Introduction
Angiosarcomas are rare soft tissue neoplasms with an
aggressive and disruptive biological behavior, constituting <1%
of all sarcomas, worldwide. The majority of angiosarcomas have a
skin or soft tissue origin and are generally localized to the head
and neck region, or on the lips of patients with lymphedema
(1). Angiosarcoma of the thyroid is
a rare pathological finding, which has been under debate for ~100
years (2–4). Several studies have reported tumors
that exhibit both an anaplastic carcinoma and
pseudoangiosarcomatous appearance and thus, it is difficult to
classify these tumors as either anaplastic carcinomas of the
thyroid or conventional angiosarcomas, according to the WHO
classifications (2–4).
Out of 1,271 excised thyroid samples that were
assessed over a period of six years (between 2008 and 2013) at the
Thyroid Section of the Department of Pathology (Bağcılar Training
and Research Hospital, Istanbul, Turkey), only one case of
angiosarcoma was determined. Together with a literature review, the
current study reports a case of angiosarcoma of the thyroid that
was determined by light microscopy, and endothelial
differentiation, which was identified by immunohistochemistry and
electron microscopy. Written informed consent was obtained from the
patient.
Case report
The patient presented in the current study had
previously undergone surgery at a secondary care health center
(Başakşehir State Hospital, Istanbul, Turkey) following a diagnosis
of undifferentiated thyroid carcinoma. In December 2013, the
patient was subsequently referred to the tertiary care center at
Bağcılar Training and Research Hospital (Istanbul, Turkey). to
receive therapy and consultation. The 62-year-old Turkish female
patient had a history of goiter for ~10 years, however, was not on
any medication at the time of admission. A swelling had been
observed on the right side of the neck, which had grown over the
previous few months, however, as the swelling had not compressed
the esophagus or trachea, no sign of shortness of breath,
difficulty in swallowing or pain was exhibited. When performing
laboratory assessments, the thyroid function tests, blood count and
coagulation profile were within the normal limits. Laboratory
assessments revealed normal levels of free triiodothyronine (2.38
pq/ml; normal range, 2–4.4 pq/ml), free thyroxine (1.16 ng/dl;
