Introduction
Ca2+, a ubiquitous signal ion, controls a
series of physiological processes, including cell proliferation,
metabolism and gene transcription. Ca2+ signalling is
essential for all eukaryote cells, including cancer cells, to grow
and proliferate (1). Altered
expression of specific Ca2+ channels and pumps causes
over-sufficiency in growth signals, promoting cancer cell
proliferation (2). Studies
evaluating the ability of Ca2+ to regulate cell death
and proliferation present an opportunity for a new set of drug
targets in cancer (2,3).
Tumor cells are non-excitable cells with few
voltage-gated Ca2+ channels, among which the transient
receptor potential (TRP) channels have been recognized as the main
Ca2+ entry pathway (4).
Transient receptor potential melastatin 7 (TRPM7), one member of
the TRPM channel subfamily of TRP channels, has been shown to be
present in human head and neck squamous carcinoma FaDu and SCC25
cells. Suppression of TRPM7 expression or blockage of TRPM7
currents leads to inhibition of the growth and proliferation of
FaDu and SCC25 cells (5), which may
provide an opportunity for therapeutic intervention.
In the present study, the levels of TRPM7 were
pharmacologically manipulated, in order to use its downregulation
as a tool to repress the cell proliferation of FaDu cells. The aim
was to test whether midazolam [molecular weight 325.77, a
clinically widely-used benzodiazepine (BZ) anesthetic] inhibits
cell growth and proliferation by repressing TRPM7 expression in
FaDu cells. We also aimed to determine whether this effect was
unique to midazolam or common to benzodiazepines. We propose that
the present results, showing the proliferation-inhibitory activity
of midazolam, not only lay a theoretical foundation for the
preferential use of midazolam as the anesthetic during tumorectomy,
but also identify TRPM7 as a therapeutic target for cancer.
Materials and methods
Antibodies and reagents
Midazolam, diazepam, clonazepam and flumazenil were
purchased from Nhwa Pharmaceutical Group (Jiangsu, China). PK11195
was obtained from Sigma, (St. Louis, MO, USA). Antibodies against
cyclin D1, cyclin E, P21, P27, Rb and phosphorylated Rb were
obtained from Cell Signaling Technology (1:1,000; Beverly, MA,
USA), while tubulin antibody (1:5,000) was obtained from Sigma and
CDK 2, 4 and 6 antibodies were purchased from Santa Cruz
Biotechnology (1:500; Santa Cruz, CA, USA).
Cell culture
FaDu human hypopharyngeal squamous cell carcinoma
cells (ATCC HTB-43), were maintained in Eagle’s MEM with 10% fetal
bovine serum (FBS; Invitrogen, Grand Island, NY, USA), 50 U/ml
penicillin and 50 μg/ml streptomycin. Cells were cultured in
a 5% CO2 humidified atmosphere at 37°C. The study was
approved by the Ethics Committee of Sun Yat-sen University,
Guangzhou, China.
Cell viability assay
The cell viability assay was performed with MTT
(Sigma). Cells were seeded in 96-well plates and the initial cell
number was adjusted to 3,000/well. Following drug treatment, 20
μl MTT (5 mg/ml in PBS) was added to the medium to induce
the production of formazan crystals. After 4 h, the MTT solution
was aspirated off and 100 μl dimethyl sulfoxide (Sigma) was
added to solubilize the formazan crystals. The optical density (OD)
was determined at 570 nm using an iMark™ Microplate Reader
(Bio-Rad, Richmond, CA, USA). The cell viability rate =
ODtreatment / ODcontrol (vehicle) × 100.
Cell proliferation assay
For the cell proliferation assay, a cell
proliferation ELISA kit for the thymidine analog
5-bromo-2′-deoxyuridine (BrdU; Roche Diagnostics, Mannheim,
Germany) was used as per the manufacturer’s instructions. In brief,
cells were seeded in 96-well plates and the initial cell number was
adjusted to 3,000/well. Following drug treatment, the cells were
labeled with BrdU for 4 h. Subsequently, anti-BrdU-POD Fab
fragments and substrate were added to the medium. The optical
density (OD) was determined at 405 nm using an iMark Microplate
Reader. The results were normalized to the control (the group
treated with vehicle).
Cell death assay
Cell death was evaluated using a lactate dehydro
genase (LDH) release assay. LDH release was quantified with a
CytoTox 96 non-radioactive cytotoxicity assay kit (Promega,
Madison, WI, USA) according to the manufacturer’s instructions.
