Introduction
Multiple myeloma is a B-cell disorder characterized
by accumulation of malignant plasma cells, generally derived from
one clone in the bone marrow (1).
It accounts for ∼1% of all malignant diseases and represents ∼10%
of hematologic malignancies (2).
The intricate interactions between an increase in osteoclastic bone
resorption and a reduction in bone formation usually cause bone
destruction, with the most common localization being the spine. The
condition is associated with severe bone pain, pathological
fractures, osteoporosis and spinal cord compression (3). Spinal cord compression occurs in ∼5%
of patients with multiple myeloma (4). In the present study, a case of
multiple myeloma with a large, lytic bone of the vertebral body and
spinal cord compression is described, which was treated by
laminectomy, pedicle screw fixation and kyphoplasty, known as open
kyphoplasty (OKP). To our knowledge, such methods have rarely been
used to treat a patient with intractable back pain and neurological
compromise resulting from multiple myeloma or spinal
metastases.
Case report
A 72-year-old male was referred with the complaint
of severe back pain and dysfunction of ambulation. The back pain
had begun two months prior to admission and was preceeded by a
history of weakness and significant weight loss. The patient was
unable to walk due to progressive back pain and heaviness of both
lower extremities. Physical examination showed tenderness in the
T9-T10 region, hypertension of both lower extremities without
paraparesis, sensory loss, sphincter disorder or abnormal reflexes.
The study was approved by the Ethics Committee of The First
Affiliated Hospital of Soochow University, Suzhou, China. Written
informed consent was obtained from the patient.
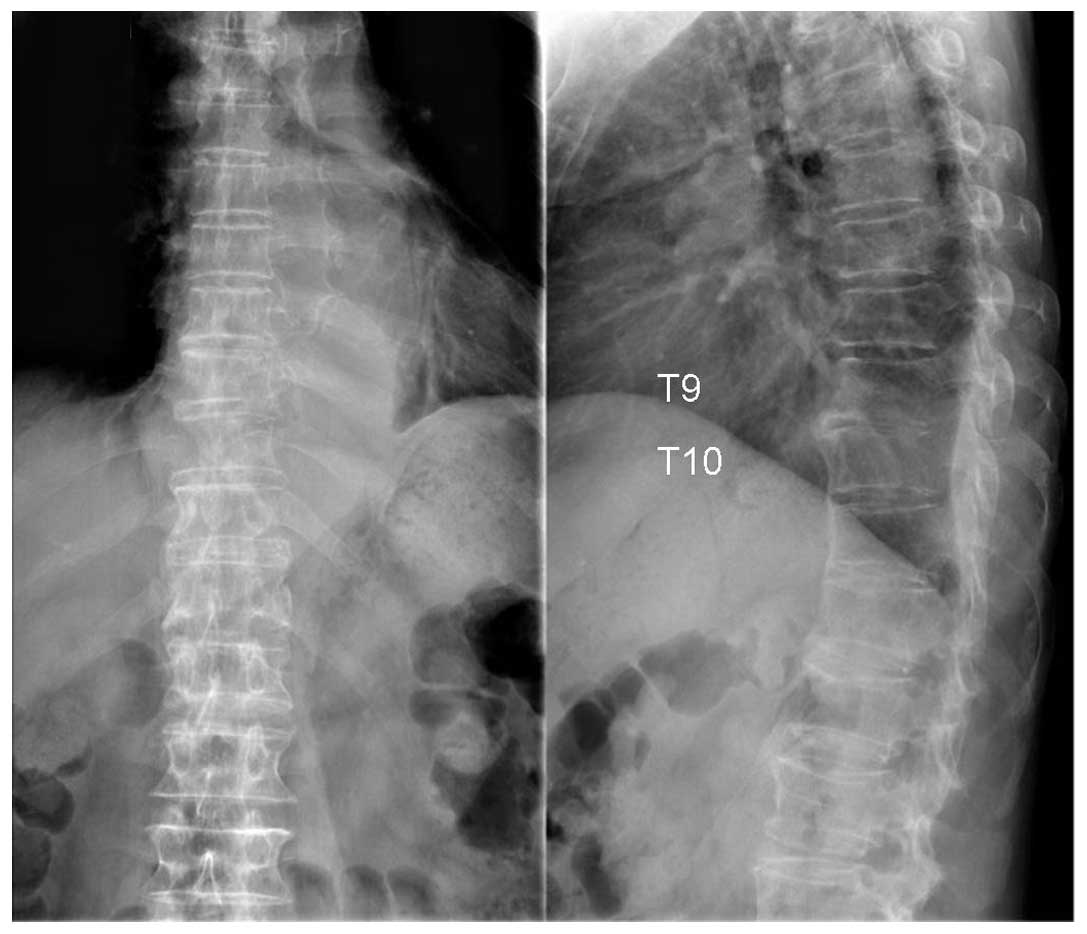
X-ray, computed tomography (CT) and magnetic
resonance imaging (MRI) of the thoracic spine revealed spinal cord
compression at the T9-T10 level due to an extensive epidural mass
in the spinal canal (Figs.
