Introduction
Primary lung cancer is the leading cause of
cancer-related mortality in the majority of industrialized
countries and ~15% of primary lung cancer patients have small cell
lung cancer (SCLC) (1,2). In total, 60–70% of SCLC patients
present with extensive-stage disease (2). Following apparently successful
induction therapy, the majority of patients are diagnosed as
experiencing a relapse within two years due to the emergence of
drug-resistant cancer cells, during the induction therapy, or due
to their presence prior to chemotherapy. As a result, long-term
survival is quite uncommon; <25% of patients with limited-stage
disease and only 1–2% of patients with extensive-stage disease
survive for five years (3,4). The high mortality rate of SCLC is
predominantly attributable to the frequent recurrence of distant
metastasis. Thus, tumor cells may be circulating in the blood of
the majority of SCLC patients at the time of diagnosis irrespective
of whether there is any clinical evidence of distant metastasis or
not. The CellSearch System® (Veridex LLC, Raritan, NJ,
USA) is a commercially available system for detecting circulating
tumor cells (CTCs). Previous studies have shown that CTCs may be
detected in the peripheral blood of approximately half of lung
cancer patients using the CellSearch System®. Detection
of CTC presence and their characteristics may be used to estimate
the risk of metastatic relapse, facilitate stratification of
patients to adjuvant therapy, select therapeutic regimens and
monitor the efficacy of systemic anticancer therapy (5–7). Taki
et al (8) previously
constructed an adenovirus vector termed Telomelysin®
(OBP-301®) that drives the E1A and E1B
genes under the control of the human telomerase reverse
transcriptase (hTERT) promoter, and demonstrated its selective and
supersensitive replication in a variety of viable human cancer
cells. The authors developed a telomerase-specific
replication-selective adenovirus OBP-401 assay
(TelomeScan®; Oncolys BioPharma Inc., Tokyo, Japan), in
which the green fluorescent protein (GFP) gene is driven by a
cytomegalovirus promoter (9).
Telomerase is a ribonucleoprotein complex that is responsible for
the complete replication of chromosomal ends (10,11).
Expression of telomerase activity has been demonstrated in >85%
of human cancers, however, only in limited numbers of normal
somatic cells (12,13). Therefore, telomerase activation is
considered to be a critical step in carcinogenesis and telomerase
activity has been found to closely correlate with hTERT expression
(14). Subsequently, the present
study was conducted to assay the peripheral venous blood of SCLC
patients for the presence of CTCs, using the novel OBP-401 assay,
and investigate whether the CTC count of peripheral venous blood
was associated with prognosis.
Patients and methods
Study design
The current prospective study was conducted at the
Kitasato University Hospital (Sagamihara, Japan). The recruitment
criteria were as follows: i) Histologically or cytologically
confirmed SCLC and confirmation of the clinical stage based on the
results of examination by chest X-ray, computed tomography (CT) of
the chest and abdomen. In addition to other procedures as
indicated, including brain magnetic resonance imaging (MRI) and
positron emission tomography (PET) scanning or radionuclide bone
scanning; ii) chemotherapy-naïve; iii) evaluable or measurable
disease; iv) adequate bone marrow, hepatic and renal function; v)
no active concomitant malignancy; and vi) written informed consent.
Tumor response was classified in accordance with the Response
Evaluation Criteria for Solid Tumors. CT, brain MRI and PET
scanning or radionuclide bone scanning were routinely conducted to
evaluate tumor progression. The institutional review board at the
Kitasato University Hospital approved the study protocol and all
patients provided written informed consent.
A peripheral blood specimen was collected to analyze
the presence of CTCs at each of the following five time periods:
Within seven days prior to commencing treatment (baseline);
chemotherapy cycles two and three; following chemotherapy cycle
four; and the time point at which progressive disease was
confirmed.
CTC detection
The OBP-401 virus was used to detect CTCs as
described previously (15).
Briefly, a 7.5-ml peripheral-vein blood sample was drawn into tubes
containing citric acid, phosphoric acid and dextrose (Nacalai
Tesque, Inc., Kyoto, Japan). The himac CF12RX (Hitachi, Ltd.,
Tokyo, Japan) was used for centrifugation at 540 × g for 5 min.
