Introduction
Non-melanoma cutaneous cancer is the most common
type of malignancy occurring worldwide and consists primarily of
basal cell carcinoma and squamous cell carcinoma (SCC) (1). Its occurrence is associated with light
exposure, the presence of scars, ethnicity and other factors.
Nasopharyngeal carcinoma is one of the most frequent types of
malignancy in Southern China and is closely associated with
Epstein-Barr virus (EBV) infection (2). The current report presents a case of
left nasal alar cutaneous SCC and nasopharyngeal SCC diagnosed
concurrently. Based on analysis of histology, epidemiology and
etiology of the tumors at the two sites, it was concluded that
cutaneous SCC was the primary carcinoma and that it had
metastasized to the nasopharynx. A brief literature review is also
included on the pathogenesis, epidemiology and diagnosis of
cutaneous SCC and nasopharyngeal carcinoma. The patient provided
written informed consent for the publication of this study.
Case report
A 53-year-old female presented with a scar that was
accompanied by erosion of the left nasal alar skin. The lesion was
2.5 cm in diameter and had originally developed as a papule, which
was 0.3 cm in diameter, five years previously. The patient
scratched the papule due to pruritus, which resulted in breakage,
and repeatedly scratched the site once the breakage had healed,
causing a scar to eventually form. The scar slowly grew during the
repeated process of breakage and healing until the patient was
admitted to Sichuan Provincial People’s Hospital (Chengdu, China)
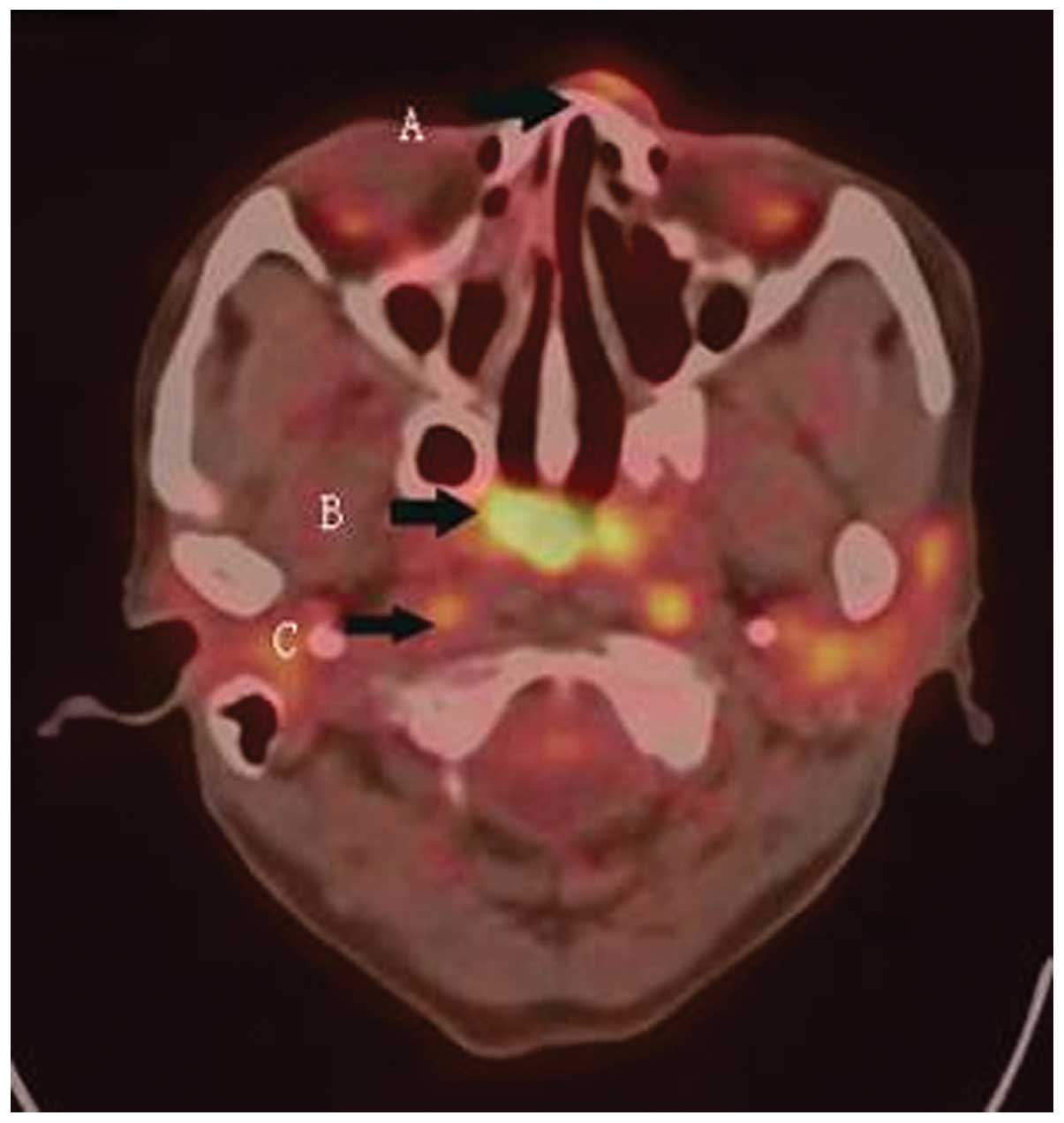
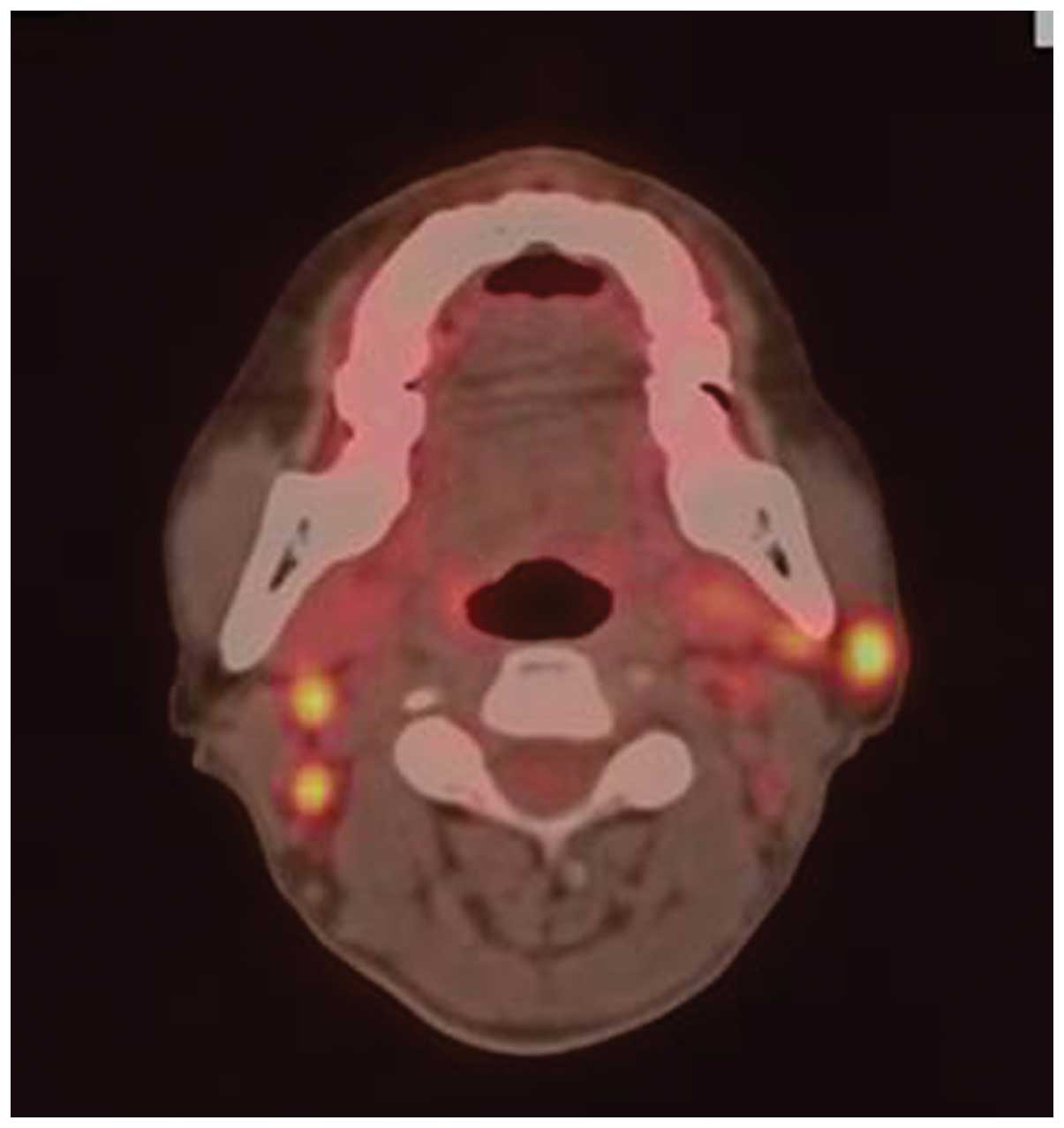
in November of 2011. The patient consented to whole-body
18-fluorine-2-fluoro-2-deoxy-d-glucose (18F-FDG)
positron emission tomography (PET)/computed tomography (CT)
