a pancreatic adenocarcinoma was
suspected. Thus, the intraoperative exploration of the pancreas and
the pancreatoduodectomy was preoperatively planned.
References
|
1.
|
P EfstathiosP AthanasiosI
PapaconstantinouCoexistence of gastrointestinal stromal tumor
(GIST) and colorectal adenocarcinoma: a case reportWorld J Surg
Oncol596200710.1186/1477-7819-5-9617708776
|
|
2.
|
A AgaimyPH WuenschGastrointestinal stromal
tumours in patients with other-type cancer: a mere coincidence or
an etiological association? A study of 97 GIST casesZ
Gastroenterol4310251030200510.1055/s-2005-858378
|
|
3.
|
M MiettinenJ LasotaGastrointestinal
stromal tumors - definition, clinical, histological,
immunohistochemical, and molecular genetic features and
differential diagnosisVirchows
Arch438112200110.1007/s004280000338
|
|
4.
|
JA MaduraBT JarmanMG DohertyMN YumTJ
HowardAdenosquamous carcinoma of the pancreasArch
Surg134599603199910.1001/archsurg.134.6.59910367867
|
|
5.
|
K YamaguchiCarcinoma of the uncinate
process of the pancreas with a peculiar clinical manifestationAm J
Gastroenterol871046105019921642209
|
|
6.
|
D BirkMH SchoenbergF GansaugeA FormentiniG
FortnagelHG BegerCarcinoma of the head of the pancreas arising from
the uncinate processBr J
Surg85498501199810.1046/j.1365-2168.1998.00629.x9607531
|
|
7.
|
T SuzukiH KuratsukaK UchidaY MatsumotoI
HonjoCarcinoma of the pancreas arising in the region of the
uncinate
processCancer30796800197210.1002/1097-0142(197209)30:3%3C796::AID-CNCR2820300330%3E3.0.CO;2-O5075362
|
|
8.
|
CA DasanuT MesologitesG
TrikudanathanSynchronous tumors: adenosquamous carcinoma of
pancreas and GIST of stomachJ Gastrointest
Cancer42186189201110.1007/s12029-010-9187-320623381
|
|
9.
|
YJ LiuZ YangLS HaoL XiaQB JiaXT
WuSynchronous incidental gastrointestinal stromal and epithelial
malignant tumorsWorld J
Gastroenterol1520272031200910.3748/wjg.15.202719399938
|
|
10.
|
L LiszkaE Zielinska-PajakJ PajakD GolkaJ
HusznoCoexistence of gastrointestinal stromal tumors with other
neoplasmsJ
Gastroenterol42641649200710.1007/s00535-007-2082-417701127
|
|
11.
|
T OkabayashiK HanazakiSurgical outcome of
adenosquamous carcinoma of the pancreasWorld J
Gastroenterol1467656770200810.3748/wjg.14.676519058301
|
|
12.
|
KR VoongJ DavisonTM PawlikResected
pancreatic adenosquamous carcinoma: clinicopathologic review and
evaluation of adjuvant chemotherapy and radiation in 38 patientsHum
Pathol41113122201010.1016/j.humpath.2009.07.012
|
|
13.
|
W SmitJP MathyE DonaldsonPancreatic
cytology and adenosquamous carcinoma of the
pancreasPathology25420422199310.3109/003130293090908738165013
|
|
14.
|
DE KardonLD ThompsonRM PrzygodzkiCS
HeffessAdenosquamous carcinoma of the pancreas: a clinicopathologic
series of 25 casesMod
Pathol14443451200110.1038/modpathol.388033211353055
|
|
15.
|
CA BoydJ Benarroch-GampelKM SheffieldCD
CooksleyTS Riall415 patients with adenosquamous carcinoma of the
pancreas: a population-based analysis of prognosis and survivalJ
Surg Res1741219201110.1016/j.jss.2011.06.01521816433
|
|
16.
|
MH KatzTH TaylorWB Al-RefaieAdenosquamous
versus adenocarcinoma of the pancreas: a population-based outcomes
analysisJ Gastrointest
Surg15165174201110.1007/s11605-010-1378-521082275
|
|
17.
|
G AurilioT MacarullaJF RamosN FazioF NolèC
IglesiasSuccessful treatment with GEMOX in patient with metastatic
pancreatic adenosquamous carcinomaTumori97239242201121617724
|
|
18.
|
R WilkowskiS BoeckS
OstermaierChemoradiotherapy with concurrent gemcitabine and
cisplatin with or without sequential chemotherapy with
gemcitabine/cisplatin vs chemoradiotherapy with concurrent
5-fluorouracil in patients with locally advanced pancreatic cancer
- a multi-centre randomised phase II studyBr J
Cancer101185318592009
|
|
19.
|
C YePC XiXG HuClinical analysis of
uncinate process carcinoma of the pancreasHepatobiliary Pancreat
Dis Int2605608200314627529
|
|
20.
|
S LiYQ PeiFT DuSurgical treatment for
uncinate process carcinoma of the pancreasHepatobiliary Pancreat
Dis Int1592594200214607693
|