Following washing with phosphate-buffered saline (PBS) and
RPMI-1640 medium (Sigma-Aldrich, St. Louis, MO, USA) by
centrifugation, the samples were infected with a 4×108
plaque-forming unit of OBP-401 virus for 24 h at 37°C. Each sample
was fixed with 4% paraformaldehyde (Wako Pure Chemical Industries,
Osaka, Japan) and treated with a surface-active agent (Emalgen 2025
G; Kao Chemicals, Tokyo, Japan) to degrade the red blood cells. The
remaining cells were scraped from the slides, applied to glass
slides and examined using a fluorescence microscope (IX71; Olympus
Corporation, Tokyo, Japan).
Immunostaining
The glass slides were soaked in PBS to remove the
coverglass and the cells were scraped from the slides, suspended in
PBS and applied to glass slides by cytocentrifugation in a Cytospin
4 cytocentrifuge (Thermo Fisher Scientific, Waltham, MA, USA). The
cells were subsequently blocked with blocking buffer [1% normal
goat serum (Millipore, Bedford, MA, USA) in PBS] for 1 h at room
temperature and incubated for 1 h at room temperature with mouse
monoclonal anti-pan cytokeratin antibody (ab961; Abcam, Cambridge,
UK). Next, the cells were washed with PBS and treated with Alexa
Fluor 405-conjugated secondary antibody (Invitrogen Life
Technologies, Carlsbad, CA, USA) for 1 h at room temperature.
Following washing with PBS, the cells were mounted and examined
using a fluorescence microscope (IX71; Olympus, Tokyo, Japan) and
the number of CTCs in the 7.5 ml peripheral venous blood was
counted.
Definition of CTC
Previously, GFP-positive cells with relatively small
diameters have been observed in blood samples obtained from cancer
patients and healthy controls (16). The small GFP-positive cells were
double-stained with a variety of anti-CD antibodies
(CD2/3/13/14/15/16/19/45/203c; Biolegend, Inc., San Diego, CA, USA)
to characterize the cell attributes and the results showed that the
majority (~70%) of the small GFP-positive cells were monocytes
(16). Accordingly, to define CTCs
in the blood samples of cancer patients, the cut-off value of cell
diameter for CTCs was determined as >8.4 μm. This value was
deduced from the average value plus two standard deviations, by
analyzing the diameter distribution of monocytes in the blood
samples of healthy controls, which statistically indicated that
>95% of monocytes may be excluded from the GFP-positive cells in
the blood samples of cancer patients. Consequently, in the present
study, GFP-positive cells >8.4 μm in diameter were counted as
CTCs (17). A GFP-positive cell
that was isolated from the peripheral blood of a SCLC patient is
shown in Fig. 1.
Statistical analysis
The primary analysis was a comparison between
overall survival (OS) in the unfavorable and favorable groups
stratified according to the selected threshold of baseline CTC
count. OS and progression-free survival (PFS) were measured from
the date of when the baseline blood sample was collected to the
date when clinical progression was confirmed by mortality or
censoring at the last follow-up examination. PFS and OS curves were
plotted using the Kaplan-Meier method and differences in survival
time were analyzed for statistical significance with the log-rank
test. Student’s t-test was performed to evaluate absolute change in
the mean CTC count. Cox proportional hazards regression was used to
determine the hazard ratios (HRs) for OS, which were adjusted for
age, gender, pretreatment stage (extensive disease versus limited
disease), Eastern Cooperative Oncology Group performance status,
serum lactate dehydrogenase (LDH) levels, serum Na levels and the
baseline CTC count prior to the initiation of chemotherapy.
P<0.05 was considered to indicate a statistically significant
difference and the statistical analysis was performed using the
SPSS for Windows software program, version 17 (SPSS, Inc., Chicago,
IL, USA).
Results
Patient characteristics
The 30 patients with histologically or cytologically
confirmed SCLC (28 males and two females; mean age, 69 years; age
range, 51–85 years; limited disease patients, n=8; and extensive
disease patients, n=22) who met the inclusion criteria between
April 2009 and December 2011 were the subjects of the current
study. The patient characteristics are summarized in Table I. At the time of analysis, 28 of the
30 (93%) evaluable patients had experienced disease progression,
and 25 of the 30 (83%) evaluable patients had succumbed to their
diseases, resulting in a median PFS of 5.7 months (95% CI, 4.8–6.5
months) and median survival time of 11.5 months (95% CI, 9.2–13.7
months). The median follow-up period for determining the survival
time was 12.0 months from the baseline blood sample collection.
