Introduction
Primary sarcoma of the aorta is extremely rare and
accounts for <1% of all sarcomas (1). A prompt diagnosis prior to organ
ischemia and systemic metastasis is difficult due to the various
clinical presentations of this disease. Despite the availability of
various imaging studies, including computed tomography (CT) and
magnetic resonance (MR) imaging, the condition may be mistaken for
an aortic aneurysm or other arterial occlusive diseases (2,3).
Treating a primary sarcoma of the aorta is also difficult since
this disease is usually diagnosed at a relatively late stage. The
present study describes a case of primary sarcoma in the infrarenal
aorta and its palliative treatment. Written informed consent was
obtained from the patient’s family.
Case report
A 50-year-old male was initially admitted to a
community hospital due to claudication, and was consequently
diagnosed with arteriosclerosis obliterans. The vasodilator,
cilostazol, was administered to the patient for ~1 month. However,
the ischemia of the lower limbs worsened with significant pain on
resting, as well as abdominal pain. Therefore, the patient was
transferred to Xijing Hospital (Xi’an, Shaanxi, China). A physical
examination revealed a pulsatile mass in the abdomen. The lower
limbs were cold and the femoral, popliteal and dorsalis pedis
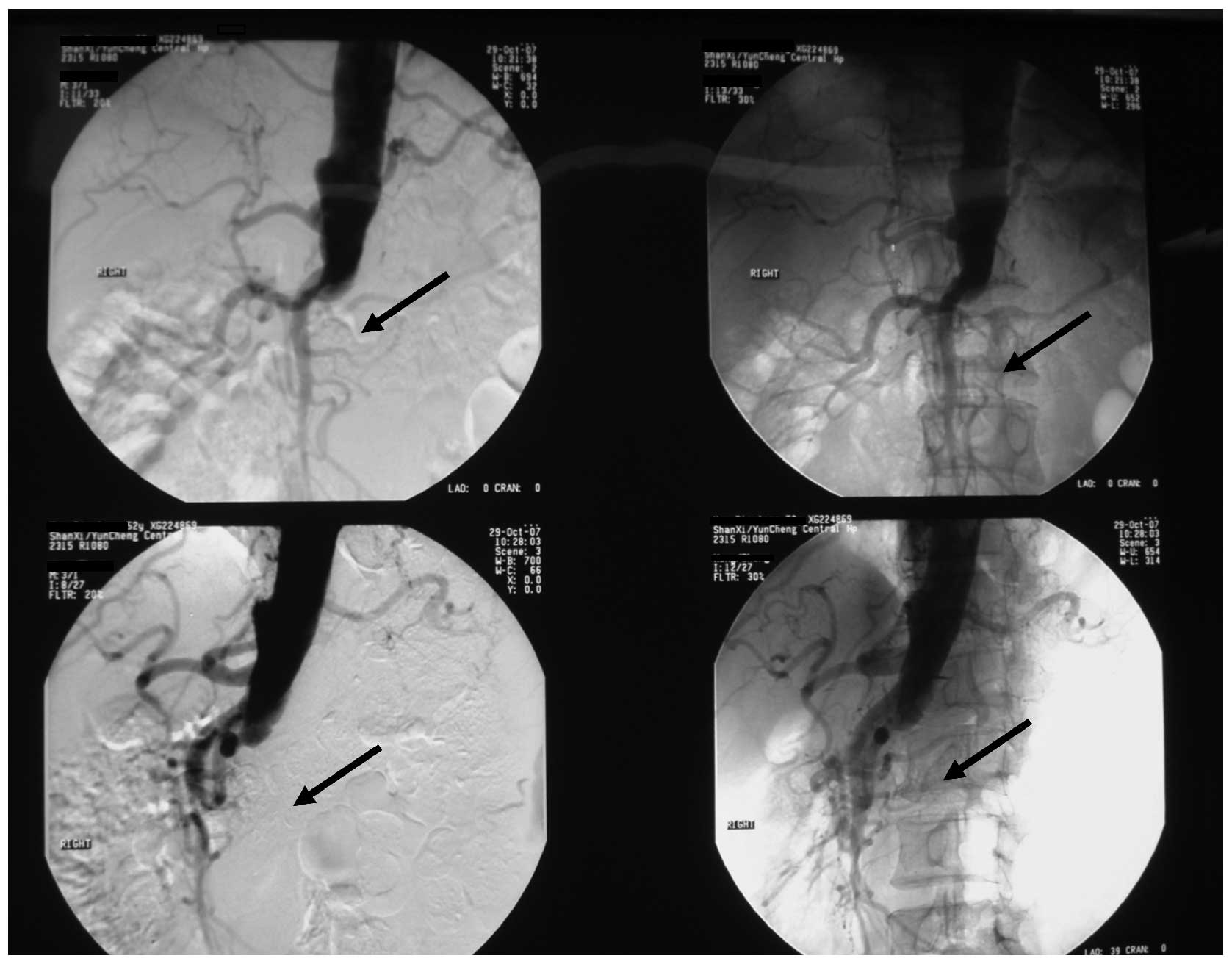
arteries were pulseless. An abdominal CT scan demonstrated an
irregular thrombus-like mass in the infrarenal aorta. MR
arteriography revealed an almost complete occlusion of blood flow
from the infrarenal segment of the abdominal aorta to the aortic
bifurcation (Fig. 1).
Initially, an abdominal aortic aneurysm (AAA) was
diagnosed. Thus, an AAA resection and vascular reconstruction were
planned. However, exposure of the abdominal aorta revealed the
absence of thrombosis in the lumen. Instead, a tumor was identified
covering the entire aortic wall. A section of the tumor was removed
for frozen section analysis. The result suggested a sarcoma that
originated from undifferentiated non-endothelial intimal stromal
cells. Further exposure revealed that the tumor had invaded the
vena cava. However, the patient refused radical surgery involving a
major vascular resection and reconstruction due to the potential
dangers. Therefore, a palliative treatment was decided upon. A
large section of the tumor was removed and axillary bifemoral and
femoro-femoral cross-over bypass grafts were established (Fig. 2).
The post-operative histology confirmed the diagnosis
of a sarcoma. The lower limb pain improved significantly following