examination, and the results revealed 18F-FDG uptake in
the left nasal alar skin and the right wall of the nasopharynx. In
addition, a number of cervical and parapharyngeal lymph nodes
demonstrated 18F-FDG uptake (Figs. 1 and 2). The left nasal alar lesion was removed
surgically with clear margins, and histological results confirmed
that the lesion was cutaneous SCC with keratosis. Examination with
a nasopharyngoscope was performed, which revealed a neoplasm on the
right wall of the nasopharynx. A biopsy of the neoplasm was
conducted, and the pathology results confirmed that the neoplasm
was SCC with keratosis. EBV-encoded RNA (EBER) was performed in
situ in the nasopharyngeal SCC lesion. The nasopharyngeal tumor
cells were all negative for EBV (Fig.
3). Based on analysis of histology, etiology and epidemiology
of the cutaneous and nasopharyngeal carcinomas, it was concluded
that cutaneous SCC was the primary tumor and that it had
metastasized to the nasopharynx. The patient refused radiotherapy
and chemotherapy, and opted for traditional Chinese medicinal
therapy. The patient succumbed to the disease one year after the
initial examination.
Discussion
SCC is an epithelium-derived carcinoma that
possesses intercellular bridges or characteristics of keratosis
(3). There is a risk of
hematogenous and lymphatic metastasis in SCC cases. The patient in
the current case report presented with SCC at two sites, namely the
left nasal ala and the nasopharynx. This phenomenon is extremely
rare, and three possibilities exist that could explain this case:
i) The two carcinoma sites were both primary tumors; ii) the tumor
of the left nasal ala was a primary tumor that had metastasized to
the nasopharynx; or iii) the tumor of the nasopharynx was a primary