 | Table ICharacteristics of 30 patients with
histologically or cytologically confirmed small cell lung
cancer. |
Table I
Characteristics of 30 patients with
histologically or cytologically confirmed small cell lung
cancer.
| Patient
characteristics | Value |
|---|
| Age at baseline,
years |
| Median | 69 |
| Range | 51–85 |
| Gender, n (%) |
| Male | 28 (93) |
| Female | 2 (7) |
| Stage at diagnosis, n
(%) |
| Limited disease | 8 (27) |
| Extensive
disease | 22 (73) |
| Baseline WHO PS, n
(%) |
| 0 or 1 | 20 (66) |
| 2 | 8 (27) |
| 3 | 2 (7) |
| Treatment received, n
(%) |
| Combination
regimen |
| Carboplatin +
etoposide | 11 (36) |
| Cisplatin +
etoposide | 2 (7) |
| Cisplatin +
irinotecan | 1 (3) |
| Carboplatin +
irinotecan | 2 (7) |
| Amrubicin +
irinotecan | 8 (27) |
| Single agent
regimen, n (%) |
| Amrubicin | 6 (20) |
| Laboratory value, n
(%) |
| Na, meq/l |
| ≥135 | 9 (30) |
| <135 | 21 (70) |
| LDH, U/l |
| ≥229 | 10 (33) |
| <229 | 20 (67) |
Evaluating the change in CTC counts
between baseline and after two cycles of chemotherapy
CTCs were detected in 29 of the 30 (96%) patients.
The blood samples following two cycles of chemotherapy (prior to
chemotherapy cycle three) for CTC analysis were obtained from 29
patients. The comparison between the mean CTC count at baseline and
following two cycles of chemotherapy, according to treatment
response, are shown in Table II.