normal range, 0.9–1.7 ng/dl) and thyroglobulin (7.25 ng/ml; normal
range, 3–40 ng/ml). However, a low level of thyroid stimulating
hormone was identified (0.01 mU/l; normal range, 0.35–5.5 mU/l).
Furthermore, the patient’s hemoglobin level was 13 gm/dl (normal
range, 12–16 gm/dl), international normalised ratio was 0.65
(normal range, 0.53–1.62) and activated partial thromboplastin time
level was 38.5 sec (normal range, 31.3–54.5 sec). The fine needle
aspiration biopsy (FNAB) was rich in blood elements, however, was
not diagnostic. The patient did not respond well to the repetition
of the aspiration, therefore, elective surgery was proposed and a
bilateral thyroidectomy was performed.
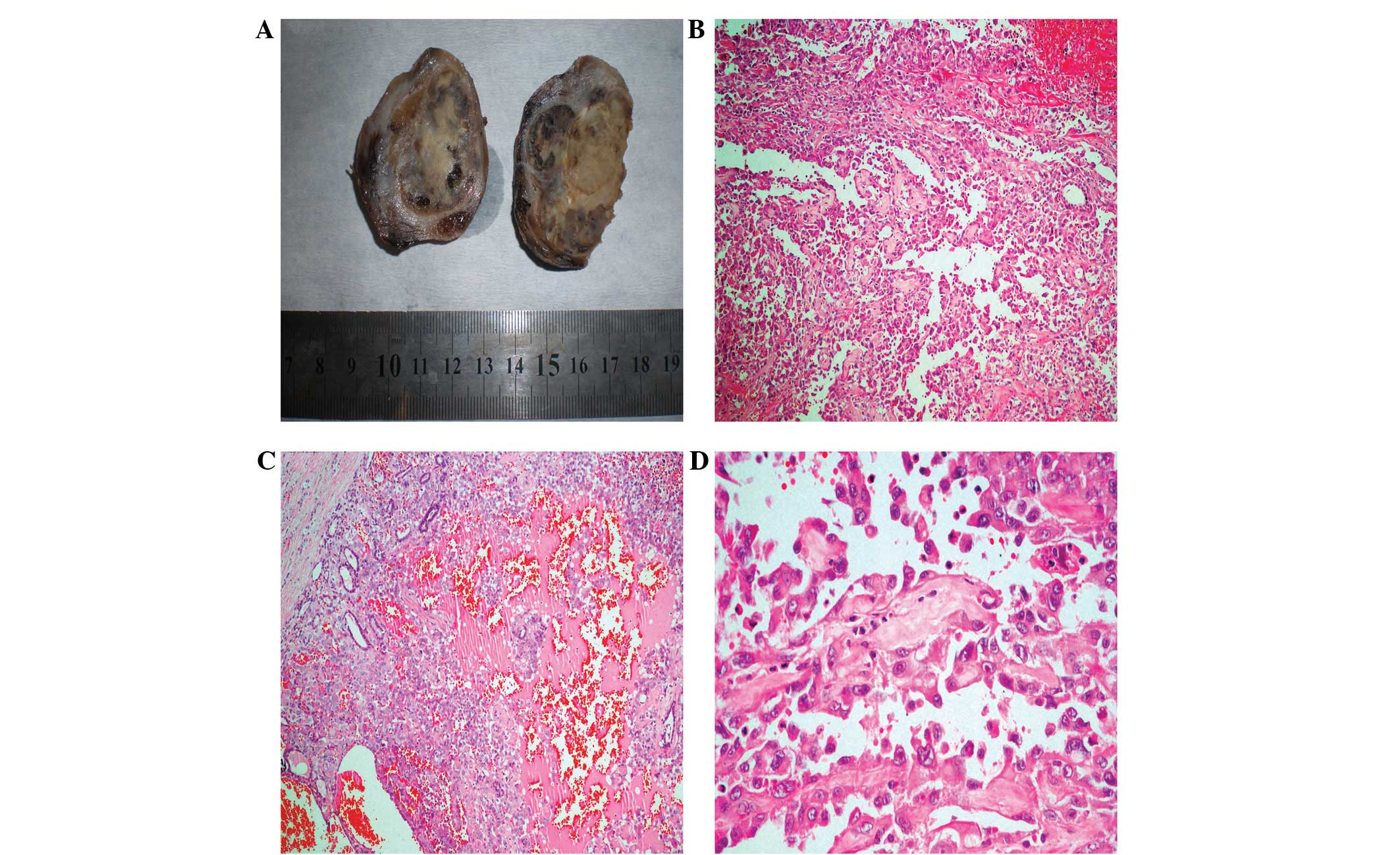
Macroscopically, the right lobe (size, 5×5×3.5 cm;
weight, 50 g) contained a hemorrhagic nodule measuring 3×2 cm in
diameter on the cross section. The left lobe appeared to be normal,
weighing 40 g and measuring 4×3×2.5 cm. Paraffin-embedded tissue
blocks from the samples obtained by FNAB and multiple samples
reprepared from the macroscopic specimen were evaluated together.
Microscopically, nodular structures containing intact follicles
with fibrous capsules were observed at a number of sites, and
exhibited wide hemorrhagic foci at the center. Certain vascular
channels formed anastomoses within the bleeding sites, several of
which resulted in endothelial proliferation, while other channels
were lined by a single layer of epithelial cells. The cells
exhibited large vesicular nuclei and prominent macronucleoli
(Fig. 1). No capsular invasion or
extrathyroidal spread was observed.
Immunohistochemistry revealed that the typical cells
exhibited strong immunoreactivity for CD31 and vimentin, but weak
immunoreactivity for CD34 and factor VIII (FVIII). Strong
cytokeratin (CK) AE1/AE3 staining was occasionally observed, as was
positive staining for thyroglobulin in the abortive follicles among
the atypical cells (Fig. 2). Cells
were identified to be negative for TTF-1, which was applied to
exclude coexistent follicular carcinoma, and HMB-45, which was
applied to exclude malignant melanoma. A diagnosis of angiosarcoma
was determined based on these characteristics and upon observation
of Weibel-Palade bodies, which exhibited endothelial
differentiation that was observed under an electron microscope
(Fig. 3).