1–3). There was also a large
lytic mass at the T7-T12 level with the extraosseous extension
surrounding the abdominal aorta, and lytic involvement of T9 and
T10. Initial laboratory studies revealed a Bence-Jones proteinuria
and an erythrocyte sedimentation rate of 100 mm/h. Bone marrow
aspiration of the posterior iliac crest showed an infiltration of
atypical plasma cells.
Surgery was performed under general anesthesia, with
the patient placed in the extended prone position, with padding
beneath the upper chest and pelvic regions. The first operative
phase involved osteosynthesis where 8 pedicle screws were placed at
T7, T8, T11 and T12. Laminectomy of T9 and T10 was performed to
achieve decompression of the spinal cord. This was followed by
biopsy. The second phase of surgery involved kyphoplasty. An
11-gauge Jamshidi needle was placed into the posterior part of T9
via the left transpedicular approach as the right pedicle was
totally eroded. The kyphoplasty systems (Kyphon, Sunnyvale, CA,
USA) were placed into the T9 vertebral body through the left
working channel. The balloon was inflated to 2 ml under
fluoroscopic guidance until manometric parameters reached 150 Pa.
Polymethyl methacrylate (PMMA) cement (2.5 ml) was placed into the
cavity under continuous fluoroscopic monitoring in the lateral
plane following the withdrawal of the balloon. The same procedure
was performed in T10. The whole duration of the surgical
intervention was 3.5 h and 400 ml red blood cells was
transfused.
The patient tolerated surgery and showed a good
clinical outcome. The day after the procedure, the patient had
excellent alleviation of back pain without painkillers and the
visual analogue scale (VAS) score was decreased from 8 to 2 points.
Three days after surgery, the patient could ambulate with
assistance. Two weeks after the operation, the patient was
transferred to the Hematological Department for further
chemotherapy and radiotherapy. The postoperative radiographs showed
no cement leakage or mislocation of screws (Fig. 4). Histopathological examination of
the tumor tissue confirmed multiple myeloma consistent with bone
marrow aspiration.
Discussion
Multiple myeloma is a fatal hematological malignancy
associated with clonal expansion of malignant plasma cells within
the bone marrow and the development of a destructive osteolytic
bone disease (3). The median age at
diagnosis is 68 years old and males are more frequently affected
than females. Although chemotherapy and radiotherapy as noninvasive
treatment have a major role in the management of multiple myeloma,
they may have adverse effects on a patient’s immune system
(5). Furthermore, neither of these
treatment approaches protect the spine from progressive osteolytic
collapse and spinal cord compression, which cause intractable pain,
neurological compromise and overt or impending spinal instability.
An effective alternative therapy is therefore required.
Posterior decompression and pedicle screw
instrumentation supplemented with kyphoplasty, known as OKP, is
recognized as an appropriate surgery to achieve pain relief,
neurological improvement and spinal stability. OKP is not a new
method. It was first reported by Hsiang (6) in 2003 to treat an osteoporotic
vertebral compression fracture with fractured posterior cortex.
Fuentes et al(7) recently
reported the use of OKP in a series of 16 patients with severe
osteoporotic compression fractures associated with neurological
disorders, all of whom gained significant pain reduction and
neurological improvement. Furthermore, Marco et al(8) used OKP with calcium phosphate instead
of PMMA to treat 38 relatively young and healthy patients suffering
from unstable thoracolumbar burst fractures with or without
neurological deficit. They demonstrated that this method
reconstructed and stabilized the anterior column, restored
vertebral body height, indirectly and directly decompressed the
thecal sac, reduced the kyphotic deformity and stabilized the
posterior column, using a posterior approach. Open vertebroplasty
(OVP) was recently described by Weitao et al(9), who reported that this method was used
to treat 18 cases with spinal metastatic disease. Excellent pain
relief and neural function recovery were obtained, apart from in 1
case where cement leakage into the pulmonary veins occurred due to
the use of low viscosity cement and a high application pressure. To
our knowledge, no study has evaluated the clinical outcome for
patients with multiple myeloma with neurological deficits who have
been managed with OKP.
