Introduction
Inflammatory pseudotumors (IPTs) arise most commonly
from the lungs (1). Histologically,
IPTs are characterized by proliferating fibrovascular tissue with
an infiltration of inflammatory cells, including plasma cells,
lymphocytes and eosinophils (2).
IPTs of the liver are rare and are often mistaken as malignant
tumors. Computed tomography (CT) scans and magnetic resonance
imaging (MRI) are of certain value when forming a differential
diagnosis. However, in specific cases, particularly those with
hepatitis B virus (HBV)-related cirrhosis, it is extremely
difficult to establish a definite diagnosis by radiological
imaging. For these cases, a correct differential diagnosis of IPT
from the malignant tumor is of great importance to prevent the
delay of necessary treatment (3).
The current study presents the case of liver IPT
with HBV-related cirrhosis, which was misdiagnosed as a primary
hepatic malignant tumor. The final diagnosis of IPT was made by a
post-operative pathological examination. Written informd consent
was obtained from the patient.
Case report
Clinical presentation
A 58-year-old male was referred to the First
Affiliated Hospital (Hangzhou, China) following detection of a
lesion in the right lobe of the liver by ultrasonography of the
abdomen. Upon admission, the patient was free from symptoms and in
good general health, without jaundice. The liver and spleen were
not palpated, since the patient had no hepatomegaly and only had
mild splenomegaly, and there was no sign of any abdominal mass. In
addition, the patient had a 10-year history of HBV infection.
Pathological analysis
Laboratory investigations revealed normal liver
function test results. The hepatitis serology for HBsAg was
positive and no hepatitis C infection was identified. In addition,
no leukocytosis was observed and normal AFP, CA19-9 and CEA levels
were detected. The upper GI endoscopy and colonoscopy results were
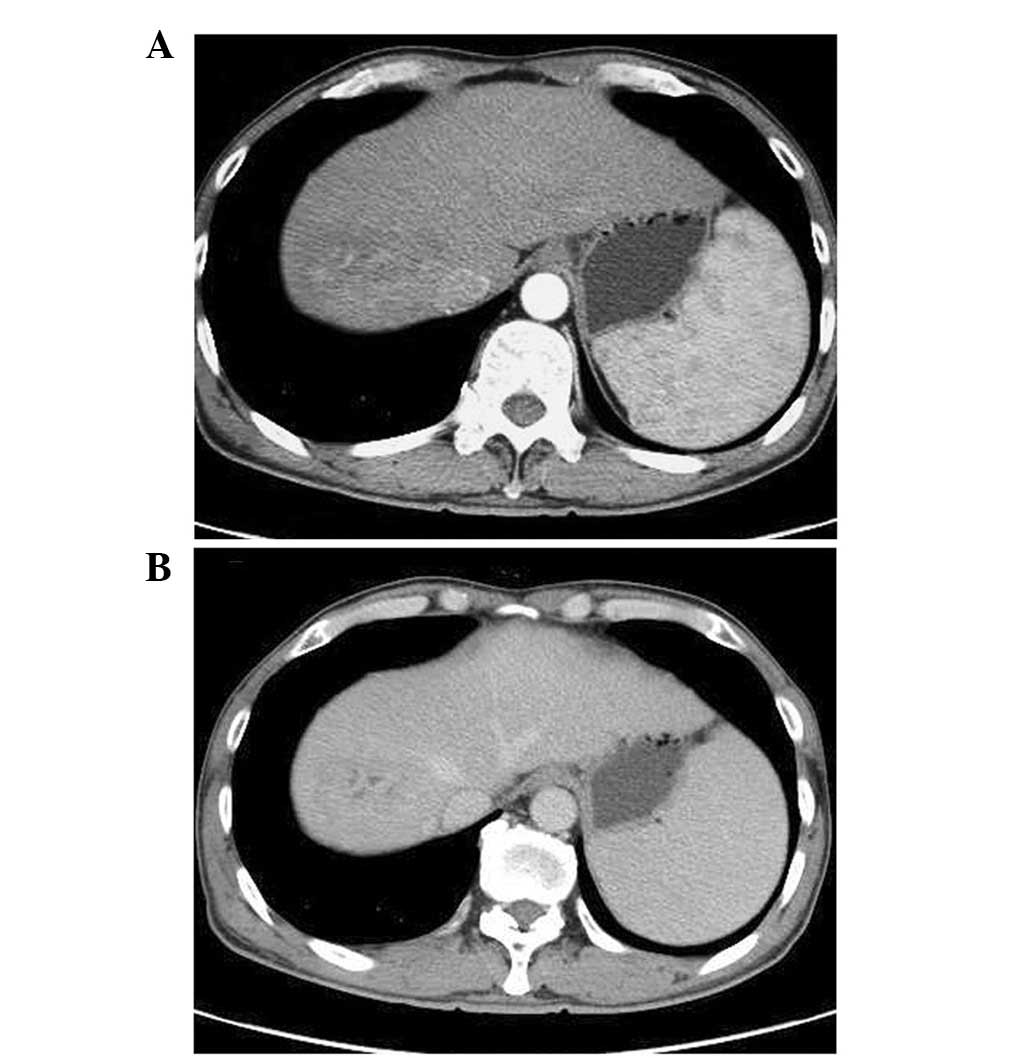
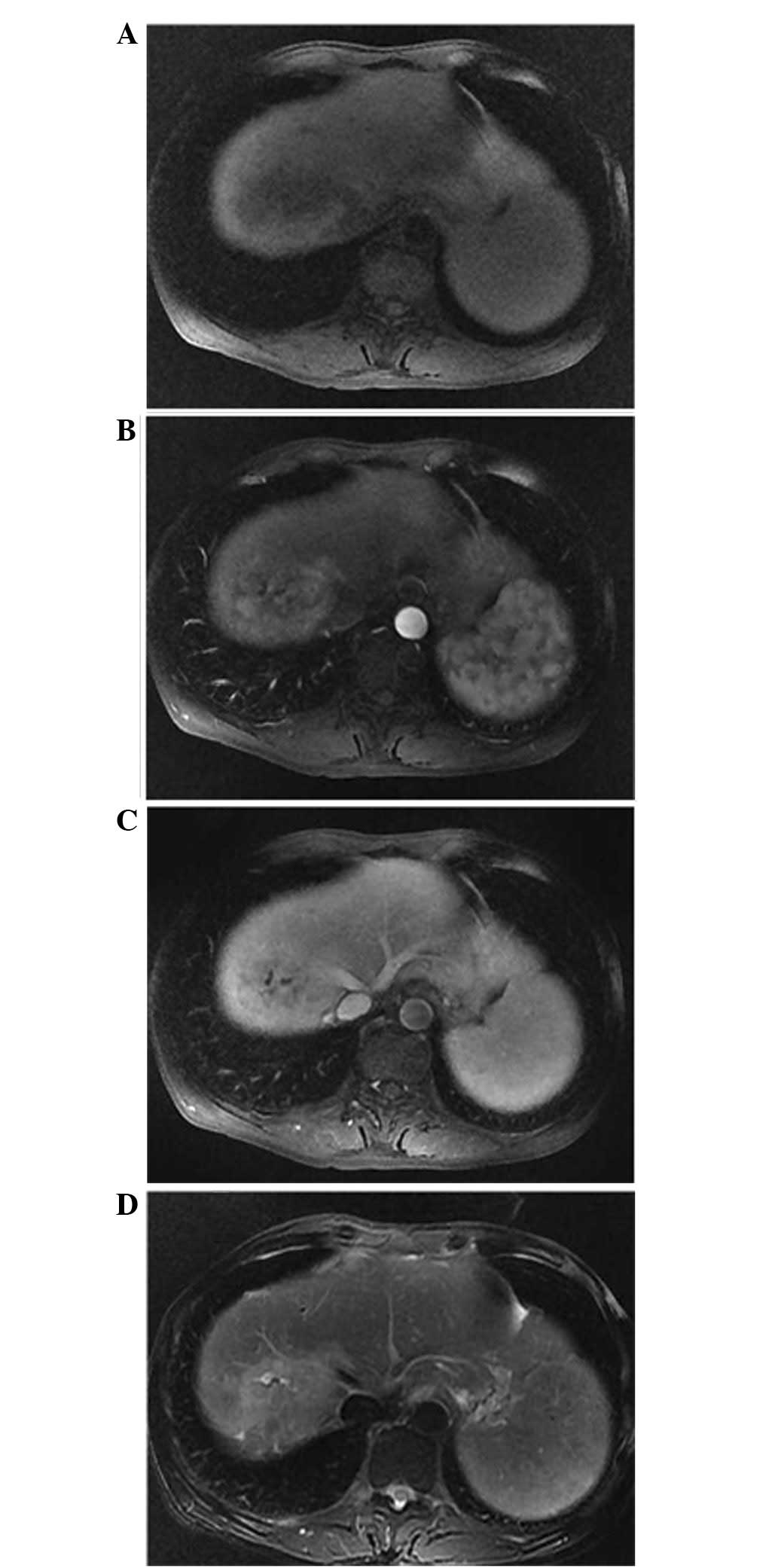
normal. The abdominal CT (Fig. 1)
and MRI (Fig. 2) examinations
revealed a well-defined heterogeneous mass situated in Couinaud
segment 8 and measuring 3.8×5.0 cm. The lesion featured a mild
enrichment from the arterial phase in the CT and MRI, consistent
with a malignancy. The initial diagnosis was of a primary hepatic
malignant tumor. During surgery, mild liver cirrhosis was
identified. The tumor was located in Couinaud segment 8 and had
clear boundaries. A local resection was performed and the
intra-operative blood loss was measured at 300 ml. The patient
recovered well following the surgery and was consequently
discharged on the ninth post-operative day.
