Introduction
Adenomas of the adrenal cortex are usually
asymptomatic and are discovered incidentally, when the diameter is
3–3.5 cm (1). Evidence has revealed
that the risk of malignancy increases with increasing tumor size
(2,3). Between 45 and 100% of adrenal tumors
that are over 4 cm in diameter are diagnosed as malignant (4). Adrenocortical carcinomas are typically
large at diagnosis, ranging from 3 to 20 cm in diameter, with
distant metastases occurring in 20–50% of these cases (2).
Case report
In the present study, we describe the case of a
54-year-old female who was admitted to the Department of
Oncosurgery at Anyang Tumor Hospital, Henan, China, with complaints
of nonspecific right-sided upper abdominal pain accompanied with
vomiting. These symptoms had commenced approximately 24 h earlier.
Four months previously, an asymmetric distended abdomen had been
observed. The patient’s medical history was insignificant and there
had been no external trauma in the days prior to admission.
Accompanied with haphalgesia, asymmetry in the abdomen and a right
upper abdominal huge mass was discovered during a routine physical
examination. The examination of the heart and lungs was
unremarkable. No Cushing’s syndrome features were observed.
Laboratory parameters including tumor markers were
all within the normal range. Ultrasonography demonstrated a solid
mass in the right liver that measured 25x14.5 cm and was suggestive
of an hepatic lesion. A mass in the right adrenal area, which made
the right kidney lower than usual, was observed by intravenous
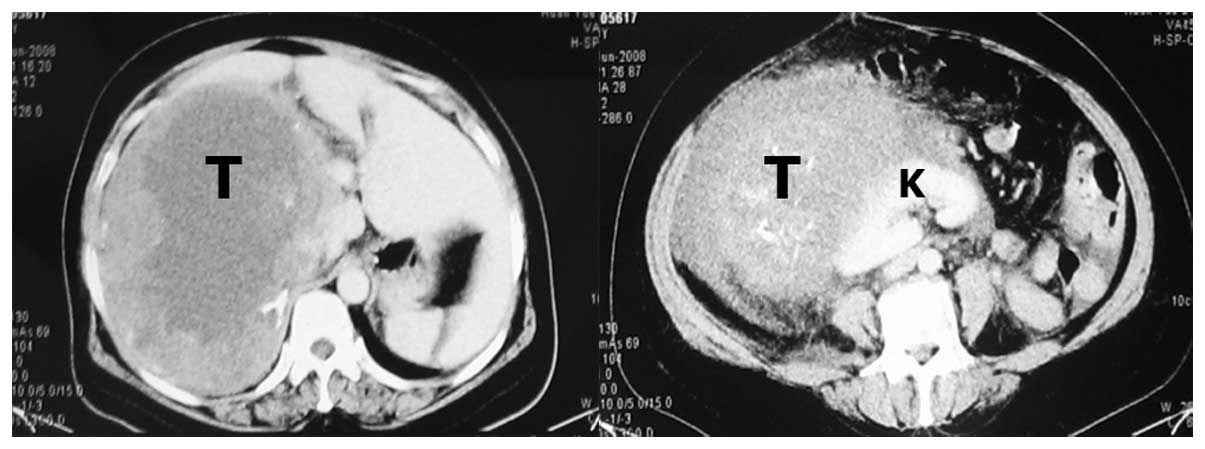
pyelography. A computed tomography scan revealed a
well-circumscribed mass of approximately 25 cm in diameter (25x20
cm) in the right liver which was smooth at the edge and had
low-density imaging in the central tumor area. The right kidney,
positioned lower than the normal location, was also observed
(Fig. 1).
A retroperitoneal tumor was suspected. Surgical
exploration was performed under general anesthesia. During surgery,
a large tumor, which was covered with vessels, was found to occupy
the area from the inferior part of the liver to the iliac
bifurcation. Right hepatic lobe atrophy was found. The right kidney
was compressed and situated at the bifurcation of the right iliac
total artery. Vascular and capsular invasion were not present.