Among the patients who exhibited a partial response (PR) following
two cycles of chemotherapy, the mean CTC count tended to increase
(2.32 cells/7.5 ml) compared with the mean CTC count at baseline
(0.84 cells/7.5 ml) regardless of a reduction in tumor volume
(P=0.05).
| Table IICTC count according to treatment
response following two cycles of chemotherapy. |
Table II
CTC count according to treatment
response following two cycles of chemotherapy.
| Effect of
treatment | n | CTCs base line
(cells/7.5 ml) | CTCsa (cells/7.5 ml) | P-value |
|---|
| PR | 19 | 0.84 | 2.32 | 0.05 |
| SD/PD | 10 | 1.67 | 2.76 | 0.41 |
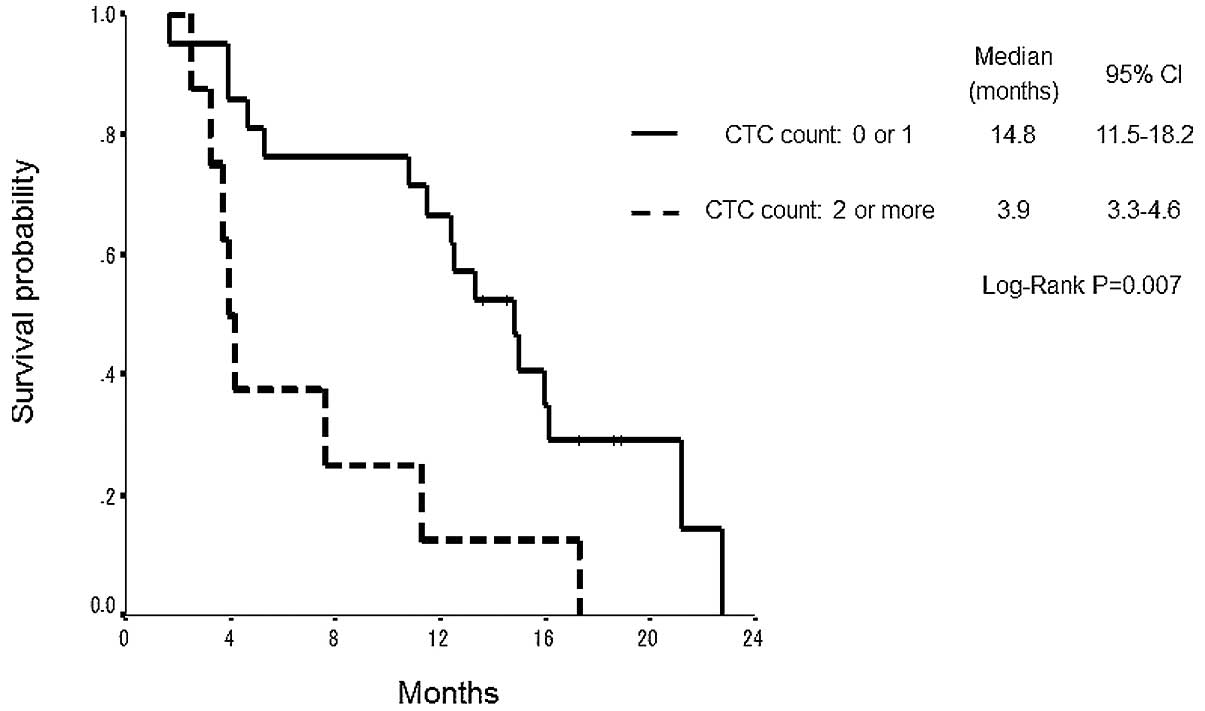
Correlation between the GFP-positive CTC
count and survival time
The group of 21 patients with CTC counts of <2
cells/7.5 ml at the baseline exhibited a significantly longer
median survival time (14.8 months; 95% CI, 11.5–18.2) than the
group of nine patients with a CTC count of ≥2 cells/7.5 ml (3.9
months; 95% CI, 3.3–4.6) (P=0.007; Fig.
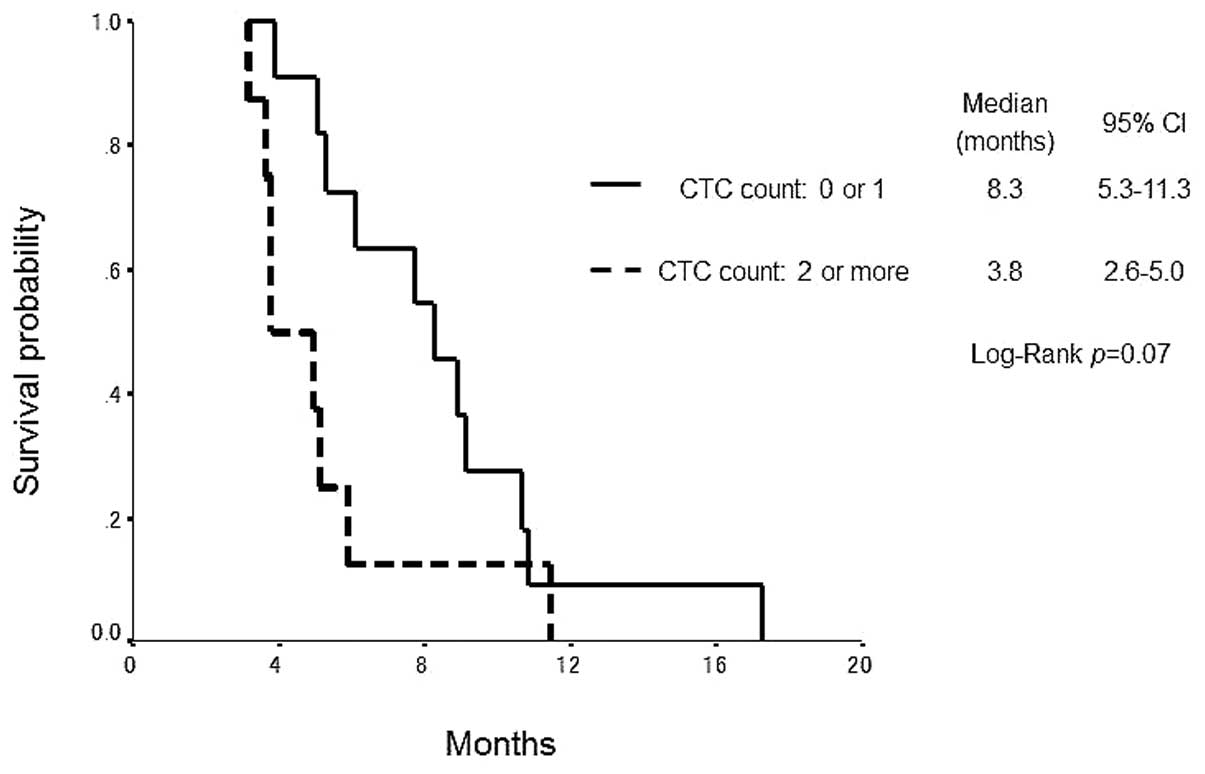
2). The group of patients that exhibited a PR following two
cycles of chemotherapy who had a CTC count of <2 cells/7.5 ml
prior to chemotherapy cycle three tended to have a longer median
PFS (8.3 months; 95% CI, 5.3–11.3) compared with the group with a
CTC count of ≥2 cells/7.5 ml (3.8 months; 95% CI, 2.6–5.0) (P=0.07;
Fig. 3).
