Introduction
Granulosa cell tumors (GCTs) are rare sex
cord-stromal tumors, and are classified into either adult or
juvenile forms and the median age at presentation, for the adult
form is 50 years. GCTs are low-grade neoplasms, whose early
symptoms are uterine bleeding and pain, in addition to pressure
symptoms with a palpable mass (1).
GCTs have a low malignant potential and a strong tendency for late
recurrences, with an incidence of 25–30%. However, hepatic
metastases are rare and account for only 5–6% of all GCT
recurrences (2,3). These rare metastases usually occupy a
wide region of the liver parenchyma as a result of their large size
and may be identified by microscopy due to the presence of
Call-Exner bodies (4). The first
case was reported in the English literature Margolin et al in 1985
(5). As few studies and little data
are available on the subject of metastasis in the liver with a GCT
of the ovary, a metastasis occurring from GCT of the ovary can
easily be misdiagnosed as end-stage PLC, for which surgery may not
necessarily be performed, leading to a deteriorative pathogenetic
condition. Resectioning liver metastases for GCTs is usually
performed only as a palliative procedure rather than as a
therapeutic plan, however it may significantly improve the quality
of life for the patient (6). The
present study reports the case of a patient in whom surgery for GCT
of the ovary was performed >20 years prior to recurrence,
following which, a second surgery was performed that resulted in a
significantly improved quality of life. The patient provided
written informed consent.
Case report
A 62-year-old female was admitted to The Affiliated
Hospital of Guilin Medical University (Guilin, China) in 2013 with
acute abdominal pain and severe malnutrition. Previously, in 1986,
at 35 years of age, the patient had undergone a total abdominal
hysterectomy and bilateral salpingo-oophorectomy (TAH+BSO) for a
stage 1 grade 1 adult GCT of the ovary in the Second Hospital of
Guangxi Province (Guilin, China). The patient did not receive any
adjuvant chemotherapy and remained disease-free until 2013. Upon
admittance to hospital in 2013, the blood test for the
α-fetoprotein (AFP) tumor marker was negative. A computed