the surgery and the patient was administered no other adjuvant
therapies. At the 3-month follow-up appointment, the prosthetic
bypass was patent, however, a local tumor had developed. The
patient succumbed due to extensive metastasis 3 months later.
Discussion
Aortic sarcoma is a rare disease. Aortic tumors are
generally classified into two categories, the intimal-type and the
mural-type, according to the site of the occurrence in the aortic
wall. The intimal-type is a malignant mesenchymal tumor that is
characterized by an intraluminal growth with tract obstruction and
emboli seeding. The tumor grows in the direction of the aortic
lumen, extending along the intima or growing as a polypoidal mass
(4,5). Clinically, the primary presentations
of a patient are symptoms of occlusion, including pulseless and
painful extremities or abdominal pain, rather than symptoms that
are directly associated with the primary tumor (4). The present case describes an
intimal-type sarcoma. The post-operative histological examination
identified spindle cells with various degrees of atypia overlying
an acellular layer that contained collagen in the lumen of the
involved artery. Immunohistochemical staining of the mesenchymal
marker, vimentin, was positive.
The majority of intimal tumors are initially
misdiagnosed as they have the same presentation as aorto-iliac
occlusive or aneurysmal arteriosclerotic diseases (2,3). In
the present study, the patient was first diagnosed with
arteriosclerosis obliterans upon admittance to the community
hospital. No further examinations were performed due to the lack of
imaging instruments. When the patient was transferred to Xijing
Hospital and correctly diagnosed, the tumor had already reached an
advanced stage. In certain cases, hypertension is the primary
manifestation due to renal artery stenosis or occlusion (3,6). Less
commonly, patients may present with a ruptured aneurysm that is
caused by the tumor (7). CT and
angiography provide unique opportunities for the diagnosis and
evaluation of aortic sarcomas. In the present case, CT with
contrast enhancement had a limited role in the evaluation as the
findings were suggestive of a thrombotic aneurysm. Compared with
conventional angiography, MR angiography is more favored as it does
not carry the risks of embolization or contrast-induced renal
failure (8). A previous study has
indicated that transesophageal echocardiography may also reveal an
inhomogeneous and echodense mass with an outer membrane, which is
unlike a thrombus and is suggestive of a primary aortic tumor
(9).