Univariate survival analyses and
multivariate Cox proportional hazards regression analysis
The clinical factors that were identified as
significant in relation to survival time in the univariate analysis
were stage at diagnosis, serum LDH levels and baseline CTC count
(Table III). Multivariate
analysis with adjustment for these factors identified all of the
factors (HR, 3.91; 95% CI, 1.19–12.87; P=0.026) to be independent
prognostic markers for OS (Table
IV).
| Table IIIUnivariate Cox regression analysis for
prediction of OS. |
Table III
Univariate Cox regression analysis for
prediction of OS.
| OS rate |
|---|
|
|
|---|
| Parameter | P-value | HR | 95% CI |
|---|
| Gender | 0.84 | 1.23 | 0.16–9.26 |
| M | | | |
| F | | | |
| Age, years | 0.17 | 2.07 | 0.73–5.89 |
| <75 | | | |
| ≥75 | | | |
| PS, n | 0.16 | 1.95 | 0.77–4.99 |
| 0 or 1 | | | |
| ≥2 | | | |
| Na, meq/l | 0.15 | 1.98 | 0.79–4.92 |
| <135 | | | |
| ≥135 | | | |
| LDH, U/l | 0.001 | 12.82 | 2.70–60.61 |
| <229 | | | |
| ≥229 | | | |
| Stage at
diagnosis | 0.014 | 12.52 | 1.68–93.46 |
| Limited | | | |
| Extensive | | | |
| CTC count at
baseline | 0.028 | 2.96 | 1.13–7.76 |
| 0 or 1 | | | |
| ≥2 | | | |
| Table IVStepwise multivariate Cox regression
analysis for prediction of OS. |
Table IV
Stepwise multivariate Cox regression
analysis for prediction of OS.
| OS rate |
|---|
|
|
|---|
| Parameter | P-value | HR | 95% CI |
|---|
| LDH, U/l | 0.012 | 0.13 | 0.027–0.64 |
| <229 | | | |
| ≥229 | | | |
| Stage at
diagnosis | 0.023 | 0.090 | 0.011–0.71 |
| Extensive | | | |
| Limited | | | |
| CTC at
baseline | 0.026 | 3.91 | 1.19–12.87 |
| 0 or 1 | | | |
| ≥2 | | | |
Discussion
Detection of CTCs by the OBP-401 assay has
previously been reported to be useful in the diagnosis, prognosis
and evaluation of therapeutic efficacy in breast and gastric cancer
(15,16,18).
With regard to SCLC, previous studies have reported that higher CTC
counts detected by the CellSearch® System were strongly
associated with shorter SCLC patient survival times (19–21).
The present study was, to the best of our knowledge, the first to
report the detection of CTCs in patients with SCLC using the
OBP-401 assay, as well as being the first prospective evaluation of
CTCs used to predict a prognosis in SCLC patients with the OBP-401
assay.
Various SCLC patients, such as responders or
non-responders to chemotherapy, were inevitably included prior to
commencing treatment. Therefore, attention was restrictively
focused on the CTC counts of patients who had acquired PR following
two cycles of chemotherapy. The patients who responded to
chemotherapy included one group in which the CTC count increased
and another group in which the CTC count decreased compared with
the baseline group of responders, regardless of the reduction in
tumor volume. Additionally, the group of responders with a CTC
count of ≥2 tended to show a shorter PFS compared with the group of
responders with a CTC count of <2 cells/7.5 ml. Accordingly, it
is reasonable to suppose that the CTC count following two cycles of
chemotherapy may be a predictor for the duration of relapse-free
time among responders.