Cells were seeded in 96-well plates and the initial cell number was
adjusted to 3,000/well. Following drug treatment, 50 μl
medium/well was transferred to another 96-well plate. The solution
of LDH substrate (50 μl) was added to the medium and
incubated for 30 min. Subsequently, 50 μl stop solution was
added to stop the reaction and the absorbance was measured at 490
nm with an iMark Microplate Reader. The results were normalized to
the control (the group treated with vehicle).
Cell cycle analysis
After 24 h of serum starvation, the cells were
exposed to the complete medium with 10% FBS. Following treatment,
the cells were harvested by trypsinization, washed twice with cool
PBS and fixed in 75% ethanol overnight at 4°C. Subsequently, the
cells were incubated in solution with 50 mg/ml DNA-binding dye PI,
4 kU/ml RNase, 0.3 mg/ml NaF and 1 mg/ml sodium citrate for 30 min
at 37°C away from light. Finally, the red fluorescence from the 488
mm laser-excited PI in every cell was analyzed with an EPICS ALTRA
flow cytometer (Beckman Coulter, Fullerton, CA, USA) using a peak
fluorescence gate to discriminate aggregates. The percentages of
cells in the G0/G1, S and G2/M
phases were determined from DNA content histograms using Multicycle
for Windows (Phoenix Flow Systems, San Diego, CA, USA).
Western blot analysis
Western blot analysis was performed as described
previously (6). In brief, cells
were scraped and then resuspended in protein extraction reagent.
The cell lysate was centrifuged at 140,000 g for 10 min at 4°C and
the supernatant was collected for electrophoresis. Prior to
electrophoresis, the concentration of protein was determined using
a BCA protein assay kit (Pierce, Rockford, IL, USA) following the
manufacturer’s instructions. Equal amounts of proteins (30
μg) were separated by 12% SDS-PAGE. After electrophoresis,
the proteins were transferred to PVDF membranes, blocked with 5%
skimmed milk in TBS for 2 h and reacted with antibodies overnight.
After reaction with horseradish peroxidase-labeled secondary
antibody, the immune complexes were visualized using the
ECL-detection reagents according to the manufacturer’s
instructions.
Quantitative real-time PCR (qPCR)
Total RNA was extracted with TRIzol reagent
(Invitrogen, Carlsbad, CA, USA) according to the manufacturer’s
instructions. The purity and integrity of all isolated RNA samples
was analyzed using agarose gel electro phoresis. The first strand
of the cDNA was synthesized using SuperScript III reverse
transcriptase (Invitrogen) with an oligo(dt) primer. The sequences
of the PCR primers used were as follows: TRPM7, 5′-TGC AGC AGA GCC
CGA TAT TAT-3′ (sense primer) and 5′-CTC TAT CCC ATG CCA ATG TAA
GG-3′ (antisense primer); GAPDH, 5′-TCA CCA TCT TCC AGG AGC GAG
A-3′ (sense primer) and 5′-ATG AGC CCT TCC ACG ATG C-3′ (antisense
primer). qPCR was performed with Platinum SYBR-Green qPCR
SuperMix-UDG (Invitrogen) and detected with a LightCycler 480
(Roche, Basel, Switzerland). The comparative CT method
(2−ΔΔCT) was used to evaluate the relative
quantities.
Statistical analysis
Data are presented as the mean ± standard deviation
(SD) of at least three separate experiments. The statistical
significance was determined by ANOVA analysis. P<0.05 was
considered to indicate a statistically significant difference.
Results
Midazolam inhibits the growth and
proliferation of FaDu cells
To examine whether midazolam affects the growth of
human hypopharyngeal squamous cell carcinoma FaDu cells, the
changes in morphology and cell number of FaDu cells treated with
100 μM midazolam were observed by phase-contrast microscopy.
As shown in Fig. 1A, the bodies of
the majority of cells exposed to midazolam appeared to be smaller
than the controls and the cell number was significantly lower,
indicating that midazolam inhibits the growth of FaDu cells. The
MTT assay used to measure the relative counts of live cells showed
that midazolam treatment for 24 h decreased the cell viability
which was evident at 50 and 100 μM. By 48 h, the cell
viability had decreased at 6.25 μM and been reduced to 47.1%
at 100 μM (Fig. 1B). To
further investigate whether cell viability loss by midazolam was
due to proliferative inhibition or cell death, the relative levels
of BrdU incorpration representing cell proliferation and LDH
release representing cell death were measured in FaDu cells treated
with 25, 50 and 100 μM midazolam. The data from Fig. 1C and D showed that midazolam
dose-dependently reduced BrdU incorpration but did not trigger LDH
release. Therefore, midazolam induced cell viability loss by
inhibiting cell proliferation in FaDu cells.