Complete resection of the lesion was performed. The patient’s blood
pressure and heart rhythm were stable during surgery. The
post-operative course was unremarkable. The patient was
asymptomatic when discharged 9 days after the operation.
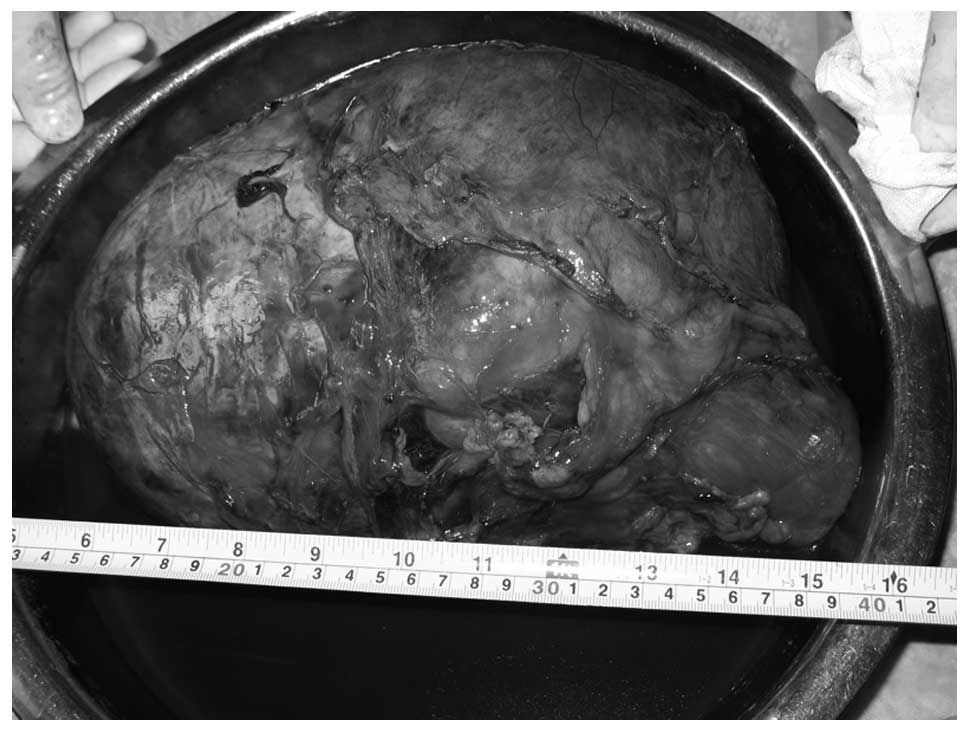
Pathological examination revealed a centrally
hemorrhagic tumor, 35x25x11 cm in size and weighing 7,500 g,
surrounded by a thick fibrous capsule (Fig. 2). There was little normal adrenal
tissue remaining. Necrosis and hemorrhage was observed in the
central area of the tumor. Histologically, the tumor was composed
of monomorphic clear cells with abundant microvesicular cytoplasm,
which were arranged in trabecular or cord-like structures. The
tumor cell nuclei were small and round and mitosis was rare.
Fibrosis, adipose tissue and infiltration of multinucleated giant
cells were found in limited areas.
The study was approved by the Ethics Committee of
Anyang Tumor Hospital and Anyang Hygiene Bureau, China. Informed
consent was obtained from the patient.
Discussion
Unilateral tumors or masses of the adrenal gland are
common. They are categorized as functional or nonfunctional, and as
benign or malignant. The majority of adrenocortical tumors are
benign, nonfunctioning adenomas that are discovered incidentally on
abdominal imaging studies (5).
Others are benign, hormone-secreting adenomas that cause Cushing’s
syndrome, primary aldosteronism or much less commonly,
virilization. Following the initial discovery of an adrenal mass,
subsequent evaluation should determine whether it is benign or
malignant and whether it is functional or nonfunctional, in order
to determine treatment options.
Adrenal adenomas are common, benign adrenocortical
tumors, with a diameter of 3–3.5 cm (1) and an incidence of 2.86% (6). When adrenal adenomas are very large,
it is difficult to distinguish an adenoma from a carcinoma.
