Introduction
Myxoma is a benign tumor of mesenchymal origin
composed of undifferentiated stellate cells in a loose mucoid
stroma with delicate reticulin fibers. The diagnostic criteria of
the myxomas were initially proposed by Stout (1). These tumors develop in a variety of
locations, including the heart, subcutaneous and aponeurotic
tissues, bones, genitourinary tract, skin, retroperitoneum,
intestine, pharynx, joints and skeletal muscles. Myxomas that arise
from skeletal muscles are known as intramuscular myxomas (IMs),
which were described as a distinct subtype of myxomas in 1965 by
Enzinger (2), constituting only 17%
of all soft tissue myxoma cases in his study. IMs have an incidence
of ~1/1,000,000/year, most commonly occur in females, with a ratio
to male patients of 14:3 (3) and
have an adult predominance, with only two cases reported in infants
(4). Myxomas are uncommon in the
oral and maxillofacial region, and develop almost exclusively in
the jaw, where they are considered to be of odontogenic origin. By
contrast, soft tissue myxomas rarely occur in the oral and
maxillofacial region, with IMs that do present in the oral and
maxillofacial region being extremely rare. Following a review of
the literature, it was revealed that only nine cases of IM in these
regions have been documented (Table
I). In the present report, the case of a 74-year-old male with
an IM in the hyoglossus muscle of the tongue is described, with a
brief review of the literature concerning this condition. Patient
provided written informed consent.
 | Table ICases of intramuscular myxoma in the
oral and maxillofacial region, as reviewed in the literature. |
Table I
Cases of intramuscular myxoma in the
oral and maxillofacial region, as reviewed in the literature.
| Case | First author, year
(Ref.) | Location | Age/Gender |
|---|
| 1 | Rosin RD, 1973
(5) | Geniohyoid
muscle | 44/M |
| 2 | Bedrosian SA,
1984 (6) | Masseter muscle | 43/F |
| 3 | Nishijima W, 1985
(7) | Digastric
muscles | 16/F |
| 4 | Mockli GC, 1993
(8) | Tongue | |
| 5 | Serrat A, 1998
(9) | Temporalis
muscle | |
| 6 | van Roggen, 2001
(10) | Right cheek | 56/M |
| 7 | Robin C, 2004
(11) | Temporalis
muscle | 43/F |
| 8 | Papadogeorgakis N,
2009 (12) | Masseter muscle | 74/M |
| 9 | Patsiaoura K, 2009
(13) | Mimetic muscles of
the nasal vestibule | 52/M |
Case report
A 74-year-old male patient presented to the First
Affiliated Hospital of Yangtze University (Jingzhou, China) with a
painless mass in the anterior region of the upper neck that had
been growing slowly for more than five years; the patient noted
that the expansive mass had exhibited a progressive volume increase
within the last six months. The patient also complained that
swallowing food and pronunciation had been affected by the mass.
The patient had no history of trauma, fever or weight loss.
Clinical examination revealed a firm and tender mass (diameter, ~8
cm) in the root of the tongue.
Computed tomography (CT) of the neck revealed a
hypodense lesion located in the anterior cervical region of the
neck, on the hyoid bone within the hyoglossus muscle. The CT value
of the tumor was ~20.3 HU (Hounsfield unit). The oropharyngeal
cavity became narrow as a result of tumor pressure (Fig. 1A) and the diameter of the mass was
~80 mm (Fig. 1B). The imaging
diagnosis characterized the mass as a cystic space-occupying lesion
or lipoma.
Surgical resection was accomplished through a
horizontal incision on the hyoid bone over the tumor site, under
general anesthetic. The tumor was easily separated from the normal
muscle margins of the root of the tongue and the mucous membrane of
the root of the tongue, which was adhered to the tumor was
resected.