tomography (CT) scan of the patient was performed and reviewed. A
2.5-mm slightly enhancing mass was observed in the tumor of
metastasis; the tumor was ~10×15×25 cm in size (Fig. 1). A biopsy was not obtained prior to
surgery. Following the diagnosis of right PLC, surgery was
performed. Recurrences were present on the right hemi-liver and
jejunum, with sparse nodules. A radical hepatectomy involving
segments 5/6, a cholecystectomy and a segmental jejunectomy were
performed. Following the resection, the tissues were delivered to
the Department of Pathology, and then embedded in paraffin and
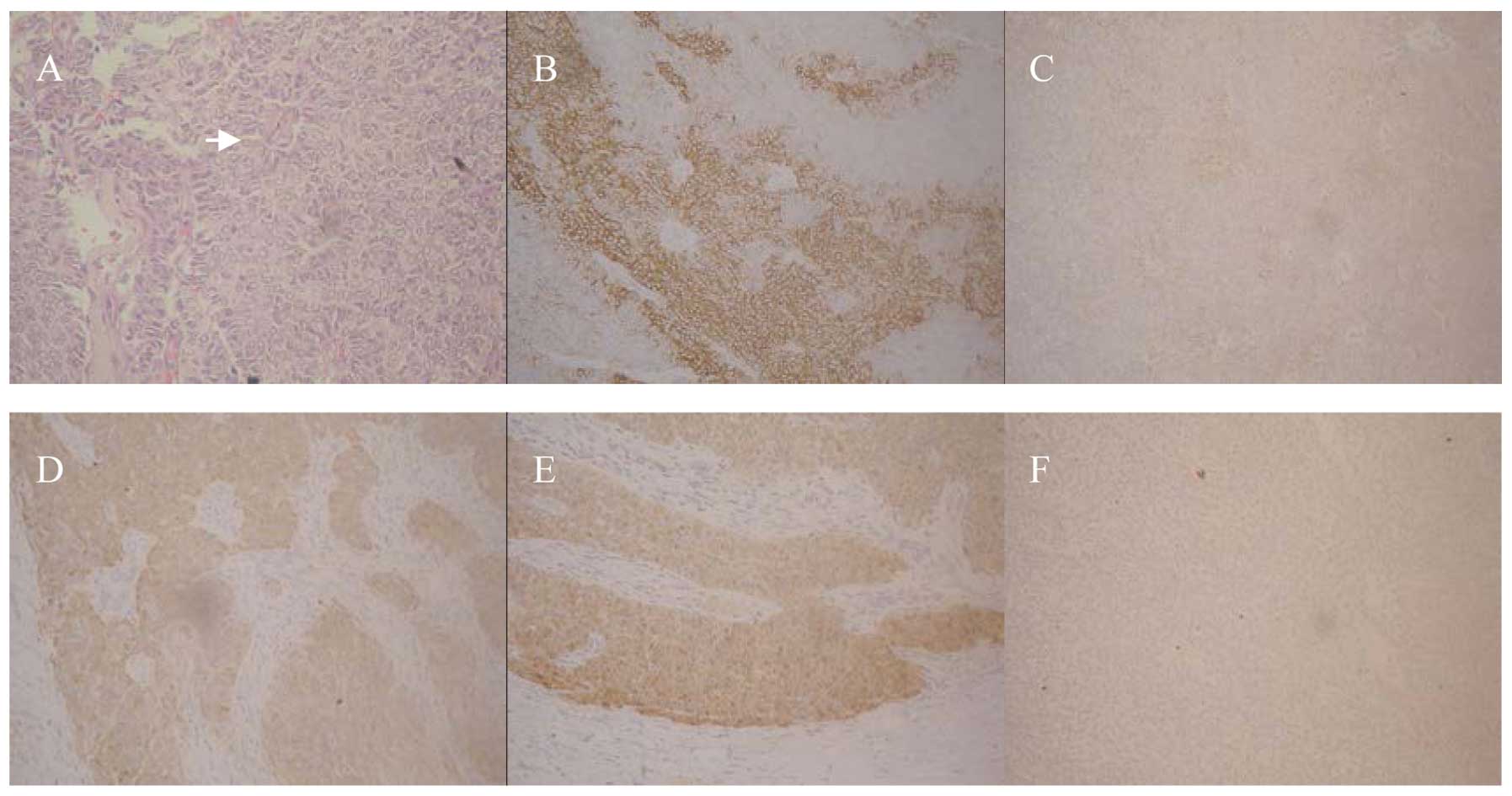
sectioned. The pathological results showed Call-Exner bodies as
microfollicular structures and clear metastasis of the liver, with
GCT of the ovary (Fig. 2).
Immunhistochemistry results revealed positivite staining for CD56,
CD99, inhibin-α and S-100 and negative staining for CK19. The
patient made a good recovery, with resolution of the previous
abdominal pain, and remains disease-free at one year
post-surgery.
Discussion
Ovarian cancer has the fifth highest mortality rate
of all cancers in females, after breast, bowel, lung and uterine
cancer, representing 5–6% of cancer-related mortalities (2). In total, 85% of ovarian cancers arise
from the ovarian surface epithelium; sex cord-stromal tumors
account for 2–5% overall, with GCT being the most common (3). The main characteristics of GCT are the
presence of Call-Exner bodies as microfollicular structures on
microscopy, and immunohistochemistry results showing positive CD56,
CD99, inhibin-α and S-100 staining, but negative CK19 staining.
GCTs are generally low-grade neoplasms associated with a long
disease-free interval due to the indolent nature of the disease,
however, the majority of patients must be manage their condition
and be aware of new symptoms, as the tumors are well known late
recurrences, which occur with an incidence of 25–30% (4). Hepatic metastases rarely occur, with
an incidence of 5–6% of all GCT recurrences (7). The occurrence of these metastases in
only one segment is also rare, as they are almost always large in
size and occupy a wide region of the liver parenchyma (8).