The most effective treatments for an aortic sarcoma
are radical resection and vascular reconstruction. The surgeries
often present difficulties according to the tumor volume, depth of
location and the proximity to the vital organs. For the patient in
the present case, a major vascular resection and reconstruction was
planned, as the aorta and the vena cava were involved. However, the
patient refused radical resection due to the potential dangers. To
improve the pain in the lower extremities, axillary bifemoral and
femoro-femoral cross-over bypass surgeries were adopted. The result
was satisfactory. When dealing with benign aortic occlusive
disease, including abdominal aorta thrombotic aneurysms, ligation
of the proximal neck of the aneurysm with an axillary bifemoral
bypass graft may be considered. Certain studies of single patients
or small collectives have reported that chemotherapy may benefit
the overall survival of patients suffering from aortic sarcomas
(1,4). However, sufficient data are lacking to
provide evidence for this hypothesis (10).
In conclusion, aortic sarcoma is an extremely rare
disease with a poor prognosis. A diagnosis at a relatively early
stage is necessary for a longer survival time. Aortic sarcoma
should be suspected in patients with symptoms of
non-atherosclerotic-related aortic occlusive diseases or distal
embolic events. Radical surgery is the most important treatment.
For patients at advanced stages, palliative surgery may also be
considered in order to improve their quality of life.
References
|
1
|
Mayer F, Aebert H, Rudert M, et al:
Primary malignant sarcomas of the heart and great vessels in adult
patients - a single-center experience. Oncologist. 12:1134–1142.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Van Putte BP, Bollen TL and Schepens MA:
Bleeding sarcoma of the aorta mimicking a symptomatic aneurysm. J
Thorac Cardiovasc Surg. 133:1643–1644. 2007.PubMed/NCBI
|
|
3
|
Karamlou T, Li MK, Williamson WK, Heller L
and Wiest JW: Angiosarcoma of the thoracoabdominal aorta presenting
with systemic hypertension, anemia, and visceral ischemia. Ann Vasc
Surg. 22:459–464. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chiche L, Mongrédien B, Brocheriou I and
Kieffer E: Primary tumors of the thoracoabdominal aorta: surgical
treatment of 5 patients and review of the literature. Ann Vasc
Surg. 17:354–364. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Székely E, Kulka J, Miklós I and Kaliszky
P: Leiomyosarcomas of great vessels. Pathol Oncol Res. 6:233–236.
2000.
|
|
6
|
Iguchi S, Alchi B, Asakawa K, et al:
Leiomyosarcoma of the abdominal aorta: a rare cause of renovascular
hypertension. Hypertens Res. 30:279–283. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Alexander JJ, Moawad J and Cai D: Primary
intimal sarcoma of the aorta associated with a dacron graft and
resulting in arterial rupture. Vasc Endovascular Surg. 40:509–515.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mohsen NA, Haber M, Urrutia VC and Nunes
LW: Intimal sarcoma of the aorta. AJR Am J Roentgenol.
175:1289–1290. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rhee MY, Myong NH and Park YB: Primary
intimal sarcoma of the aorta: role of transesophageal
echocardiography. Circ J. 66:111–113. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
No authors listed. Adjuvant chemotherapy
for localised resectable soft-tissue sarcoma of adults:
meta-analysis of individual data. Sarcoma Meta-analysis
Collaboration. Lancet. 350:1647–1654. 1997. View Article : Google Scholar : PubMed/NCBI
|