The tumor was encapsulated intact and
macroscopically, it exhibited a gray-white appearance and the cut
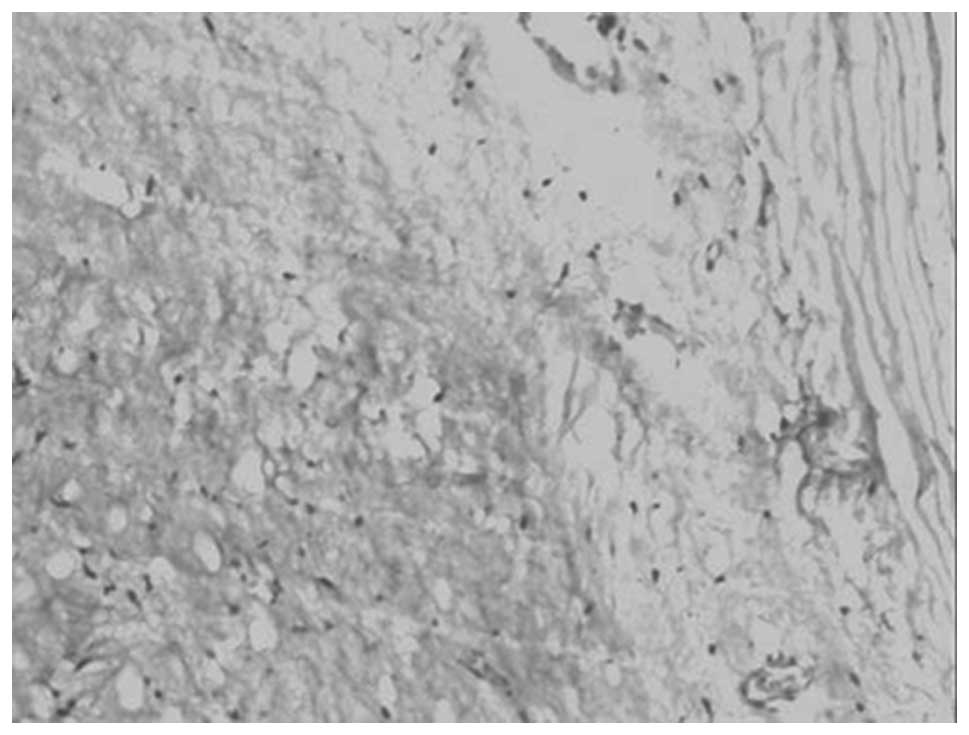
surface of the specimen was ovoid, yellow and gelatinous (Fig. 2). Histopathological analysis
revealed a hypocellular neoplasm of low vascularity, composed of
small spindle-shaped cells, stellate cells and fibers in abundant
myxoid stroma. Mitotic activity, necrosis and nuclear atipias were
absent. The fibrous pseudo-encapsulation of the tumor was
identified and there was no infiltration of the fascicles of the
adjacent skeletal muscle. The neoplastic cells were negative for
S-100 protein expression. The pathological diagnosis of the mass
was an IM (Fig. 3). The patient
experienced an excellent recovery following surgery and was able to
swallow food and speak without pronunciation issues. The follow-up
at three years demonstrated no evidence of local recurrence.
Discussion
In 1871, Virchow (14) used the term myxoma to describe a
lesion that resembled the mucinous substance of the umbilical cord.
The diagnostic criteria of myxomas were first proposed by Stout
(1) and IMs were described as a
distinct subtype of myxomas in 1965, by Enzinger (2). IM is a slow-growing tumor and usually
presents as a painless mass that may exhibit symptoms due to the
compression of surrounding structures (2). The most frequent sites of IMs are the
muscles of the thigh, buttock, shoulder, lower leg, arm and trunk
(2,5). IM in the oral and maxillofacial
location is highly rare. Head and neck intramuscular myxomas
usually occur in patients between the ages of 40 and 60 years
(15). In the present case, the
patient had experienced no pain as a result of the mass for five
years, however, in the six months prior to diagnosis, the mass
began to interefere with the patient’s swallowing and pronunciation
as the oropharynx had been compress by the large mass.
The clinical diagnosis of IM is problematic prior to
microscopic examination due to the oral and maxillofacial location,
as IM exhibits non-specific clinical manifestations. Therefore, the
clinical differential diagnosis includes benign tumors of
mesenchymal origin, for example, benign muscle neoplasms, such as
rhabdomyoma and leiomyoma. In the present case, the patient’s tumor
was located in the root of tongue, therefore various diagnoses
could have been considered, including a more common benign tumor or
cyst of the tongue, such as a dermoid or epidermoid cyst, teratoma
or neurilemmoma. The mass may also have been a rare benign tumor,
such as a tumor arising from the lingual ectopic thyroid or lipoma,
or it may have been a benign salivary gland tumor (pleomorphic and
monomorphic adenoma) arising from the small salivary glands of the
root of the tongue.
The majority of tumors are solitary, however, a
small proportion are multiple and are associated with fibrous
dysplasia. The combination of multiple tumors, or more rarely
solitary IMs, with skeletal fibrous dysplasia in now termed
Mazabraud’s syndrome (16); when an
IM is suspected, the patient must also be examined for fibrous
dysplasia.