At 40 days following the surgery and staging
assessments, whole body imaging with positron emission
tomography-computed tomography was conducted 1 h following the
injection of 11.66 mCi F-18 fluorodeoxyglucose (FDG), while the
fasting blood glucose level was 113 mg/dl. A hypodense lesion,
20×22 mm in size, in the right inferior jugular area was detected,
revealing a peripheral hypermetabolism with a low intensity signal,
compatible with the collection area. Furthermore, lymphadenopathies
were identified in the bilateral jugular chain, which did not
exhibit pathological FDG involvement (Fig. 4). The patient refused additional
complementary surgery and chemotherapy and at the 15-month
follow-up reported no health issues regarding the angiosarcoma.
Discussion
Angiosarcoma of the thyroid, a rare type of sarcoma,
was originally reported in a patient from the mountainous Alpine
region 90 years ago (3,5). Based on a search conducted using
PubMed, to date 48 cases have been reported in the literature
(6). A limited number of cases from
non-Alpine regions have previously been reported (5,7),
however, to the best of our knowledge, this is the first reported
case of angiosarcoma of the thyroid in Turkey from a non-Alpine
region, which was identified by electron microscopy.
In total, 2–10% of all malignant thyroid tumors are
observed with a high incidence in Alpine regions, including
Switzerland, North Italy and Austria (2,5,7). The
patient in the current study had a 10-year history of goiter and
was from the Black Sea region, an endemic goiter region of Turkey.
Although iodine deficiency may be a factor in the etiology of
angiosarcoma, the identification of cases reported from a
non-Alpine region leads to the consideration that additional
factors may also have an impact.
The female gender had a marked predominance in the
distribution of cases presented in the literature and the mean age
in the Alpine regions was 60 years, whereas the mean age was 65.5
years in the non-Alpine regions (7,8). In a
recent study and literature review, it was reported that
angiosarcomas of the thyroid were most frequently identified in
females aged >60 years (6).
Thus, the patient in the present study was comparable with those
from the endemic regions in Europe, with regard to age and
gender.
The diagnosis of angiosarcoma is challenging for
clinicians and pathologists and is one of the most debated vascular
pathologies of the thyroid, when observed in patients from unusual
regions. Certain authors question the existence of angiosarcomas
(4); while others hypothesize that
the reported cases were neoplasms exhibiting angiomatoid
characteristics of anaplastic or undifferentiated carcinomas
(2–4). Additionally, previous studies have
reported that the immunohistochemical detection of endothelial
differentiation and the observation of Weibel-Palade bodies, via
electron microscopy, supports the endothelial origins of
epithelioid angiosarcomas (5,9,10). In
the present case, the diagnosis was determined by electron
microscopic assessment.
When vascular pathologies are exhibited in the
thyroid, immunohistochemical markers that are frequently used by
pathologists may facilitate the differential diagnosis and
determination of a diagnosis of angiosarcoma. The highly sensitive
CD31 antibody is expressed in 90% of angiosarcomas, whereas it is
expressed in ~1% of carcinomas (1).
The immunohistochemical detection of FVIII-related antigens and the
ultrastructural identification of Weibel-Palade bodies confirmed
the occurence of endothelial differention in neoplastic cells
(2,9). Therefore, the endothelial markers,
CD31 and FVIII, in addition to immunopositivity for vascular
markers, CD34 and FVIII related antigen, may be added to the
immunohistochemical panel when determining a diagnosis of
angiosarcoma (11,12). However, the staining may be
associated with marked platelet uptake (2), which may cause confusion during the
diagnosis of angiosarcomas. Additionally, cases that are positive
for pan-CK are determined to be epithelioid angiosarcoma and should
also be taken into consideration (10); strong pan-CK staining was locally
observed in the present case.
It is hypothesized that angiosarcomas are
transitional tumors, which exhibit variable presentations of
mesenchymal metaplasia with endothelial and epithelial
differentiation. Angiosarcomas have not yet been included in the
WHO classification of thyroid tumors (2004) and have instead been
classified under other rare thyroid malignancies of the four major
groups (papillary, follicular, medullar and anaplastic carcinomas)
(13). Despite the continuation of
nosological issues and regardless of where this sarcoma is grouped,
it appears that the distinction of this type of tumor, which
possesses similar prognosis and treatment options to other types of
tumor, remains a topic for academic debate. Although the common
treatment approach is multimodal therapy, which involves obtaining
negative surgical margins and administering adjuvant chemotherapy
with or without radiotherapy, the survival rates are limited to
just a few months (5,7).