With the development of minimally invasive surgery,
vertebral augmentation has widely been used for intractable painful
pathological vertebral fracture caused by multiple myeloma. Yang
et al(10) reported that
vertebroplasty combined with chemotherapy in the treatment of
multiple myeloma-associated spinal fracture showed significant
improvement of pain relief. Kyphoplasty as a modified version of
vertebroplasty involved inflation of a balloon within a collapsed
vertebral body to allow a void injection of PMMA. A report from Zou
et al(11) involved 21
myeloma patients with vertebral compressive fractures who underwent
43 kyphoplasty procedures which provided a significant and
sustained reduction of pain, resulting in a significant functional
improvement for the multiple myeloma patients. Several analgesic
and antitumor mechanisms of PMMA were proposed, including
stabilization of vertebral microfracture and enhancement of bone
support force, both monomer cytotoxicity and thermal effect on
tumor cell and pain nerve endings, and blood supply cut off by
solidification of cement (12,13).
In the present study, we described a case of back pain of VAS 8
points which was reduced to 2 points immediately after surgery. The
effect has lasted to the latest follow-up without additional
painkillers.
Both vertebroplasty and kyphoplasty have been shown
to substantially reduce pain from vertebral collapse caused by
myeloma but have the same complication of cement leakage into the
spinal canal, neural foramina or pulmonary venous system. Moreover,
the incidence of cement extravasation with kyphoplasty or
vertebroplasty for myeloma is much higher than that associated with
osteoporotic fractures due to cortical destruction and the enriched
blood supply of myeloma (9). Lee
et al used a meta-analysis and reported that the rate of
symptomatic cement leakage was 10% in metastatic disease or myeloma
and only 1% in osteoporotic collapse (14). Furthermore, the rate in
vertebroplasty is much higher than that in kyphoplasty. The largest
North American series reporting augmentation of cement for
metastatic spinal disease showed that leakage of cement occurred
during vertebroplasty at six of 65 levels (9.2%) while no
extravasation (0/32) was seen during kyphoplasty (15).
The large eroded vertebral posterior wall of T9 and
T10 implied high risks of cement leakage and secondary neurological
deterioration in the present case, which presented the greatest
challenge of the procedure. Spinal canal compromise and disruption
of the posterior cortex of the vertebral body have been considered
as relative contraindications. In our study, to minimize the
disruption of the posterior wall, continuous fluoroscopic
monitoring was performed throughout the bone cement-filling
process. The filling process was stopped as soon as the bone cement
reached one-fourth of the distance to the posterior wall of the
vertebrae (16). Unipedicular
kyphoplasty was performed as the right side of vertebral pedicle
and posterior wall were totally eroded. It was observed by La Maida
et al(17) that unipedicular
kyphoplasty demonstrate results comparable with those of
bipedicular kyphoplasty in the treatment of multiple myeloma. In
this case, no cement leakage into the spinal canal, neural foramina
or venous system was found at X-ray, either postoperatively or by
fluoroscopic monitoring during surgery (Fig. 4).
Vertebral augmentation has limitations in relieving
spinal cord compression and stabilizing the spinal column, however.
A surgical approach including laminectomy and pedicle screw
fixation is therefore necessary. It was recognized that surgical
decompression when performed without instrumentation, whether via a
ventral or dorsal approach, caused further instability to the
metastatic spine (18). In this
case, decompression and osteosynthesis were performed ahead of
kyphoplasty for several reasons. Firstly, the rate of spinal cord
injury caused by the mechanically inflated balloon during
kyphoplasty could be decreased significantly when the canal was
decompressed. Secondly, laminectomy and decompression allowed
direct visualization of the posterior vertebral wall for safe
cement-filling and removal of cement leakage as soon as it was
observed under fluoroscopic monitoring (15). In addition, the use of PMMA cement
augmentation helped secure the pedicle screws when pathological
fractures or kyphosis developed due to operative instability such
as loss of posterior spinal elements (19,20).