 | Figure 1Midazolam inhibited the growth and
proliferation of FaDu cells. (A) Phase-contrast image of cells
treated with 0 (control) and 100 μM mida zolam for 48 h
(original magnification, ×200). (B) Dose- and time-dependent effect
of midazolam on cell viability. FaDu cells were incubated with 0,
6.25, 12.5, 25, 50 and 100 μM midazolam for 24 and 48 h. The
data are the mean ± SD (n=5), **P<0.01 compared with
the control. Effects of midazolam on (C) cell proliferation by BrdU
incorporation assay and (D) cell death by lactate dehydrogenase
(LDH) release assay. FaDu cells were incubated with 25, 50 and 100
μM midazolam for 48 h. The data are the mean ± SD (n=3),
*P<0.05, **P<0.01, compared with the
control. |
Midazolam triggers
G0/G1 cell cycle arrest by regulating cell
cycle regulators
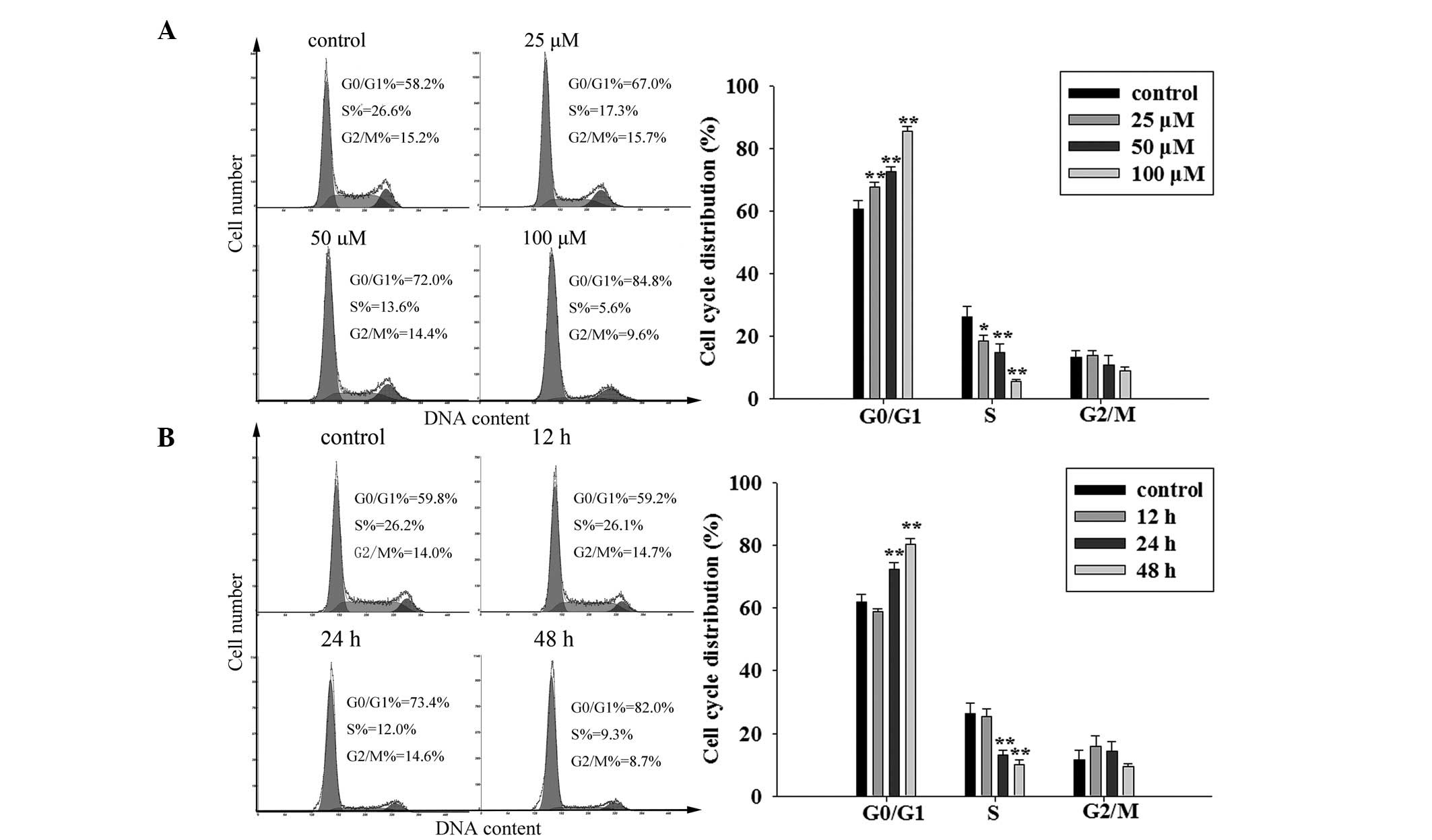
The cell cycle distribution determines the rate of
cell proliferation. Generally, the percentage of cells in the S
phase reflects the quantity of proliferating cells. Cancer cells
are abnormal cells which have lost their balance of proliferation
and apoptosis so the percentage in S phase is much larger than that
of normal cells from the same tissues or organs (7). The data from three independent cell
cycle analyses showed that midazolam reduced the mean S phase
percentage from 26.1 to 18.4, 15.0 and 5.7% at concentrations of
25, 50 and 100 μM, respectively. The mean
G0/G1 phase percentage climbed from 60.5 to
67.7, 72.5 and 85.3% (at 25, 50 and 100 μM midazolam,
respectively), while no statistically significant differences were
observed in the mean M phase percentages (Fig. 2A). In addition, the cell cycle
distributions of FaDu cells in response to midazolam treatment for
12, 24 and 48 h were analyzed. The results showed that
G0/G1 phase arrest induced by midazolam had
begun by 24 h and was greater by 48 h (Fig. 2B). These data suggest that midazolam
hinders the cells’ progression from G1 to S phase and
that the checkpoint of the G1/S phase transition may be
affected by midazolam.