tumor that had metastasized to the left nasal ala. Based on the
findings of this report as discussed below, it was concluded that
the primary tumor occurred on the left nose ala and metastasized to
the nasopharynx.
Non-melanoma skin cancer consists primarily of basal
cell carcinoma and SCC. Of non-melanoma skin cancers, ~80% are
basal cell carcinomas, while 20% are SCC (4). The risk factors for the development of
cutaneous SCC include exposure to ultraviolet or ionizing
radiation, infection with human papillomavirus, ulcers or chronic
injury. Chronic scar formation is regarded as one of the most
important etiological factors in this disease, and SCC is more
likely to develop in skin affected by long-standing ulcers,
radiation dermatitis or vaccination scars. Tumors arising at these
sites may not be identified for years and, if neglected, carry a
substantial risk of metastasis (5).
The cutaneous SCC in this patient was detected in the chronic
cicatricial areas of the skin and gradually grew over five years.
Therefore, it was concluded that the cutaneous SCC on the left
nasal alar skin was the primary tumor.
Multiple primary cancers are also relatively
uncommon. The incidence of multiple primary cancers has been
estimated to be 0.73–11.7% of all cancer patients (6). In a large-scale epidemiological
investigation conducted in Japan, only 4% of male and 1% of female
cancer patients were expected to develop multiple primary cancers
in their lifetime (7). The
incidence of synchronous multiple primary cancers is much lower,
and only one case of synchronous undifferentiated nasopharyngeal
carcinoma and infiltrating ductal carcinoma of the breast has been
reported (8). Therefore, the
probability that the nasopharyngeal carcinoma in this patient was a
synchronous second primary cancer was extremely low.