Adrenocortical carcinomas are rare, extremely aggressive tumors
that may be functional and are discovered as a result of the
appearance of an abdominal mass or as an incidental finding. The
differential diagnosis between malignant and benign tumors of the
adrenal cortex can be difficult before surgery. The criteria for
malignancy are distant metastases and/or local invasion. However,
compared to adenomas, carcinomas are usually larger and occur at
any age, including in children. According to previous reports, the
risk of malignancy increases with increasing tumor size and the
majority of tumors that were over 4 cm in diameter were diagnosed
as malignant (7,8). In our study, the tumor was 35x25x11 cm
in size, so the tumor should be diagnosed as malignant. However, in
1984, Weiss proposed that the presence of three or more of the
following features was significant criteria for malignant clinical
behavior: nuclear grade III or IV, mitotic rate >45/50
high-power fields, atypical mitoses, clear cells constituting
<25%, more than 1/3 diffuse architecture, necrosis, sinusoidal,
venous and capsular invasion (9,10).
Referring to this criteria proposed by Weiss, the case we reported
belongs to the benign category. In agreement with our study,
Denzinger et al reported an adenoma of the adrenal cortex
with a diameter of 18 cm, which ruptured spontaneously (2). Masugi et al also described a
case of non-functional adrenocortical adenoma with a diameter of
5.5 cm (11). Thus, it was not
surprising that the present tumor proved to be benign.
In summary, to the best of our knowledge, this is
the largest case of nonfunctional adrenocortical adenoma reported
to date. Careful clinical work and histopathological examination
may help in determining the dignity of adrenocortical tumors,
although difficulty remains in differentiating benign from
malignant adrenal tumors, particularly in large tumors without
invasive features and cellular atypia.
Acknowledgements
This study was supported by Grants
from the National Natural Science Foundation of China (nos.
81071960) and New Teacher Foundation of Ministry of Education,
China (no. 20100101120129).
References
|
1
|
Mantero F and Arnaldi G: Management
approaches to adrenal incidentalomas. A view from Ancona, Italy.
Endocrinol Metab Clin North Am. 29:107–125. ix2000. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Denzinger S, Burger M, Hartmann A,
Hofstaedter F, Wieland WF and Ganzer R: Spontaneous rupture of a
benign giant adrenal adenoma. APMIS. 115:381–384. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Medeiros LJ and Weiss LM: New developments
in the pathologic diagnosis of adrenal cortical neoplasms. A
review. Am J Clin Pathol. 97:73–83. 1992.PubMed/NCBI
|
|
4
|
Francis IR, Smid A, Gross MD, Shapiro B,
Naylor B and Glazer GM: Adrenal masses in oncologic patients:
functional and morphologic evaluation. Radiology. 166:353–356.
1988. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Miyamori I: Clinical aspect of adrenal
incidentaloma. Nihon Rinsho. 62:925–928. 2004.(In Japanese).
|
|
6
|
Dunnick NR: Hanson lecture. Adrenal
imaging: Current status. AJR Am J Roentgenol. 154:927–936. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bertagna C and Orth DN: Clinical and
laboratory findings and results of therapy in 58 patients with
adrenocortical tumors admitted to a single medical center (1951 to
1978). Am J Med. 71:855–875. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Nishikawa T, Saito J and Omura M: Mini
review: surgical indications for adrenal incidentaloma. Biomed
Pharmacother. 56(Suppl 1): 145s–148s. 2002.PubMed/NCBI
|
|
9
|
Weiss LM: Comparative histologic study of
43 metastasizing and nonmetastasizing adrenocortical tumors. Am J
Surg Pathol. 8:163–169. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Weiss LM, Medeiros LJ and Vickery AL Jr:
Pathologic features of prognostic significance in adrenocortical
carcinoma. Am J Surg Pathol. 13:202–206. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Masugi Y, Kameyama K, Aiba M, Mukai M,
Hara S, Ohigashi T and Murai M: Non-functional adrenocortical
adenoma with extensive degeneration. Pathol Int. 53:241–245. 2003.
View Article : Google Scholar : PubMed/NCBI
|