The checkpoint is composed of cyclin D1 and E,
cyclin-dependent kinase (CDK) 2, 4 and 6 (cyclin/CDK complex), p21
and p27 (CDK inhibitors), and Rb (a determinant of E2F1 release).
Western blot analysis revealed that p21 and p27 proteins were
significantly upregulated, while the total and phosphorylated Rb
(active type) were markedly decreased, although the other proteins
did not noticeably change (Fig 3).
The data indicate that the reduction of active Rb is the main
contributor to G0/G1 cell cycle arrest by
midazolam.
 | Figure 3Midazolam prevented Rb activation by
affecting the expression of cell cycle regulators. (A) Effect of
midazolam on protein levels of Rb, phosphorylated Rb (p-Rb), p21,
p27, cyclin D1, cyclin E, CDK2, CDK4 and CDK6. (B) Statistical
graph of three independent experiments. Gray scales of proteins
were normalized to housekeeping genes (tubulin, β-actin and GAPDH)
and data are presented as values relative to the control. FaDu
cells were treated with 0 (control), 25, 50 and 100 μM
midazolam for 48 h and then subjected to western blot analysis. The
data are the mean ± SD (n=3), *P<0.05,
**P<0.01, compared with the control. |
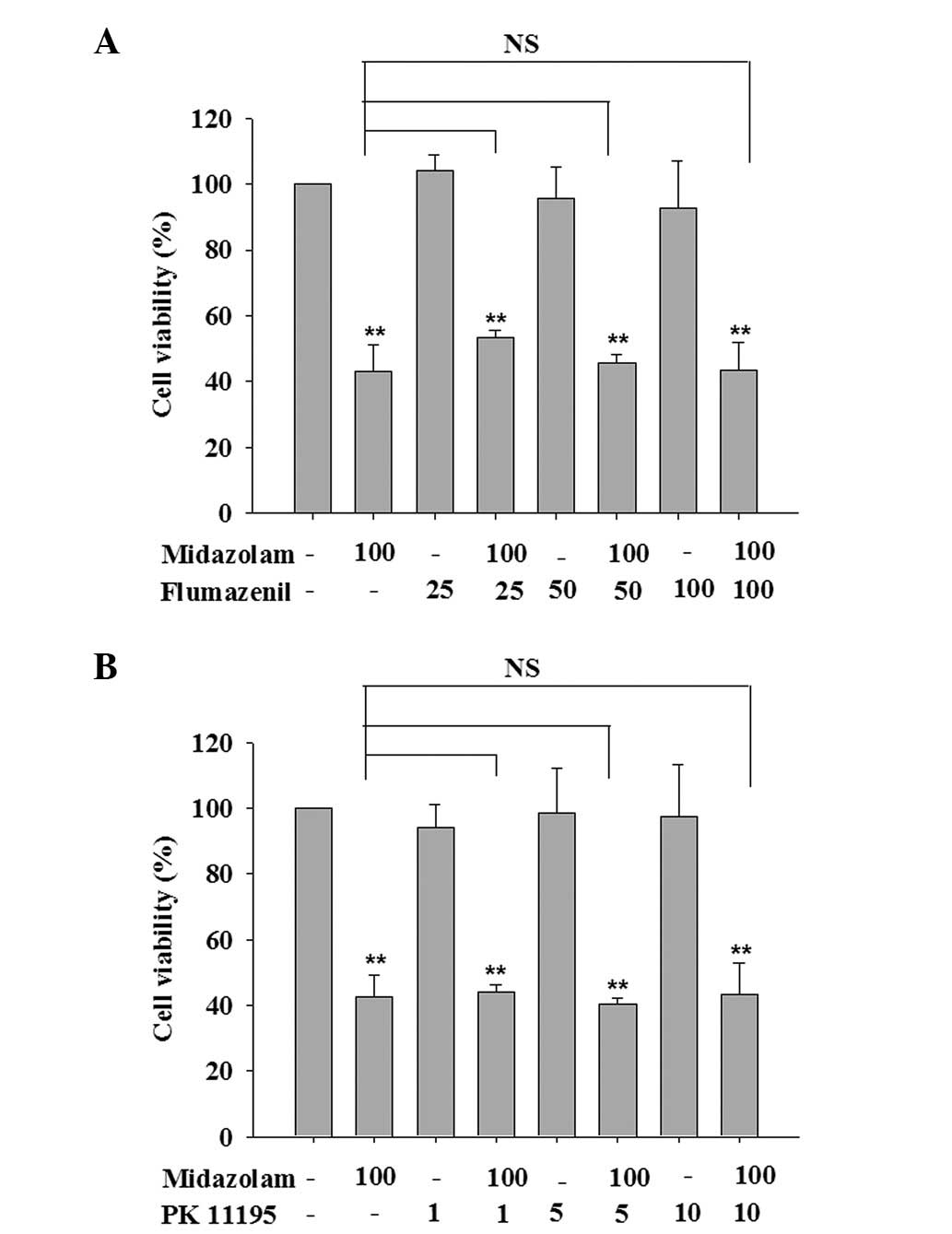
Proliferation-inhibitory effect of
midazolam is benzodiazepine receptor (BR)-independent but
TRPM7-dependent
The nervous system-inhibitory activity of midazolam
is known to be mediated by BRs, including central-type BZ receptor
(CBR) and peripheral-type benzodiazepine receptor (PBR). To
determine the mechanism underlying the proliferation-inhibitory
effect of midazolam, the role of CBR and PBR in this non-nervous
system activity had to be clarified. Thus, the specific CBR
antagonist flumazenil and PBR antagonist PK11195 were used to
compete with midazolam to bind to CBR or PBR. At a concentration
range within which cell viability was not affected, flumazenil
(25–100 μM) and PK11195 (1–10 μM) were unable to
reverse the proliferation loss induced by midazolam (Fig. 4). This result suggests that the
mechanism underlying midazolam-induced FaDu cell proliferation is
BR-independent.
Based on the evidence that TRPM7 exists in FaDu