IMs lack specific radiographic features and CT scans
typically reveal a cystic-like mass, with a CT value that is
greater than water, but less than the surrounding normal muscle
(17). These radiological features
may be presented in other lesions, such as cystic hygroma, lipoma
and cystic teratoma amongst others. Therefore, it is difficult to
preoperatively diagnose IM using CT scans, and as a result these
tumors are frequently misdiagnosed as cystic hygroma or lipoma.
However, CT scans of these masses is a necessity, as they provide
information regarding the structure of the lesion, including the
tumor size, boundaries and the associations between the tumor and
the surrounding tissues. In the present case, the CT scan revealed
that the mass had sharp borders, with no infiltration of the
adjacent muscle and the tumor was identified as benign. Imaging
diagnosis identified the mass as a cystic space-occupying lesion of
the root of the tongue.
Due to a lack of specific symptoms and common
laboratory tests for identifying IMs, the diagnosis of IMs is
difficult. It is very rare for these tumors to be correctly
diagnosed prior to biopsy and histological examination. It has been
reported that carbohydrate antigen (CA) 19-9, a tumor marker, may
be correlated with IM. In a previous study, the serum level of CA
19-9 increased preoperatively and returned to a normal level six
months following surgery (18),
however, the levels also increased in a variety of other malignant
and benign conditions. The origin and the nature of the tumor can
be established via fine needle aspiration, however, while the
diagnosis of an IM is possible using this method (8,19), the
final diagnosis is always based on the histopathological
examination.
Macroscopic analysis of IMs has demonstrated that
the majority of these tumors are ovoid or globular, and covered by
bundles of skeletal muscle, with a yellow/gray and gelatinous cut
surface. Microscopic visualization using hematoxylin and eosin
staining, shows that IMs are hypocellular, hypovascular, intensely
mucoid and basophilic, and are composed of stellate and
spindle-shaped cells in a myxoid stroma; certain IMs exhibit focal
areas of hypercellularity and hypervascularity (20,21).
Hypercellular zones appear in 76% of IMs and may occupy 10–80% of
the tumor (20) and in these
hypercellular zones, an absence of mitoses, nuclear atypia and
necrosis indicates IM (2,20). In one immunohistochemical analysis,
the neoplastic cells were positive to vimentin and cluster of
differentiation 34, however, were negative for S-100 protein and
smooth muscle actin (3,22).
IMs present as benign masses and there have been no
reports of cases involving metastasis or other malignant changes.
As a result, the treatment for IM is surgical excision, including
enucleation, simple excision and wide local excision. Previous
studies demonstrated several cases of recurrence following
incomplete excision or simple enucleation due to the adjacent
muscle tissue being infiltrated or an incomplete capsule (20,23,24).
However, there were no recurrences of the solitary IMs following
enucleation, simple excision or wide local excision (11,23,25)
and simple excision (with a margin of only a few muscle fibers) is
highly recommended (12,13). In the present case, total removal of
the tumor was performed by simple excision, and the mucous membrane
of the root of the tongue, which was adherent to the tumor capsule,
was resected. There were no signs of recurrence three years
following surgery, therefore, simple excision is considered to be a
feasible method.
In conclusion, the occurrence of IM in the
hyoglossus muscle is highly rare. To the best of our knowledge,
this is the first study of this type of tumor in this region. An
accurate diagnosis prior to surgery is difficult due to a lack of
characteristic clinical history and radiographic findings;
therefore, a CT scan or MRI is required for treatment planning.
Furthermore, IM must be considered in the differential diagnosis of
swellings in the root of the tongue and simple excision was
identified as a feasible method for the treatment of solitary
IM.
References
|
1
|
Stout AP: Myxoma, the tumor of primitive
mesenchyme. Ann Surg. 127:706–719. 1948. View Article : Google Scholar
|
|
2
|
Enzinger FM: Intramuscular myxoma; a
review and follow-up study of 34 cases. Am J Clin Pathol.
43:104–113. 1965.
|
|
3
|
Hashimoto H, Tsuneyoshi M, Daimaru Y,
Enjoji M and Shinohara N: Intramuscular myxoma. A
clinicopathologic, immunohistochemical, and electron microscopic
study. Cancer. 58:740–747. 1986. View Article : Google Scholar
|
|
4
|
Ishoo E: Intramuscular myxoma presenting
as a rare posterior neck mass in a young child: case report and
literature review. Arch Otolaryngol Head Neck Surg. 133:398–401.
2007. View Article : Google Scholar
|
|
5
|
Rosin RD: Intramuscular myxomas. Br J
Surg. 60:122–124. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bedrosian SA, Goldman RL and Pearl MJ:
Intramuscular myxoma of the masseter. J Oral Maxillofac Surg.