OKP is a reasonable palliative surgery to treat
multiple myeloma or spinal metastatic disease accompanied by spinal
cord compression. It allows simultaneous decompression of the
spinal cord and stabilization of the vertebral column in the same
procedure and demonstrates excellent clinical results in pain
relief and the recovery of neural function with less blood loss,
shorter operation time and fewer complications.
References
|
1
|
Sirohi B and Powles R: Multiple myeloma.
Lancet. 363:875–887. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Angtuaco EJ, Fassas AB, Walker R, Sethi R
and Barlogie B: Multiple myeloma: clinical review and diagnostic
imaging. Radiology. 231:11–23. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Edwards CM, Zhuang J and Mundy GR: The
pathogenesis of the bone disease of multiple myeloma. Bone.
42:1007–1013. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dispenzieri A and Kyle RA: Neurological
aspects of multiple myeloma and related disorders. Best Pract Res
Clin Haematol. 18:673–688. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zou J, Mei X, Gan M, Wang G and Yang H: Is
kyphoplasty reliable for osteoporotic vertebral compression
fracture with vertebral wall deficiency? Injury. 41:360–364. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hsiang J: An unconventional indication for
open kyphoplasty. Spine J. 3:520–523. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fuentes S, Blondel B, Metellus P, et al:
Open kyphoplasty for management of severe osteoporotic spinal
fractures. Neurosurgery. 64:350–354. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Marco RA and Kushwaha VP: Thoracolumbar
burst fractures treated with posterior decompression and pedicle
screw instrumentation supplemented with balloon-assisted
vertebroplasty and calcium phosphate reconstruction. J Bone Joint
Surg. 91:20–28. 2009. View Article : Google Scholar
|
|
9
|
Weitao Y, Qiqing C, Songtao G, et al: Open
vertebroplasty in the treatment of spinal metastatic disease.
Clinical Neurology and Neurosurgery. 114:307–312. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yang Z, Tan J, Xu Y, et al: Treatment of
MM-associated spinal fracture with percutaneous vertebroplasty
(PVP) and chemotherapy. Eur Spine J. 21:912–919. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zou J, Mei X, Gan M and Yang H:
Kyphoplasty for spinal fractures from multiple myeloma. J Surg
Oncol. 102:43–47. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gangi A and Buy X: Percutaneous bone tumor
management. Semin Intervent Radiology. 27:124–136. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Urrutia J, Bono CM, Mery P and Rojas C:
Early histologic changes following polymethylmethacrylate injection
(vertebroplasty) in rabbit lumbar vertebrae. Spine. 33:877–882.
2008. View Article : Google Scholar
|
|
14
|
Lee MJ, Dumonski M, Cahill P, et al:
Percutaneous treatment of vertebral compression fractures: a
meta-analysis of complications. Spine. 24:1228–1232.
2009.PubMed/NCBI
|
|
15
|
Fourney DR, Schomer DF, Nader R, et al:
Percutaneous vertebroplasty and kyphoplasty for painful vertebral
body fractures in cancer patients. J Neurosurg. 98:21–30.
2003.PubMed/NCBI
|
|
16
|
Qian Z, Sun Z, Yang H, et al: Kyphoplasty
for the treatment of malignant vertebral compression fractures
caused by metastases. J Clin Neurosci. 18:763–767. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
La Maida GA, Sala F, Callea G, et al:
Efficacy of unipedicular baloon kyphoplasty for treatment of
multiple myeloma vertebral lesions. Asian Spine J. 5:162–168.
2011.PubMed/NCBI
|
|
18
|
Steinmetz MP, Mekhail A and Benzel EC:
Management of meta-static tumors of the spine: strategies and
operative indications. Neurosurg Focus. 11:e22001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
McGirt MJ, Garcés-Ambrossi GL, Parker SL,
et al: Short-term progressive spinal deformity following
laminoplasty versus laminectomy for resection of intradural spinal
tumors: analysis of 238 patients. Neurosurgery. 66:1005–1012. 2010.
View Article : Google Scholar
|
|
20
|
Frankel BM, Jones T and Wang C: Segmental
polymethylmethacrylate-augmented pedicle screw fixation in patients
with bone softening caused by osteoporosis and metastatic tumor
involvement: a clinical evaluation. Neurosurgery. 61:531–538. 2007.
View Article : Google Scholar
|