In addition, nasopharyngeal SCC is relatively
uncommon. The incidence of nasopharyngeal carcinoma is
0.5–2/100,000 individuals in Europe and the USA. However, in
Southern China, nasopharyngeal carcinoma is endemic, with an
incidence of ~25/100,000 individuals (9). The World Health Organization
classifies nasopharyngeal carcinoma into three types: Type I,
moderately differentiated SCC; type II, non-keratinizing squamous
cell, differentiated; and type III, non-keratinizing squamous cell,
undifferentiated (10). Of
nasopharyngeal carcinoma cases, >95% are classified as
non-keratinizing carcinomas (type II) in the nasopharyngeal
carcinoma endemic area, and keratinizing SCCs only account for 3–5%
of all cases (11). According to a
survey conducted by the Sichuan Provincial People’s Hospital, the
proportion of SCCs was only 2.4% of all the nasopharyngeal
carcinoma cases admitted to the hospital between March 2003 and
September 2009 (12).
A marked association between EBV and nasopharyngeal
non-keratinizing carcinomas has been reported, although the
association between keratinizing SCC and EBV is controversial.
However, the majority of researchers in this field still regard
keratinizing SCC as being associated with EBV infection. EBERs are
small non-coding viral RNAs that are abundantly expressed in cells
infected by EBV. Performing EBER detection in situ is
regarded as one of the most sensitive detection methods for EBV.
Zhang et al detected the expression of EBER-1 in all
keratinizing nasopharyngeal SCC cases assessed by the authors
(13). EBER expression has also
been detected in nasopharyngeal SCC cases from several geographical
regions. For example, in a study by Nicholls et al, EBV was
detectable in approximately half of patients from Chengdu, which is
located in central China (14).
The patient in the present case report lived in a
nasopharyngeal carcinoma-endemic area, but the possibility that the
nasopharyngeal carcinoma was a second primary cancer was low due to
the uncommon pathological type and the negative EBER test results.
More importantly, however, the pathological characteristics of the
nasopharyngeal carcinoma in this case were extremely similar to
those of the cutaneous SCC. Histological analysis revealed that the
two lesions were highly differentiated SCC with keratin pearls
(Fig. 4). Based on these findings,
it was concluded that the cutaneous SCC was a primary tumor that
had metastasized to the nasopharynx.
The risk factors of metastasis of cutaneous SCC
include location, size, depth and histological differentiation of
the primary tumor, histological evidence of perineural invasion and
host immunosuppression. The five-year rate of recurrence of primary
cutaneous SCC is 8%, and the five-year rate of metastasis is 5%. In
addition, SCCs arising in injured or chronically diseased skin are
associated with a risk of metastasis that approaches 40% (5,15).
Metastases include regional lymph node metastasis and soft tissue
metastasis (STM), where STM is defined as free soft tissue tumor
deposits lacking continuity with the primary tumor and without
discernible associated lymph node tissue (16). STM can occur by the spread of tumor
cells through lymphatic channels that drain the primary tumor or
through perineural or vascular routes. We hypothesize that the
cutaneous tumor cells of the current patient metastasized to the
nasopharynx through lymphatic channels for the following reasons:
i) tumors with direct vascular invasion may be more prone to
distant spread; ii) there was no clear evidence that the tumor had
invaded nerve fibers (nasal alar skin is controlled by the
infraorbital nerve and does not pass by the nasopharynx); and iii)
18F-FDG PET/CT revealed metastasis to the parapharyngeal
lymph nodes near the nasopharynx. It has been demonstrated in an
animal model that tumor cells may escape the lymphatic system or
travel through small vessels to become free tumor deposits in soft
tissues (17). Therefore, we
speculate that the tumor cells of this patient may have escaped
from lymphatic channels and been deposited in the nasopharynx to
form a metastatic tumor.
Metastasis of nasopharyngeal carcinomas is extremely
rare, which may partly be due to the fact that the nasopharynx is
not a suitable environment for the growth of metastatic tumors. It
is also possible that the nasopharynx is well concealed and
prevents sufficient detection of metastatic lesions. To the best of
our knowledge, this is the first case report describing a case of
cutaneous SCC metastasizing to the nasopharynx [only lung cancer
metastasis to the nasopharynx has been previously reported
(18)]. Therefore, this report may
improve the understanding of the biological character of cutaneous
SCC for practicing physicians.
Acknowledgements
The authors thank Dong DanDan for the pathological
analyses and Xie HongJun for providing the PET-CT images.