cells and silencing the TRPM7 channel inhibits cell proliferation
(5), it was investigated whether
the anti-proliferative activity of midazolam is mediated by the
inhibition of TRPM7 expression. As shown in Fig. 5A, the data from the RT-qPCR analysis
showed that the addition of 25, 50 and 100 μM midazolam to
the medium decreased the mRNA level of TRPM7 by 21.5, 43.8 and
58.7%, respectively. Subsequently, bradykinin, a TRPM7 channel
activator, was used to examine whether the activation of TRPM7
abrogates the inhibition of proliferation by midazolam in FaDu
cells. Fig. 5B shows that the
addition of 200 μM bradykinin with 50 μM midazolam in
the culture medium reversed the inhibition of cell growth by
midazolam, suggesting that TRPM7 inhibition contributes to the
inhibitory effect of midazolam on cell growth and proliferation.
Furthermore, the effect of 2-APB, a non-specific TRPM7 inhibitor,
on the proliferation of FaDu cells was evaluated. As shown in
Fig. 5C, 2-APB also inhibited the proliferation of
FaDu cells and the combined effect of 2-APB and midazolam appeared
to be additive for inhibiting cell growth.
 | Figure 5Anti-proliferative activity of
midazolam was mediated by suppression of TRPM7. (A) Midazolam
repressed the transcriptional expression of TRPM7 dose-dependently.
FaDu cells were treated with 0 (control), 25, 50 and 100 μM
midazolam for 48 h and then subjected to qPCR. (B) Bradykinin, a
specific TRPM7 activator, reversed the proliferation inhibition by
midazolam. (C) 2-APB, a non-specific TRPM7 inhibitor also inhibited
cell proliferation and enhanced the effect of midazolam. FaDu cells
were treated with 50 μM midazolam and co-cultured with
bradykinin (200 μM) or 2-APB (25, 50, 100 and 200 μM)
for 48 h. The data are the mean ± SD (n=3), *P<0.05,
**P<0.01, compared with the control and
#P<0.05, ##P<0.01, compared with the
group treated with 2-APB. TRPM7, transient receptor potential
melastatin 7; qPCR, quantitative real-time PCR. |
Taken together, these results indicate that the
anti-proliferative activity of midazolam was independent of the
classic BR pathway but dependent on TRPM7 inhibition.
