Introduction
Sarcomatoid carcinoma is a rare, aggressive
malignancy containing mesenchymal and epithelial components.
Sarcomatoid hepatocellular carcinoma (SHC) is an uncommon malignant
lesion of the liver, with an incidence of 2% in surgically-resected
cases and 4–9% in autopsied cases (1–4).
Forming a diagnosis may be difficult due to its atypical
presentation. Concomitant gallbladder carcinoma with primary SHC is
a rare type of hepatobiliary disease that contains two different
malignant lesions. To the best of our knowledge, such a case has
not previously been reported. The present study reports a case of
gallbladder carcinoma accompanied with SHC in a Chinese male. The
management of this rare disease is also discussed. Written informed
consent was obtained from the patient’s family for publication of
the case report and accompanying images.
Case report
An 80-year-old male, who had been a hepatitis B
virus (HBV) carrier for 10 years, was admitted to Qilu Hospital,
Shandong University, Ji’nan, Shandong, China due to right-sided
epigastric pain and a low fever occurring over the preceding 2
months. Additionally, there was no apparent loss in body weight and
the routine blood tests were normal. The levels of tumor markers,
including that of α-fetoprotein (AFP), carbohydrate antigen (CA)
19-9, CA 125, carcinoembryonic antigen (CEA) and CA 50, were all
within the normal ranges. The liver function grade of the patient
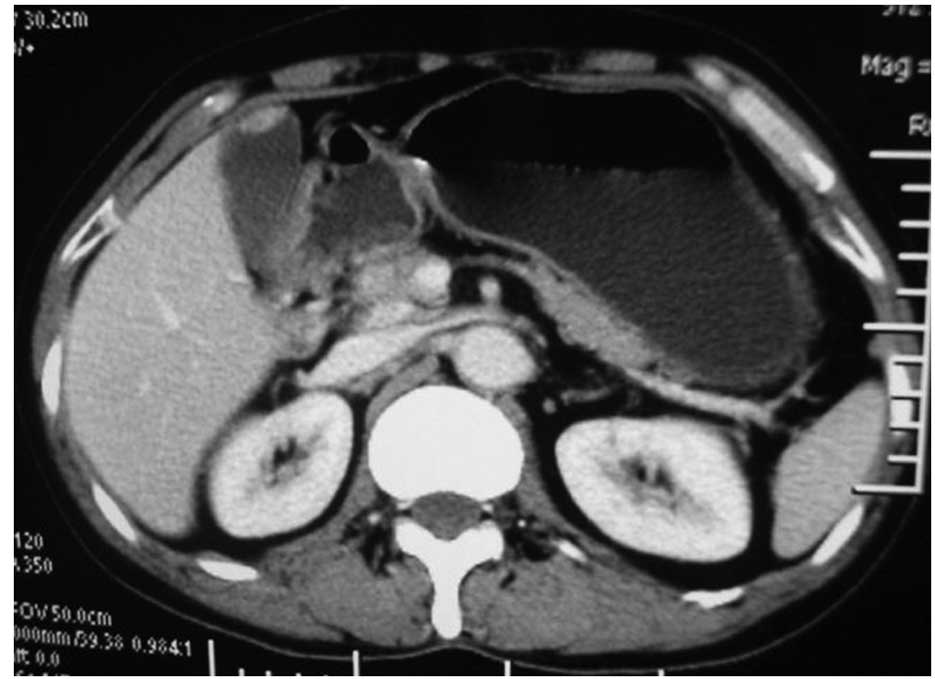
was Child-Pugh grade A. Contrast-enhanced computed tomography (CT)
of the abdomen revealed a hypodense lesion consisting of a 5×4×3 cm
mass in the right lobe of the liver (Fig. 1). Abdominal CT showed a regular
intraluminal polypoid mass in the gallbladder with no demonstrable
lymph nodes (LNs) in the pericholecystic or upper abdominal regions
(Fig. 2). No evidence of
intra-abdominal metastatic spread was observed. The first
presumptive diagnosis was of hepatocellular carcinoma (HCC) and
gallbladder adenoma, and the second was of gallbladder carcinoma
with liver metastasis. Following a partial hepatectomy of the right
lobe of the liver and a cholecystectomy, the patient was diagnosed
with SHC combined with adenocarcinoma of the gallbladder in
situ by pathological examination. On gross examination, the
mass of the liver measured 5×3.5×3 cm. A papillary tumor of 12×10×7
mm was identified in the middle third of the gallbladder, with a
basal portion of 7 mm. The surface cut appeared brown in the
peripheral portion with a hemorrhage foci and massive necrosis in