References
|
1
|
Cranmer LD, Engelhardt C and Morgan SS:
Treatment of unresectable and metastatic cutaneous squamous cell
carcinoma. Oncologist. 15:1320–1328. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yu MC and Yuan JM: Epidemiology of
nasopharyngeal carcinoma. Semin Cancer Biol. 12:421–429. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jackson DE, Mitchell CA, Bird P, Salem HH
and Hayman JA: Immunohistochemical localization of thrombomodulin
in normal human skin and skin tumours. J Pathol. 175:421–432. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kwa RE, Campana K and Moy RL: Biology of
cutaneous squamous cell carcinoma. J Am Acad Dermatol. 26:1–26.
1992. View Article : Google Scholar
|
|
5
|
Alam M and Ratner D: Cutaneous
squamous-cell carcinoma. N Engl J Med. 344:975–983. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Demandante CG, Troyer DA and Miles TP:
Multiple primary malignant neoplasms: case report and a
comprehensive review of the literature. Am J Clin Oncol. 26:79–83.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kaneko S and Yamaguchi N: Epidemiological
analysis of site relationships of synchronous and metachronous
multiple primary cancers in the National Cancer Center, Japan,
1962–1996. Jpn J Clin Oncol. 29:96–105. 1999.PubMed/NCBI
|
|
8
|
Mesmoudi M, Mahfoud T, Ismaili N, et al: A
synchronous undifferentiated nasopharyngeal carcinoma and
infiltrating ductal carcinoma of the breast successfully treated
with induction chemotherapy followed by local control of both
tumours: a case report. BMC Ear Nose Throat Disord. 11:62011.
View Article : Google Scholar
|
|
9
|
Chan AT: Nasopharyngeal carcinoma. Ann
Oncol. 21(Suppl 7): 308–312. 2010.
|
|
10
|
Bray F, Haugen M, Moger TA, Tretli S,
Aalen OO and Grotmol T: Age-incidence curves of nasopharyngeal
carcinoma worldwide: bimodality in low-risk populations and
aetiologic implications. Cancer Epidemiol Biomarkers Prev.
17:2356–2365. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wei KR, Xu Y, Zhang WJ, Liang ZH and Liu
J: Histologic classification of nasopharyngeal carcinoma. Zhonghua
Bing Li Xue Za Zhi. 40:355–357. 2011.(In Chinese).
|
|
12
|
Zhang L, Ao R, Liu H, Wang JC and Xu G:
Clinical characters of two subtypes in nasopharyngeal
non-keratinizing carcinoma and investigation of clinical
significance. Sichuan Medical Journal. 4:465–467. 2009.(In
Chinese).
|
|
13
|
Zhang JX, Chen HL, Zong YS, et al:
Epstein-Barr virus expression within keratinizing nasopharyngeal
carcinoma. J Med Virol. 55:227–233. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nicholls JM, Agathanggelou A, Fung K, Zeng
X and Niedobitek G: The association of squamous cell carcinomas of
the nasopharynx with Epstein-Barr virus shows geographical
variation reminiscent of Burkitt’s lymphoma. J Pathol. 183:164–168.
1997.PubMed/NCBI
|
|
15
|
Rowe DE, Carroll RJ and Day CL Jr:
Prognostic factors for local recurrence, metastasis, and survival
rates in squamous cell carcinoma of the skin, ear, and lip.
Implications for treatment modality selection. J Am Acad Dermatol.
26:976–990. 1992. View Article : Google Scholar
|
|
16
|
Kelder W, Ebrahimi A, Forest VI, Gao K,
Murali R and Clark JR: Cutaneous head and neck squamous cell
carcinoma with regional metastases: the prognostic importance of
soft tissue metastases and extranodal spread. Ann Surg Oncol.
19:274–279. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Cabanillas R, Secades P, Rodrigo JP,
Astudillo A, Suárez C and Chiara MD: Orthotopic murine model of
head and neck squamous cell carcinoma. Acta Otorrinolaringol Espn.
56:89–95. 2005.(In Spanish).
|
|
18
|
Wong RH, Tse GM, Ng CS, Wan IY, Underwood
MJ and Yim AP: Solitary nasopharyngeal metastasis from lung
primary: a long-term survivor after radiotherapy. Ann Thorac Surg.
92:e13–e14. 2011. View Article : Google Scholar : PubMed/NCBI
|