Diazepam and clonazepam also exhibit
inhibitory activities on the proliferation of FaDu cells
To confirm whether midazolam-induced proliferation
loss is unique, the effects of other available BZs, including
diazepam and clonazepam, on the cell proliferation of FaDu cells
were investigated. Similar to midazolam, diazepam and clonazepam
exhibited potent anti-proliferative activities at almost the same
concentration range (25–100 μM). Cell survival analysis
showed that diazepam exhibited anti-growth activity at 24 h which
became more evident at 48 h and cell viability was decreased by
19.9, 26.5 and 47.2% with 25, 50 and 100 μM diazepam,
respectively (Fig. 6A). In response
to 25, 50 and 100 μM clonazepam, the cell viabilities were
16.7, 38.3 and 44.8%, respectively (Fig. 6B). BrdU incorporation assays also
provided evidence that diazepam and clonazepam significantly
repressed cell proliferation (Fig. 6C
and D).
 | Figure 6Diazepam and clonazepam also induced
proliferation loss in FaDu cells. (A) Time and (B) dose-dependent
effects of diazepam and clonazepam on cell viability according to
MTT assays. FaDu cells were incubated with 0 (control), 6.25, 12.5,
25, 50 and 100 μM midazolam for 24 and 48 h. The data are
the mean ± SD (n=5), *P<0.05, **P<0.01
compared with the control. Effects of (C) diazepam and (D)
clonazepam on cell proliferation according to BrdU incorporation
assays. FaDu cells were incubated with 0, 25, 50 and 100 μM
midazolam for 48 h. The data are the mean ± SD (n=3),
*P<0.05, **P<0.01, compared with the
control. |
Discussion
In cancer cells, TRP ion channels, in combination
with Ca2+ pumps and exchangers, maintain cellular
Ca2+ homeostasis by driving the influx of
Ca2+ across the plasma membrane into the cell (8–10). The
ability of TRP channels to regulate [Ca2+]i and
Ca2+-dependent tumorigenic pathways, such as
proliferation, suggests that therapies modulating TRP channels in
cancer cells may be a therapeutic option. Among the members of the
TRP families, the TRP vanilloid (TRPV) 6, TRPM1 and 8 channels are
most commonly reported to be associated with malignant cell growth
and cancer progression (4,11). An accumulating amount of data shows
that TRPM7 also acts as a promoter of proliferation, migration and
even carcinogenesis in lung carcinoma, pancreatic carcinoma and
breast cancer (12–14). This suggests the potential of TRPM7
as a valuable target for the pharmaceutical intervention of cancer.
Evidence demonstrating the presence of TRPM7 in human
hypopharyngeal squamous cell carcinoma FaDu cells (5), leads to the present study targeting
TRPM7 with BZs. The present study suggests the potential
exploitation of the anesthetic drug midazolam as a TRPM7 inhibitor.
In FaDu cells, midazolam induced cell cycle arrest and thus
proliferation loss by a TRPM inhibition-dependent, but not a
BR-dependent mechanism. 2-APB, a non-specific TRPM7 inhibitor was
also able to mimic the growth-inhibitory activity of midazolam,
further supporting the use of TRPM7 as a therapeutic target for
cancer.
Ca2+ is a ubiquitous intracellular signal
responsible for controlling numerous cellular processes and is
particularly important at specific phases of the cell cycle.
Ca2+ and calmodulin (CaM)-dependent signalling is
required for Rb phosphorylation and cell cycle progression from the
G1 to S phase (15).
Ca2+ and CaM/CaM kinase (CaMK) mainly affect the
cell-cycle components by acting directly on the cyclins, CDKs
and/or their small protein inhibitors to regulate the assembly and
activation of CDK complexes and eventually affect Rb
phosphorylation (15,16). Previous studies have demonstrated
that the inhibition of CaMK leads to a decrease in cyclin D1
expression, increase in p27 expression, inhibition of CDK2 and CDK4
and G1 arrest (17,18).
In the present study, midazolam induced an increase in p27
expression, decrease in phosphorylated Rb and cell cycle arrest at
G0/G1 by acting on a Ca2+
transport channel, in accordance with the effects of
Ca2+/CaM/CaMK signaling inhibitors.
Surgical resection of tumors is a necessary
treatment for cancers. However, the perioperative period is the
most likely time for the cancer to disseminate and metastasize.