42:684–686. 1984. View Article : Google Scholar
|
|
7
|
Nishijima W, Tokita N, Watanabe I and
Takooda S: Intramuscular myxoma of the neck. Arch Otolaryngol.
111:699–701. 1985. View Article : Google Scholar
|
|
8
|
Mockli GC, Ljung BM and Goldman RL: Fine
needle aspiration of intramuscular myxoma of the tongue: A case
report. Acta Cytol. 37:226–228. 1993.
|
|
9
|
Serrat A, Verrier A, Espeso A and Martín
J: Intramuscular myxoma of the temporalis muscle. J Oral Maxillofac
Surg. 56:1206–1208. 1998. View Article : Google Scholar
|
|
10
|
van Roggen JF, McMenamin ME and Fletcher
CD: Cellular myxoma of soft tissue: A clinicopathological study of
38 cases confirming indolent clinical behaviour. Histopathology.
39:287–297. 2001.
|
|
11
|
Robin C, Bastidas JA and Boguslaw B: Case
report: Myxoma of the temporalis muscle. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod. 97:620–624. 2004. View Article : Google Scholar
|
|
12
|
Papadogeorgakis N, Petsinis V, Nikitakis
N, Goutzanis L and Alexandridis C: Intramuscular myxoma of the
masseter muscle: A case report. Oral Maxillofac Surg. 13:37–40.
2009. View Article : Google Scholar
|
|
13
|
Patsiaoura K, Anagnostou E and Benis N:
Intramuscular myxoma of the nasal vestibule. Auris Nasus Larynx.
37:100–102. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Virchow R: Intramuscular myxoma of the
cervical paraspinal muscle. Cellular Pathology as Based upon
Physiological and Pathological Histology. JB Lippincott;
Philadelphia, PA: pp. 525–526. 1863
|
|
15
|
Canalis RF, Smith GA and Konrad HR:
Myxomas of the head and neck. Arch Otolaryngol. 102:300–305. 1976.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cabral CE, Guedes P, Fonseca T, Cruz LC Jr
and Smith J: Polyostotic fibrous dysplasia associated with
intramuscular myxomas: Mazabraud’s syndrome. Skeletal Radiol.
27:278–282. 1998.
|
|
17
|
Crankson SJ, Al Namshan M, Al Mane K and
Bamefleh H: Intramuscular myxoma: a rare neck mass in a child.
Pediatr Radiol. 32:120–122. 2002. View Article : Google Scholar
|
|
18
|
Theodorou D, Kleidi ES, Doulami GI,
Drimousis PG, Larentzakis A, Toutouzas K and Katsaragakis S:
Intramuscular myxoma associated with an increased carbohydrate
antigen 19.9 level in a woman: a case report. J Med Case Rep.
5:1842011. View Article : Google Scholar
|
|
19
|
Mehrotra R, Singh M and Azad V:
Intramuscular myxoma report of a case diagnosed on fine needle
aspiration cytology. Indian J Pathol Microbiol. 47:279–281.
2004.
|
|
20
|
Nielsen GP, O’Connell JX and Rosenberg AE:
Intramuscular myxoma: a clinicopathologic study of 51 cases with
emphasis on hypercellular and hypervascular variants. Am J Surg
Pathol. 22:1222–1227. 1998. View Article : Google Scholar
|
|
21
|
Allen PW: Myxoma is not a single entity: a
review of the concept of myxoma. Ann Diagn Pathol. 4:99–123. 2000.
View Article : Google Scholar
|
|
22
|
van Roggen JFG, McMenamin ME and Fletcher
CD: Cellular myxoma of soft tissue: a clinicopathological study of
38 cases confirming indolent clinical behaviour. Histopathology.
39:287–297. 2001.
|
|
23
|
Ozawa H, Fujii M, Tomita T and Ogawa K:
Intramuscular myxoma of scalene muscle: a case report. Auris Nasus
Larynx. 31:319–322. 2004. View Article : Google Scholar
|
|
24
|
Orlandi A, Bianchi L, Marino B, Spagnoli
LG and Nini G: Intramuscular myxoma of the face: an unusual
localization: A clinicopathological study. Dermatol Surg.
21:251–254. 1995. View Article : Google Scholar
|
|
25
|
McCook TA, Martinez S, Korobkin M, Ram PC,
Bowen JH, Breiman RS, et al: Intramuscular myxoma: Radiographic and
computed tomographic findings with pathologic correlation. Skeletal
Radiol. 7:15–19. 1981. View Article : Google Scholar
|