Histological analysis
Macroscopically, the cut surface of the resected
specimen was that of a yellowish-white tumor, which was 4.0 cm in
diameter. A microscopic examination revealed a process with benign
characteristics, which included numerous infiltrating lymphocytes,
mainly plasma cells (Fig. 3). These
histological observations confirmed the final diagnosis of a
hepatic IPT.
Discussion
Liver IPT was first described in 1953 by Pack and
Baker (2). To date, the etiology
and pathogenesis of IPTs remain unknown. Liver IPTs are associated
with a number of diseases, including Crohn’s disease, diabetes
mellitus, Sjögren’s syndrome, gout, chronic cholangitis, primary
sclerosing cholangitis, Kostmann’s disease and autoimmune
pancreatitis (3). The majority of
patients usually present with a fever and abdominal pain (3), and a small number of patients suffer
from jaundice caused by idiopathic inflammatory structures of the
extrahepatic biliary tree. Clinical manifestations and imaging are
similar to those of a tumor with the exception of the benign
biological behavior and the properties of spontaneous regression
following treatment with antibiotics (4) or non-steroidal anti-inflammatory drugs
(5). CT scans and MRI are the main
methods to establish the diagnosis. A CT scan usually reveals
lesions with variable contrast enhancement. IPTs may present with a
hypovascular character in the CT scan and manifest as a low signal
intensity (hypointense) on T1-weighted images with moderate to high
signal intensities (hyperintense) on T2 sequences in MRI. The
imaging appearance of an IPT is diverse and depends on the
proportion and distribution of inflammatory cells and fibrosis
within the lesion (5). Generally,
tumor markers are not useful, as the levels of the majority of
markers fall within the normal range. In specific cases, a
diagnosis is extremely difficult to make.
For cases of suspected IPT, the importance of
percutaneous needle biopsy has been emphasized, and due to the risk
of spontaneous regression, unnecessary surgery must be avoided
(6). In the current case, a
percutaneous needle biopsy was not performed. The imaging
appearance of the IPT indicated a malignant character, consistent
with the patient history of HBV-related cirrhosis. The lesion was
located on the surface of the Couinaud segment. As we were
concerned over the relatively high rate of hemorrhaging following a
possible percutaneous needle biopsy, as well as the risk of needle
tract seeding, a surgical resection without needle biopsy was
performed. Needle tract seeding has been reported to occur in 5.1%
of patients with hepatocellular carcinoma who have undergone
percutaneous needle biopsy (7).
Although the case was ultimately proved to be that of an IPT by a
post-operative pathological examination, in our opinion, a needle
biopsy should not be utilized as a routine diagnostic tool if a
lesion is strongly suspected to be of malignant character. Active
surgical resection must be the first choice. While hepatectomy is
dangerous in patients with poor health, a liver biopsy must be
considered in these cases to avoid unnecessary surgical
procedures.
In general, IPTs are considered to represent benign
lesions, however, the correct treatment protocol for these
pseudotumors remains controversial. Certain studies have reported
that lesions are likely to be completely resolved following
treatment with antibiotics. However, specific lesions have recurred
following this treatment protocol. By contrast, IPTs have never
been reported to recur following surgical resection. We recommend
that short-term observation should be performed in patients
diagnosed with IPT. In addition, for cases where the lesion is
difficult to differentiate from the malignancy or is associated
with high risk factors, including HBV-related cirrhosis, surgical
resection must be considered.
References
|
1.
|
Bahadori M and Liebow AA: Plasma cell
granulomas of the lung. Cancer. 31:191–208. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Pack GT and Baker HW: Total right hepatic
lobectomy: report of a case. Ann Surg. 138:253–258. 1953.
View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Faraj W, Ajouz H, Mukherji D, Kealy G,
Shamseddine A and Khalife M: Inflammatory pseudo-tumor of the
liver: a rare pathological entity. World J Surg Oncol. 23:52011.
View Article : Google Scholar
|
|
4.
|
Lupovitch A, Chen R and Mishra S:
Inflammatory pseudotumour of the liver. Report of the fine needle
aspiration cytologic findings in a case initially misdiagnosed as
malignant. Acta Cytol. 33:259–262. 1989.PubMed/NCBI
|
|
5.
|
Vassiliadis T, Vougiouklis N, Patsiaoura
K, et al: Inflammatory pseudotumor of the liver successfully
treated with nonsteroidal anti-inflammatory drugs: a challenge
diagnosis for one not so rare entity. Eur J Gastroenterol Hepatol.
19:1016–1020. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Koide H, Sato K, Fukusato T, et al:
Spontaneous regression of hepatic inflammatory pseudotumor with
primary biliary cirrhosis: case report and literature review. World
J Gastroenterol. 12:1645–1648. 2006.PubMed/NCBI
|
|
7.
|
Takamori R, Wong LL, Dang C and Wong L:
Needle-tract implantation from hepatocellular cancer: is needle
biopsy of the liver always necessary? Liver Transpl. 6:67–72.
2000.PubMed/NCBI
|