Introduction
Pericardial lipomas are rare and mostly asymptomatic
tumors, which are usually detected incidentally during physical
examination (1). The present study
describes a case of a giant pericardial lipoma that was diagnosed
by surgical pathology and presents the ultrasonography, X-ray,
computed tomography (CT) and magnetic resonance imaging (MRI)
imaging findings of the tumor in order to prevent a misdiagnosis.
Written informed consent was obtained from the patient.
Case report
A 45-year-old female suffered from post-exercise
pressure in the chest for one year. The patient was diagnosed at
Henan Provincial People’s Hospital (Zhengzhou, China). An
electrocardiogram revealed a normal sinus rhythm without any
remarkable abnormality.
The chest X-ray (GE Feitian 6000 DR; GE,
Buckinghamshire, UK) revealed a marked enlargement of the cardiac
silhouette without any sign of pulmonary congestion and the
cardiothoracic ratio was 64% (Fig.
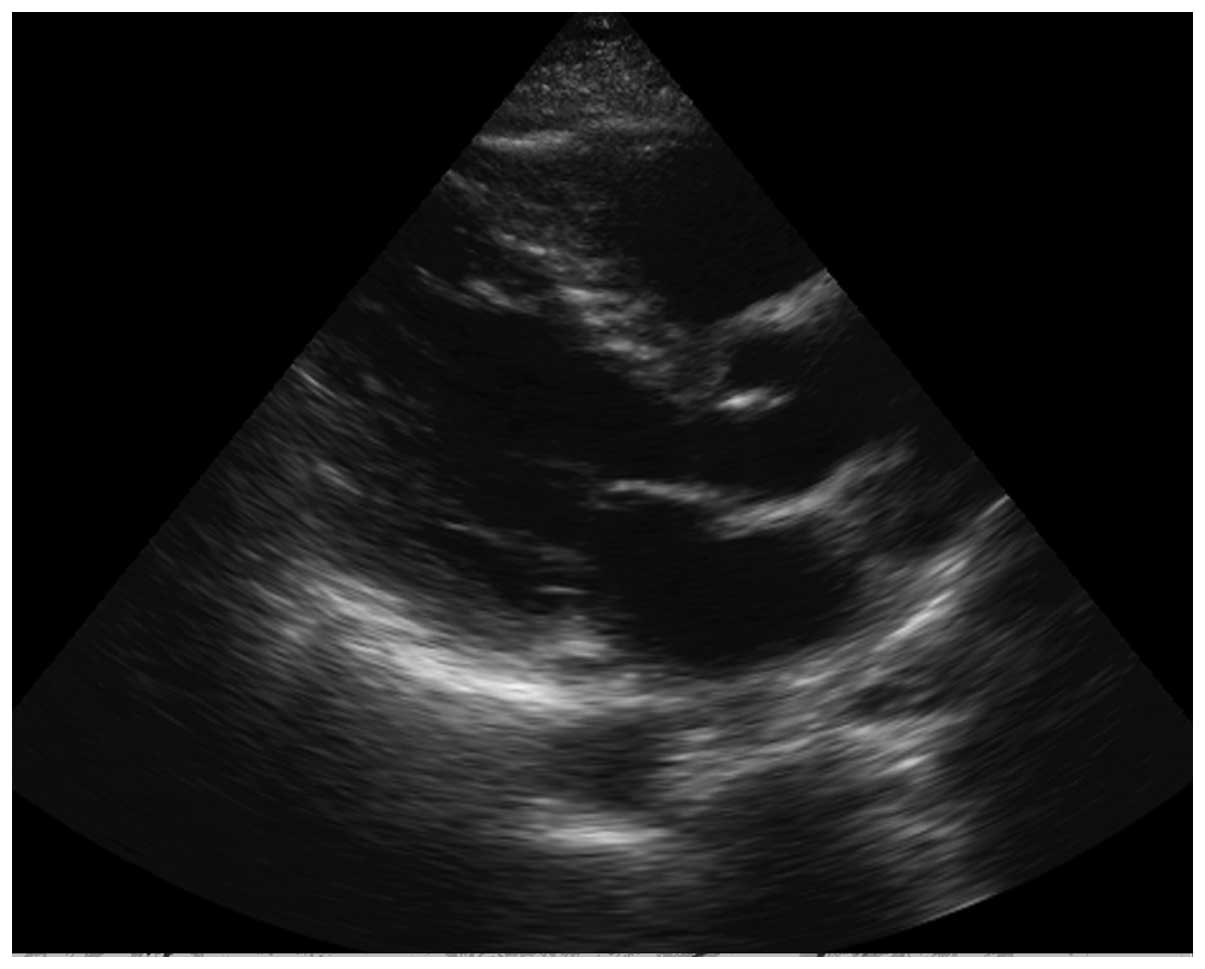
1). A transthoracic echocardiogram (Philips IE33; Philips
Healthcare, Eindhoven, Netherlands) demonstrated a huge echogenic
mass compressing the left and right ventricle (Fig. 2). The size of the mass was
15.6×13.2×5.4 cm3 and the left ventricular ejection
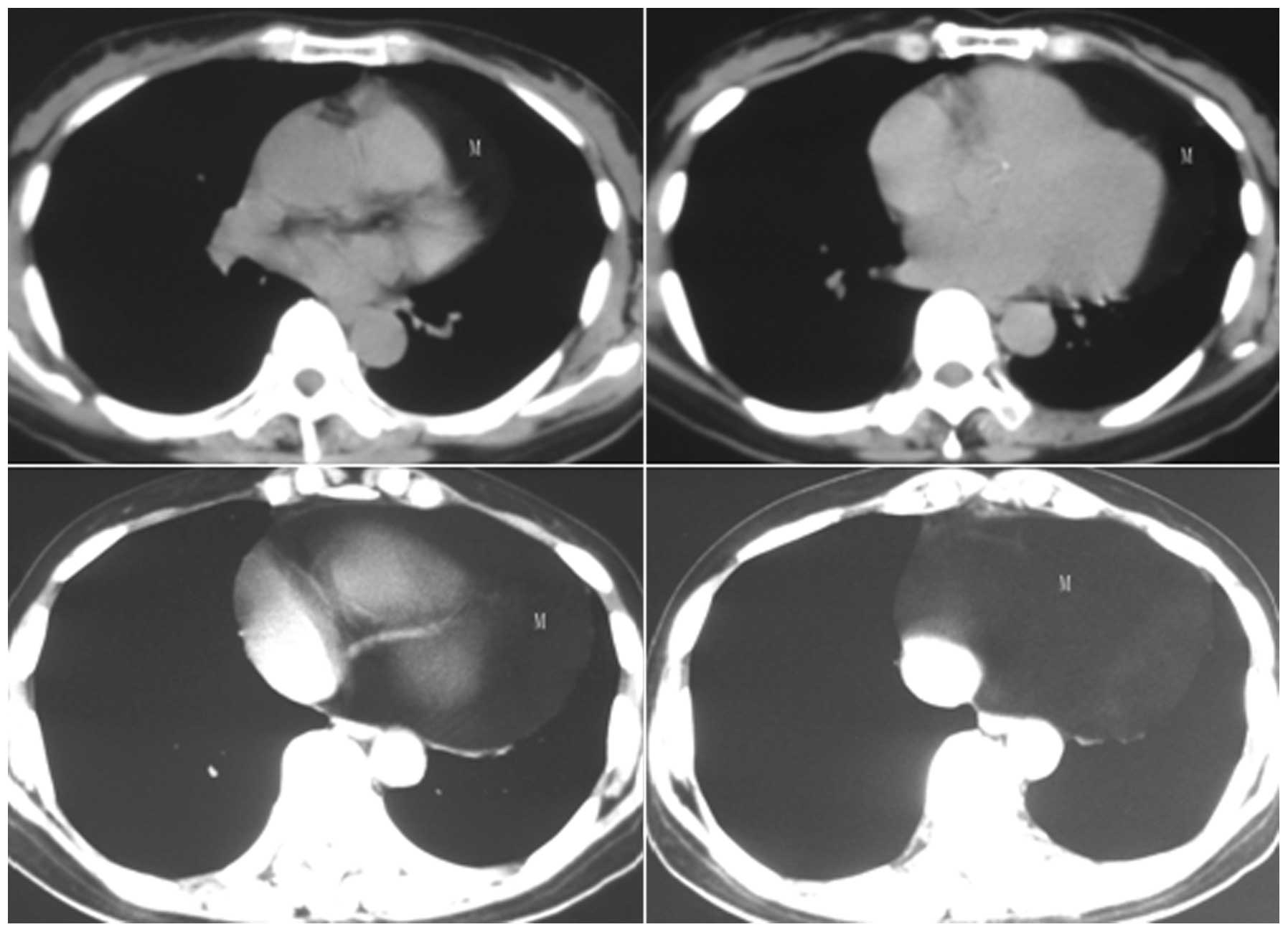
fraction was 66%. Multi-detector computed tomography (Philips
Brilliance 16; Philips Healthcare) plain scan revealed a large mass
along the right, anterior and left epicardial surface. The density
of the mass was equal to that of subcutaneous adipose tissue
(Fig. 3). 3D reconstruction and
contrast CT was not performed in this patient, as the diagnosis of
lipoma had been confirmed using echocardiography and a plain CT
scan.