Immunomagnetic cell enrichment, such as that
performed by the CellSearch® system, is currently the
most commonly used technique to detect CTCs (5–7). In
this assay, cells detected with antibodies against epithelial
markers (epithelial cell adhesion molecule [EpCAM]) are determined
to be CTCs. Previous studies have reported that epithelial
mesenchymal transition (EMT) is important in the process of
vascular invasion by tumor cells and results in hematogenous
dissemination (22,23). Thus, it is considered that a
significant number of CTCs are EMT tumor cells and that the
percentage of CTCs that are EMT tumor cells may vary from patient
to patient. Since EMT tumor cells have been reported to only weakly
express epithelial surface antigens, including EpCAM, EMT tumor
cells are less likely to be detected by the Cell Search®
System. The comparison between the OBP-401 assay and
CellSearch® system for analyses of CTCs showed that the
OBP-401 assay does not include the enrichment process of epithelial
surface antigens, including EpCAM. The OBP-401 assay identifies
CTCs on the basis of telomerase expression irrespective of
epithelial surface antigen expression. Accordingly, the OBP-401
assay must be more suitable for the detection of EMT tumor cells
(23–27).
The major limitations of the current study were that
the study population was small and the study was performed at a
single institution. Thus, the threshold value of the CTC count as a
prognostic factor was derived on the basis of results from a study
population at the Kitasato University Hospital alone and was not
independently validated at an additional institution. In addition,
the study population included patients treated by chemoradiotherapy
as well as patients who were treated by chemotherapy alone. Since
the purposes of chemotherapy and chemoradiotherapy are different,
separate derivation studies are required to determine the optimal
threshold value of the CTC count.
In conclusion, the results of the current study
showed that CTCs may be detected by the OBP-401 assay in SCLC
patients and that the CTC count prior to treatment may be a strong
prognostic factor. A large prospective multi-institutional
validation study is required to confirm these results.
Acknowledgements
The authors would like to thank Mr. M. Tanaka and Dr
H. Mitsufuji for their aid in obtaining written informed consent
from the subjects and collecting the blood specimens. The authors
would also like to thank the patients who were involved in the
current study, and Professor Toshiyoshi Fujiwara (Division of
Surgical Oncology, Department of Surgery, Okayama University
Graduate School of Medicine; Okayama, Japan) and Mr. Yasuo Urata of
Oncolys BioPharma Inc. (Tokyo, Japan) for providing OBP-401
(TelomeScan®). The current study was supported by a
grant from Sysmex Corp. (grant no. K09-049 to N.M).
References
|
1
|
Jackman DM and Johnson BE: Small-cell lung
cancer. Lancet. 366:1385–1396. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Govindan R, Page N, Morgensztern D, et al:
Changing epidemiology of small-cell lung cancer in the United
States over the last 30 years: analysis of the surveillance,
epidemiologic, and end results database. J Clin Oncol.
24:4539–4544. 2006.PubMed/NCBI
|
|
3
|
Turrisi AT III, Kim K, Blum R, et al:
Twice-daily compared with once-daily thoracic radiotherapy in
limited small-cell lung cancer treated concurrently with cisplatin
and etoposide. N Engl J Med. 340:265–271. 1999. View Article : Google Scholar
|
|
4
|
Takada M, Fukuoka M, Kawahara M, et al:
Phase III study of concurrent versus sequential thoracic
radiotherapy in combination with cisplatin and etoposide for
limited-stage small-cell lung cancer: results of the Japan Clinical
Oncology Group Study 9104. J Clin Oncol. 20:3054–3060. 2002.
View Article : Google Scholar
|
|
5
|
Alix-Panabières C, Riethdorf S and Pantel
K: Circulating tumor cells and bone marrow micrometastasis. Clin
Cancer Res. 14:5013–5021. 2008.
|
|
6
|
Tanaka F, Yoneda K, Kondo N, et al:
Circulating tumor cell as a diagnostic marker in primary lung
cancer. Clin Cancer Res. 15:6980–6986. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rolle A, Günzel R, Pachmann U, Willen B,
Höffken K and Pachmann K: Increase in number of circulating
disseminated epithelial cells after surgery for non-small cell lung
cancer monitored by MAINTRAC(R) is a predictor for relapse: A
preliminary report. World J Surg Oncol. 3:182005. View Article : Google Scholar
|
|
8
|
Taki M, Kagawa S, Nishizaki M, et al:
Enhanced oncolysis by a tropism-modified telomerase-specific
replication-selective adenoviral agent OBP-405 (‘Telomelysin-RGD’).