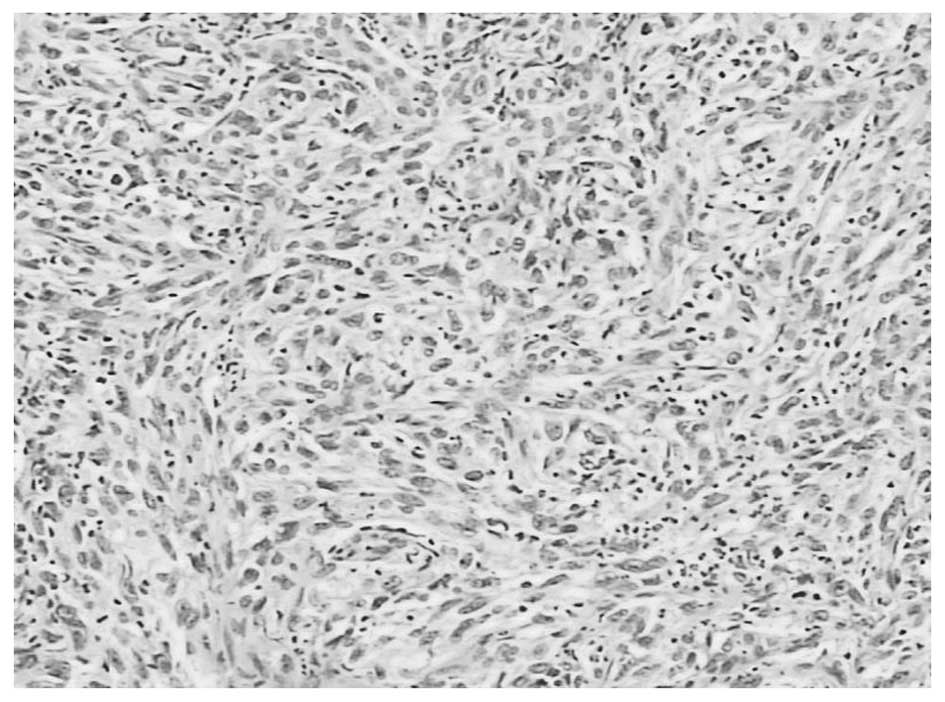
the center. On pathological examination, the tumor of the liver was
composed of spindle-shaped tumor cells, resembling true sarcomas
(Fig. 3). Histologically, the mass
in the gallbladder was found to be a high-grade adenocarcinoma. The
cancer stage of the patient was classified as type T1N0M0 using the
classification of the American Joint Committee on Cancer (AJCC)
(5). Immunohistochemically, the
neoplastic cells were strongly positive for CK, CK2, CK7 and
vimentin, showing evidence of their epithelial malignancy rather
than a combination of HCC and sarcoma. Diagnosis of this condition
may prove difficult as the histological features may mimic sarcoma.
In view of the clinical history and the morphological and
immunohistochemical observations, a diagnosis of primary SHC was
made.
The patient recovered from the surgery with no
complications, however, post-operative adjuvant chemotherapy and
radiation therapy were refused. The patient developed progressive
intrahepatic and lung metastases and finally succumbed to this six
months post-surgery.
Discussion
Patients with SHC often present with a poor
prognosis due to skin, pleural and pelvic skeletal metastases
(6–8). The incidence of SHC is highest in the
fifth and sixth decades of life. The majority of cases are
symptomatic with pain in the right upper quadrant of the abdomen.
Transarterial chemotherapy, chemoembolization or radiofrequency
ablation are presumed to promote sarcomatous changes in HCC
(9).
The terminology and pathogenesis of SHC remain
controversial issues. In the present study, the sarcomatous
elements in the neoplasms were stained positive for the epithelial
markers, as confirmed by immunohistochemical studies, which
supported the pathological diagnosis of sarcomatoid carcinoma
rather than carcinosarcoma. The pathogenesis of SHC has not yet
been clarified due to the ongoing debate on whether SHC is derived
from the transition of an ordinary HCC to a sarcomatous HCC, or if
it is a double cancer of HCC and hepatic sarcoma. One possible
origin of sarcomatoid carcinoma is the collision theory of
independent neoplasm growths from multipotent stem cells,
epithelial to mesenchymal transition, and the other possible origin
is the combination of the two tumors (2,3,10). The
majority of investigators consider that the sarcomatous component
is derived from a dedifferentiation of anaplasia from an ordinary
HCC. It is difficult to gauge if there is a connection between SHC
and HBV, however, 54% of patients are HBV carriers (11).