The patient underwent surgery to remove the mass
under the diagnosis of epicardial lipoma. During surgery, a large,
yellow, soft, encapsulated tumor was identified at the surface of
the heart. The tumor had a 1-cm pedicle that was connected to the
anterior exterior epicardial surface of the left ventricle, with no
invasion to the myocardium and pericardium. The mass was completely
removed, weighed 1,550 g and was 16×14×4 cm3 in size.
Histological examination revealed the nature of the tumor as mature
adipose tissue with inflammatory infiltration in the lipocyte and
envelope, confirming the diagnosis of lipoma (Fig. 4).
The patient was discharged on the tenth
postoperative day and remained asymptomatic in the following three
months. The patient has demonstrated no sign of recurrence by
echocardiography during every three-month follow-up for
approximately one year following the surgery (Fig. 5).
Discussion
Primary cardiac lipomas are rare benign tumors,
which account for 10% of all primary cardiac tumors and 14% of
benign cardiac tumors (2). The
tumor may occur in females or males at any age. The majority of the
patients are asymptomatic, while certain patients may suffer from
discomfort in the chest, dyspnea, palpitation, syncope or sudden
death, depending on the location of the tumor and the possible
resultant compression or obstruction (3).
Generally, cardiac lipomas originate from the
subendocardium, subpericardium or myocardium. A subendocardium
lipoma may appear hemodynamically abnormal or display other
symptoms depending on the location and the size. The tumor may
cause valve regurgitation if the location is near the valve
(4). Subpericardial lipoma is
usually detected late in the clinic and may involve an extremely
large mass that is either symptomless or causes symptoms including
angina on exertion (by compressing the coronary arteries) and
dyspnea (by tamponade). Intramyocardial lipoma may cause
arrhythmias by interfering with the conduction system (2). According to the growth pattern,
cardiac lipoma is classified into two types, invasive and
non-invasive. The former usually infiltrates the adjacent tissue
and is hard to be removed completely with a high recurrence rate.
However, the latter has an envelope and is able to be resected
completely with good prognosis (5).
In the diagnosis of cardiac lipoma, X-ray alone is
not sufficient to reach an exact diagnosis, as it is easily
misdiagnosed. The anatomical definitions, including the location,
size, activity and hemodynamic consequences of the tumor may be
assessed by transthoracic echocardiography, which is usually the
initial examination for patients with a suspected cardiac mass.
Sonography is able to identify an echogenic mass that is similar to
the adipose tissue. When the adipose tissue causes liquefactive
necrosis, it may appear as a low-level echo in the mass (6).
However, an accurate and reliable diagnosis must be
obtained by CT (7) or MRI (8) with an ideal tissue resolution. The
fatty composition of the tumor is easily identified with CT imaging
and the complications of the tumor may be accurately depicted by
reconstructed CT images (1). MRI
scanning with multiple sequences has more advantages in the
diagnosis of lipoma. The homogeneously fatty tumor with
characteristic high-signal intensity on T1-weighted was effectively
suppressed by the application of a fat saturation prepulse, which
is highly specific for epicardial lipoma. In addition, complete
morphological and functional assessment of cardiac tumors may also
be performed by cardiac MRI (9).
The patient in the present study was first diagnosed exactly by
echocardiography and further examinations were performed using CT.
However, a cardiac MRI examination was not performed for the
present patient.
Lipoma should be distinguished from liposarcoma. CT
or MRI are good tools for a differential diagnosis (10). As for liposarcoma, a plain CT scan
usually shows mixed density (−80–40 hU) and calcification is
occasionally observed. Contrast CT shows interior irregularity
enhancement and MRI shows the funicular soft tissue in the fat
tissue. Complete surgical excision of liposarcoma is the best
choice, but the prognosis depends on the pathological type
(11).
Pericardial lipoma should also be distinguished from
mesothelioma of the pericardium, constrictive pericarditis, other
secondary tumors of the pericardium, pericardial cysts and
diaphragmatocele (4). Mesothelioma
of the pericardium shows single or multiple tubercles and an
irregular thickened pericardium (12), with or without hydropericardium
(13). Constrictive pericarditis
shows pericardium thickness, calcification and inferior vena cava
broadening (14). A secondary tumor
of the pericardium has the medical history of the primary tumor.