Oncogene. 24:3130–3140. 2005.PubMed/NCBI
|
|
9
|
Fujiwara T, Kagawa S, Kishimoto H, et al:
Enhanced antitumor efficacy of telomerase-selective oncolytic
adenoviral agent OBP-401 with docetaxel: preclinical evaluation of
chemovirotherapy. Int J Cancer. 119:432–440. 2006. View Article : Google Scholar
|
|
10
|
Greider CW and Blackburn EH:
Identification of a specific telomere terminal transferase activity
in Tetrahymena extracts. Cell. 43:405–413. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Collins K and Mitchell JR: Telomerase in
the human organism. Oncogene. 21:564–579. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kim NW, Piatyszek MA, Prowse KR, et al:
Specific association of human telomerase activity with immortal
cells and cancer. Science. 266:2011–2015. 1994. View Article : Google Scholar
|
|
13
|
Shay JW and Wright WE: Telomerase activity
in human cancer. Curr Opin Oncol. 8:66–71. 1996. View Article : Google Scholar
|
|
14
|
Nakayama J, Tahara H, Tahara E, et al:
Telomerase activation by hTRT in human normal fibroblasts and
hepatocellular carcinomas. Nat Genet. 18:65–68. 1998. View Article : Google Scholar
|
|
15
|
Kim SJ, Masago A, Tamaki Y, et al: A novel
approach using telomerase-specific replication-selective adenovirus
for detection of circulating tumor cells in breast cancer patients.
Breast Cancer Res Treat. 128:765–773. 2011. View Article : Google Scholar
|
|
16
|
Ito H, Inoue H, Sando N, et al: Prognostic
impact of detecting viable circulating tumour cells in gastric
cancer patients using a telomerase-specific viral agent: a
prospective study. BMC Cancer. 12:3462012. View Article : Google Scholar
|
|
17
|
Yabusaki M, Sato J, Kohyama A, et al:
Detection and evaluation of circulating tumor cells in digestive
system cancers using telomerase-specific adenovirus. In: Proceeding
of 71st annual meeting of the Japan Cancer Association abst; 3395.
2012
|
|
18
|
Takakura M, Kyo S, Nakamura M, et al:
Circulating tumour cells detected by a novel adenovirus-mediated
system may be a potent therapeutic marker in gynaecological
cancers. Br J Cancer. 107:448–454. 2012. View Article : Google Scholar
|
|
19
|
Hiltermann TJ, Pore MM, van den Berg A, et
al: Circulating tumor cells in small-cell lung cancer: a predictive
and prognostic factor. Ann Oncol. 23:2937–2942. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Naito T, Tanaka F, Ono A, et al:
Prognostic impact of circulating tumor cells in patients with small
cell lung cancer. J Thorac Oncol. 7:512–519. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hou JM, Krebs MG, Lancashire L, et al:
Clinical significance and molecular characteristics of circulating
tumor cells and circulating tumor microemboli in patients with
small-cell lung cancer. J Clin Oncol. 30:525–532. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Thiery JP: Epithelial-mesenchymal
transitions in tumour progression. Nat Rev Cancer. 2:442–454. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yilmaz M and Christofori G: EMT, the
cytoskeleton, and cancer cell invasion. Cancer Metastasis Rev.
28:15–33. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sieuwerts AM, Kraan J, Bolt J, et al:
Anti-epithelial cell adhesion molecule antibodies and the detection
of circulating normal-like breast tumor cells. J Natl Cancer Inst.
101:61–66. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Aktas B, Tewes M, Fehm T, Hauch S, Kimmig
R and Kasimir-Bauer S: Stem cell and epithelial-mesenchymal
transition markers are frequently overexpressed in circulating
tumor cells of metastatic breast cancer patients. Breast Cancer
Res. 11:R462009. View
Article : Google Scholar
|
|
26
|
Bonnomet A, Brysse A, Tachsidis A, et al:
Epithelial-to-mesenchymal transitions and circulating tumor cells.
J Mammary Gland Biol Neoplasia. 15:261–273. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lu J, Fan T, Zhao Q, et al: Isolation of
circulating epithelial and tumor progenitor cells with an invasive
phenotype from breast cancer patients. Int J Cancer. 126:669–683.
2010. View Article : Google Scholar : PubMed/NCBI
|