The treatment of choice for SHC is surgical
resection. The utility of other treatments, including chemotherapy,
radiotherapy and immunotherapy, remains unproven. The formation of
a clinical diagnosis is difficult and relies on a combination of
imaging techniques, including ultrasound, CT scans and even
pathological techniques, such as fine-needle aspirations with
biopsies of the suspicious mass. The expression of cytokeratin by
the spindle cell component of the sarcomatoid carcinoma, as
observed by immunohistochemistry, suggests a common origin rather
than a collision tumor composed of sarcoma and carcinoma (2,3). There
were no transitional zones between the carcinomatous and
sarcomatous components in the present study, which did not support
the transformation theory. Furthermore, the sarcomatous elements
were stained positive for the epithelial markers that had been
applied for immunohistochemical staining, which supported the
pathological diagnosis of sarcomatoid carcinoma rather than
carcinosarcoma.
SHC usually presents as a large mass with peripheral
enhancement, central necrosis, variable enhancement of the solid
portion with or without a tumor capsule, and intrahepatic
metastasis (11). When gallbladder
carcinoma is accompanied by minor SHC, it is not difficult to deal
with the malignancy and early gallbladder lesions at the same time,
as the preservation of enough liver parenchyma is easy to achieve,
resulting in a successful surgery. Adjuvant chemotherapy and/or
radiation therapy may be necessary for the patient following the
resection. Intrahepatic metastasis and adjacent organ invasion are
relatively more common with SHC than with ordinary HCC (10).
In conclusion, SHC is a relatively rare, malignant
hepatic neoplasm. Although it is not easy to speculate on the
coexistence of gallbladder adenocarcinoma and SHC, pre- and
post-operative diagnoses may be essential. Surgical involvement is
the mainstay of therapy. Further studies are essential to expound
the possible associations involved. The prognosis of patients with
multiple primary carcinomas is extremely poor.
References
|
1
|
Kakizoe S, Kojiro M and Nakashima T:
Hepatocellular carcinoma with sarcomatous change. Clinicopathologic
and immunohistochemical studies of 14 autopsy cases. Cancer.
59:310–316. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kojiro M, Sugihara S, Kakizoe S, Nakashima
O and Kiyomatsu K: Hepatocellular carcinoma with sarcomatous
change: a special reference to the relationship with anticancer
therapy. Cancer Chemother Pharmacol. 23(Suppl): S4–S8. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Maeda T, Adachi E, Kajiyama K, Takenaka K,
Sugimachi K and Tsuneyoshi M: Spindle cell hepatocellular
carcinoma. A clinicopathologic and immunohistochemical analysis of
15 cases. Cancer. 77:51–57. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
He J, Zeng ZC, Tang ZY, et al: Clinical
features and prognostic factors in patients with bone metastases
from hepatocellular carcinoma receiving external beam radiotherapy.
Cancer. 115:2710–2720. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hamilton S and Aaltonen L: WHO
Classification of Tumours of the Digestive System. IARC Press;
Lyon: pp. 105–119. 2000
|
|
6
|
Inoue T, Kudo M, Minami Y, Chung H,
Fukunaga T and Kawasaki T: Case of rapidly progressed sarcomatoid
hepatocellular carcinoma in a young female without risk factor.
Liver Int. 27:1428–1430. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nishie W, Iitoyo M, Koshiyama T and Kusama
T: Sarcomatoid carcinoma of the liver with skin and pleural
metastases. Br J Dermatol. 148:1069–1071. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chen CY, Hsueh YT, Lan TY, Lin WH, Wu K
and Yang RS: Pelvic skeletal metastasis of hepatocellular carcinoma
with sarcomatous change: a case report. Diagn Pathol. 5:332010.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Koda M, Maeda Y, Matsunaga Y, Mimura K,
Murawaki Y and Horie Y: Hepatocellular carcinoma with sarcomatous
change arising after radiofrequency ablation for
well-differentiated hepatocellular carcinoma. Hepatol Res.
27:163–167. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Honda H, Hayashi T, Yoshida K, et al:
Hepatocellular carcinoma with sarcomatous change: characteristic
findings of two-phased incremental CT. Abdom Imaging. 21:37–40.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Koo HR, Park MS, Kim MJ, et al:
Radiological and clinical features of sarcomatoid hepatocellular
carcinoma in 11 cases. J Comput Assist Tomogr. 32:745–749. 2008.
View Article : Google Scholar : PubMed/NCBI
|