When the echo level of pericardial lipoma is too low, it is similar
to a pericardial cyst in the echocardiography, but CT and MRI are
able to distinguish the two (15).
When the content of diaphragmatocele is only adipose tissue, it is
difficult to distinguish it from lipoma. The content of
diaphragmatocele that is connected to the abdomen varies between
the two (16).
In summary, although pericardiac lipoma is rare and
seldom encountered, it is not difficult to obtain a correct
diagnosis using the typical imaging findings. The present case
aimed to aid the diagnosis of a cardiac tumor and propose the
initial examination method of ultrasound, location, morphology,
size, activity, internal echo, the association with the surrounding
tissues and the hemodynamic changes. The method also has the
advantage that the technique is cheap and convenient. CT and MRI
have more ideal tissue resolution and a broader visual field than
ultrasound, and are preferred in the imaging of associations with
the mediastinum, lungs, diaphragm and other surrounding tissues.
However, CT and MRI are more expensive than ultrasound and
ultrasound is more convenient for a bedside examination.
References
|
1
|
Xie LX, Chen YS and Liu SY: A giant
cardiac lipoma associated with ventricular inversion and
ventricular aneurysm: ultrasonography and CT imaging findings.
Chest. 141:241–244. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bardakci H, Altintas G, Unal U, Kervan U,
Arda K and Birincioglu L: Giant cardiac lipoma: report of a case. J
Card Surg. 23:254–256. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zwolinski R, Ammer A, Walczak A and
Jaszewski R: Intrapericardial lipoma: diagnosed unexpectedly and
resected during coronary artery bypass surgery. Interact Cardiovasc
Thorac Surg. 11:211–212. 2010. View Article : Google Scholar
|
|
4
|
Puvaneswary M, Edwards JR, Bastian BC and
Khatri SK: Pericardial lipoma: ultrasound, computed tomography and
magnetic resonance imaging findings. Australas Radiol. 44:321–324.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sheppard MN and Mohiaddin R: Tumors of the
heart. Future Cardiol. 6:181–193. 2010. View Article : Google Scholar
|
|
6
|
Auger D, Pressacco J, Marcotte F, Tremblay
A, Dore A and Ducharme A: Cardiac masses: an integrative approach
using echocardiography and other imaging modalities. Heart.
13:1101–1109. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Alkan LM, Metin M, Yener A, et al: A case
of pericardial lipoma diagnosed by noninvasive techniques. Jpn
Heart J. 32:745–749. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tuna IC, Julsrud PR, Click RL, Tazelaar
HD, Bresnahan DR and Danielson GK: Tissue characterization of an
unusual right atrial mass by magnetic resonance imaging. Mayo Clin
Proc. 66:498–501. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gulati G, Sharma S, Kothari SS, Juneja R,
Saxena A and Talwar KK: Comparison of echo and MRI in the imaging
evaluation of intracardiac masses. Cardiovasc Intervent Radiol.
27:459–469. 2004.PubMed/NCBI
|
|
10
|
Stoian I, Piser IT, Kulcsar I, Chioncel O,
Carp A and Macarie C: Rare tumors of the heart - angiosarcoma,
pericardial lipoma, leiomyosarcoma. Three case reports. J Med Life.
3:178–182. 2010.
|
|
11
|
Zehani A, Ayadi-Kaddour A, Daghfous H, et
al: Primary mediastinal sarcomas. Rev Mal Respir. 28:14–24.
2011.(In French).
|
|
12
|
Shah DP, Wong T, Roesch D, Spencer KT and
Lang RM: Echocardiographic diagnosis of malignant mesothelioma
involving the pericardium. Echocardiography. 22:538–539. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Patel J and Sheppard MN: Primary malignant
mesothelioma of the pericardium. Cardiovasc Pathol. 20:107–109.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mastouri R, Sawada SG and Mahenthiran J:
Noninvasive imaging techniques of constrictive pericarditis. Expert
Rev Cardiovasc Ther. 8:1335–1347. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Abu Bakar N, Abdul Aziz YF, Singh Sandhu
R, Fadzli F, Yaakub NA, Krishnasamy S and Raja Mokhtar RA: Imaging
of an atypical pericardial cyst. Heart Lung Circ. 22:305–308.
2013.PubMed/NCBI
|
|
16
|
Weksler B and Ginsberg RJ: Tumors of the
diaphragm. Chest Surg Clin North Am. 8:441–447. 1998.
|