This is due to the release of cancerous cells during the surgery
and suppression of immune function by stress and anesthesia
(19,20). It has been shown that the
perioperative anesthesia management affects the outcome of patients
undergoing tumor resection (21,22).
It has also been shown that certain anesthetics including ketamine,
thiopental and halothane suppress natural killer cell activity and
promote tumor metastasis (23).
Opiates are known to inhibit the function of the human immune
system (24) and morphine has been
implicated in stimulating human microvascular endothelial cell
proliferation and angiogenesis in vitro and in
vivo(25). However, the direct
effects of anesthetics on the growth and proliferation of cancer
cells have not been elucidated. The present study shows that
midazolam, a commonly-used anesthetic drug, inhibits the growth and
proliferation of human hypopharyngeal squamous cell carcinoma FaDu
cells via the suppression of TRPM7 expression. For solid tumors,
surgical excision is generally considered to be the most effective
approach for removing tumor tissues and alleviating the symptoms
caused by the cell masses. During surgery, anesthesia is essential
for painless and safe procedures. Administering anesthetics with
tumor suppression properties, such as midazolam, may offer an extra
protective benefit during tumor resection.
Similar to midazolam, two other BZ drugs, diazepam
and clonazepam, also exhibited potent anti-proliferative activities
at the same concentration range, indicating the general
anti-proliferative effect of BZs. A number of studies have
previously proposed that PBR is involved in the effect of BZs on
cell proliferation (26,27). However, the present results showing
that the anti-proliferative action of midazolam was not mediated by
PBR in combination with the fact that non-PBR agonist clonazepam
also inhibited cell proliferation, suggest a lack of correlation
between the anti-proliferative activities of these BR ligands and
PBR. Furthermore, in fibrosarcoma, rat C6 glioma and mouse
neuroblastoma, BZs including diazepam and clonazepam inhibit cell
proliferation in a PBR-independent manner (28,29).
In summary, the present results demonstrate that
targeting TRPM7 with the anesthetic midazolam inhibits the
proliferation of human hypopharyngeal squamous cell carcinoma FaDu
cells and this may be counteracted by the TRPM7 agonist bradykinin.
The concentration of BZs at which they act as TRPM7 blockers and
proliferation inhibitors, may be too high for application in cancer
therapy. Future studies are likely to concentrate on exploiting
more TRPM7 inhibitors and developing BZ derivatives with greater
efficacy. Based on the effects of midazolam, bradykinin and 2-APB,
it may be concluded that pharmacological modulation of TRPM7 is a
promising approach for preventing the growth and proliferation of
human head and neck tumor cells.
Acknowledgements
The present study was supported by the
South China Comprehensive Platform for New Medicine R&D
(2009ZX09301-015), Doctoral Fund of the Ministry of Education of
China (No. 20100171110050) and the National Natural Science
Foundation of China for Young Scholars (No. 81202555).
References
|
1
|
Roderick HL and Cook SJ: Ca2+
signalling checkpoints in cancer: remodelling Ca2+ for
cancer cell proliferation and survival. Nat Rev Cancer. 8:361–375.
2008.
|
|
2
|
Monteith GR, McAndrew D, Faddy HM and
Roberts-Thomson SJ: Calcium and cancer: targeting Ca2+
transport. Nat Rev Cancer. 7:519–530. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Capiod T: Cell proliferation, calcium
influx and calcium channels. Biochimie. 93:2075–2079. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bödding M: TRP proteins and cancer. Cell
Signal. 19:617–624. 2007.
|
|
5
|
Jiang J, Li MH, Inoue K, Chu XP, Seeds J
and Xiong ZG: Transient receptor potential melastatin 7-like
current in human head and neck carcinoma cells: role in cell
proliferation. Cancer Res. 67:10929–10938. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhu W, Ou Y, Li Y, et al: A small-molecule
triptolide suppresses angiogenesis and invasion of human anaplastic
thyroid carcinoma cells via down-regulation of the nuclear
factor-kappa B pathway. Mol Pharmacol. 75:812–819. 2009. View Article : Google Scholar
|
|
7
|
Evan GI and Vousden KH: Proliferation,
cell cycle and apoptosis in cancer. Nature. 411:342–348. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ramsey IS, Delling M and Clapham DE: An
introduction to TRP channels. Annu Rev Physiol. 68:619–647. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Carafoli E: Calcium signaling: a tale for
all seasons. Proc Natl Acad Sci USA. 99:1115–1122. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Santoni G and Farfariello V: TRP channels
and cancer: new targets for diagnosis and chemotherapy. Endocr
Metab Immune Disord Drug Targets. 11:54–67. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Prevarskaya N, Zhang L and Barritt G: TRP
channels in cancer. Biochim Biophys Acta. 1772:937–946. 2007.