In the current case, surgery was performed at an
external center; however, no extrathyroidal spreading was exhibited
and a clean surgical margin was achieved. The patient refused the
additional complementary surgery and chemotherapy options, and is
currently disease-free.
In conclusion, angiosarcoma of the thyroid is a type
of head and neck neoplasm with a poor prognosis, which
morphologically resembles a soft tissue sarcoma, and exhibits
epithelial and endothelial differentiation, as well as
immunoreactivity for pan-CK. In addition, CD31 immunohistochemistry
was identified to be valuable in the differential diagnosis;
however, a variety of markers are required for the diagnosis of
angiosarcoma, such as CD34, FVIII, vimentin and pan-CK.
Furthermore, it was established that electron microscopic
assessment may assist with endothelial differentiation. Finally,
the possibility of angiosarcoma presenting in patients with a long
history of goiter and who originate from a region of endemic
goiter, must be considered.
References
|
1
|
Weiss SW and Goldblum JR: Malignant
vascular tumors. Enzinger and Weiss’s Soft Tissue Tumors. 5th
edition. Mosby; Maryland Heights, MI, USA: pp. 703–732. 2008
|
|
2
|
Mills SE, Stallings RG and Austin MB:
Angiomatoid carcinoma of the thyroid gland. Anaplastic carcinoma
with follicular and medullary features mimicking angiosarcoma. Am J
Clin Pathol. 86:674–678. 1986.
|
|
3
|
Mills SE, Gaffey MJ, Watts JC, et al:
Angiomatoid carcinoma and ‘angiosarcoma’ of the thyroid gland. A
spectrum of endothelial differentiation. Am J Clin Pathol.
102:322–330. 1994.
|
|
4
|
Ritter JH, Mills SE, Nappi O and Wick MR:
Angiosarcoma-like neoplasms of epithelial organs: true endothelial
tumors or variants of carcinoma? Semin Diagn Pathol. 12:270–282.
1995.
|
|
5
|
Maiorana A, Collina G, Cesinaro AM, Fano
RA and Eusebi V: Epithelioid angiosarcoma of the thyroid.
Clinicopathological analysis of seven cases from non-Alpine areas.
Virchows Arch. 429:131–137. 1996.
|
|
6
|
Kaur A, Didolkar MS and Thomas A:
Angiosarcoma of the thyroid: a case report with review of the
literature. Endocr Pathol. 24:156–161. 2013.
|
|
7
|
Goh SG, Chuah KL, Goh HK and Chen YY: Two
cases of epithelioid angiosarcoma involving the thyroid and a brief
review of non-Alpine epithelioid angiosarcoma of the thyroid. Arch
Pathol Lab Med. 127:E70–E73. 2003.
|
|
8
|
Egloff B: The hemangioendothelioma of the
thyroid. Virchows Arch A Pathol Anat Histopathol. 400:119–142.
1983.
|
|
9
|
Tanda F, Massarelli G, Bocincu L and Cossu
A: Angiosarcoma of the thyroid: a light, electron microscopic and
histoimmunological study. Hum Pathol. 19:742–745. 1988.
|
|
10
|
Eusebi V, Carcangiu ML, Dina R and Rosai
J: Keratin-positive epithelioid angiosarcoma of the thyroid. A
report of four cases. Am J Surg Pathol. 14:737–747. 1990.
|
|
11
|
Cutlan RT, Greer JE, Wong FS and Eltorky
M: Immunohistochemical characterization of thyroid gland
angiomatoid tumors. Exp Mol Pathol. 69:159–164. 2000.
|
|
12
|
Papotti M, Arrondini M, Tavaglione V,
Veltri A and Volante M: Diagnostic controversies in vascular
proliferations of the thyroid gland. Endocr Pathol. 19:175–183.
2008.
|
|
13
|
De Lellis R, Lloyd RV, Heitz PU and Eng C:
WHO Classification of Tumours Pathology and Genetics of Tumours of
Endocrine Organs. 8. 3rd edition. IARC Press; Lyon: pp. 49–133.
2004
|