View Article : Google Scholar
|
|
12
|
Gao H, Chen X, Du X, Guan B, Liu Y and
Zhang H: EGF enhances the migration of cancer cells by
up-regulation of TRPM7. Cell Calcium. 50:559–568. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yee NS, Zhou W and Liang IC: Transient
receptor potential ion channel Trpm7 regulates exocrine pancreatic
epithelial proliferation by Mg2+-sensitive Socs3a
signaling in development and cancer. Dis Model Mech. 4:240–254.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Guilbert A, Gautier M, Dhennin-Duthille I,
Haren N, Sevestre H and Ouadid-Ahidouch H: Evidence that TRPM7 is
required for breast cancer cell proliferation. Am J Physiol Cell
Physiol. 297:C493–C502. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kahl CR and Means AR: Regulation of cell
cycle progression by calcium/calmodulin-dependent pathways. Endocr
Rev. 24:719–736. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Takuwa N, Zhou W, Kumada M and Takuwa Y:
Ca(2+)-dependent stimulation of retinoblastoma gene product
phosphorylation and p34cdc2 kinase activation in serum-stimulated
human fibro-blasts. J Biol Chem. 268:138–145. 1993.
|
|
17
|
Tombes RM, Grant S, Westin EH and Krystal
G: G1 cell cycle arrest and apoptosis are induced in NIH 3T3 cells
by KN-93, an inhibitor of CaMK-II (the multifunctional
Ca2+/CaM kinase). Cell Growth Differ. 6:1063–1070.
1995.PubMed/NCBI
|
|
18
|
Morris TA, DeLorenzo RJ and Tombes RM:
CaMK-II inhibition reduces cyclin D1 levels and enhances the
association of p27kip1 with Cdk2 to cause G1 arrest in NIH 3T3
cells. Exp Cell Res. 240:218–227. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ben-Eliyahu S: The promotion of tumor
metastasis by surgery and stress: immunological basis and
implications for psychoneuroimmunology. Brain Behav Immun. 17(Suppl
1): S27–S36. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ben-Eliyahu S, Page GG, Yirmiya R and
Shakhar G: Evidence that stress and surgical interventions promote
tumor development by suppressing natural killer cell activity. Int
J Cancer. 80:880–888. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Goldfarb Y and Ben-Eliyahu S: Surgery as a
risk factor for breast cancer recurrence and metastasis: mediating
mechanisms and clinical prophylactic approaches. Breast Dis.
26:99–114. 2006.PubMed/NCBI
|
|
22
|
Exadaktylos AK, Buggy DJ, Moriarty DC,
Mascha E and Sessler DI: Can anesthetic technique for primary
breast cancer surgery affect recurrence or metastasis?
Anesthesiology. 105:660–664. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Melamed R, Bar-Yosef S, Shakhar G, Shakhar
K and Ben-Eliyahu S: Suppression of natural killer cell activity
and promotion of tumor metastasis by ketamine, thiopental, and
halothane, but not by propofol: mediating mechanisms and
prophylactic measures. Anesth Analg. 97:1331–1339. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Arain MR and Buggy DJ: Anaesthesia for
cancer patients. Curr Opin Anaesthesiol. 20:247–253. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Gupta K, Kshirsagar S, Chang L, Schwartz
R, Law PY, Yee D and Hebbel RP: Morphine stimulates angiogenesis by
activating proangiogenic and survival-promoting signaling and
promotes breast tumor growth. Cancer Res. 62:4491–4498.
2002.PubMed/NCBI
|
|
26
|
Stepien H, Pawlikowska A and Pawlikowski
M: Effects of benzodiazepines on thymus cell proliferation. Thymus.
12:117–121. 1989.PubMed/NCBI
|
|
27
|
Bruce JH, Ramirez AM, Lin L, Oracion A,
Agarwal RP and Norenberg MD: Peripheral-type benzodiazepines
inhibit proliferation of astrocytes in culture. Brain Res.
564:167–170. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kletsas D, Li W, Han Z and Papadopoulos V:
Peripheral-type benzodiazepine receptor (PBR) and PBR drug ligands
in fibroblast and fibrosarcoma cell proliferation: role of ERK,
c-Jun and ligand-activated PBR-independent pathways. Biochem
Pharmacol. 67:1927–1932. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Gorman AM, O’Beirne GB, Regan CM and
Williams DC: Antiproliferative action of benzodiazepines in
cultured brain cells is not mediated through the peripheral-type
benzodiazepine acceptor. J Neurochem. 53:849–855. 1989. View Article : Google Scholar : PubMed/NCBI
|