It may be difficult to differentiate GCT from PLC
prior to surgery. In the present study, the patient underwent a
TAH+BSO for stage 1 grade 1 GCT in 1986, and no adjuvant
chemotherapy was administered. The patient remained disease-free
for >20 years until recurrence, which presented as abdominal
pain and a large mass in the liver. Consequently, it is important
that patients with GCT should be followed up regularly, even if the
disease-free interval is long, and that adjuvant treatments may be
reserved for patients with large residual or inoperable tumors. The
literature on GCTs commonly advocates the use of radiofrequency
ablation for hepatic metastases from GCT (9–11).
Historically, surgical resection of liver metastases for GCT was
performed merely as a palliative procedure, and not as a planned
intervention, even though it resulted in a significant increase in
disease-free survival (6). We
believe that the surgical resection of hepatic metastases for GCT
is necessary, particularly in patients who experience a long period
of disease-free survival following the primary surgery. Although
the surgery has certain risk factors, patients may make a good
recovery, with resolution of any previous discomfort, and resulting
in another long disease-free period post-operatively.
In the present study, the patient initially
presented in 2013 with acute abdominal pain and severe
malnutrition. A biopsy was not performed prior to surgery. A
metastatic tumor with a maximum diameter of >25 cm was detected,
and even though the mass was misdiagnosed as a PLC, surgery was
performed to remove the tumor. The patient made a good recovery and
remains disease-free at present.
Although the present reported case is rare, it
indicates the role of surgical resection for hepatic metastases of
GCT, particularly in patients with a record of a long disease-free
period. Doctors, and specifically hepatobiliary surgeons, should be
aware that patients with GCT should be regularly followed up, even
if the disease-free interval is long. Hepatic resection for GCT may
significantly improve a patient’s survival time and quality of
life.
References
|
1
|
Koukourakis GV, Kouloulias VE, Koukourakis
MJ, et al: Granulosa cell tumor of the ovary: tumor review. Integr
Cancer Ther. 7:204–215. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Redman C, Duffy S and Dobson C: Improving
early detection of ovarian cancer. Practitioner. 255:27–30.
332011.PubMed/NCBI
|
|
3
|
Pectasides D, Pectasides E and Psyrri A:
Granulosa cell tumor of the ovary. Cancer Treat Rev. 34:1–12. 2008.
View Article : Google Scholar
|
|
4
|
Hasiakos D, Papakonstantinou K, Karvouni E
and Fotiou S: Recurrence of granulosa cell tumor 25 years after
initial diagnosis. Report of a case and review of the literature.
Eur J Gynaecol Oncol. 29:86–88. 2008.PubMed/NCBI
|
|
5
|
Margolin KA, Pak HY, Esensten ML and
Doroshow JH: Hepatic metastasis in granulosa cell tumor of the
ovary. Cancer. 56:691–695. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Madhuri TK, Butler-Manuel S, Karanjia N
and Tailor A: Liver resection for metastases arising from recurrent
granulosa cell tumour of the ovary - a case series. Eur J Gynaecol
Oncol. 31:342–344. 2010.
|
|
7
|
Rose PG, Piver MS, Tsukada Y and Lau TS:
Metastatic patterns in histologic variants of ovarian cancer. An
autopsy study. Cancer. 64:1508–1513. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lordan JT, Jones RL, Karanjia ND and
Butler-Manuel S: Debulking hepatectomy for an unusual case of a
grade 1 stage 1 granulosa cell tumour of the ovary with late
metastases. Oncology. 72:143–144. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bojalian MO, Machado GR, Swensen R and
Reeves ME: Radiofrequency ablation of liver metastasis from ovarian
adenocarcinoma: case report and literature review. Gynecol Oncol.
93:557–560. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Taira Y, Hirakawa M, Nagayama C, Ikemiyagi
K, Touma T and Tokashiki M: Successful treatment of adult-type
granulosa cell tumor of the ovary by palliative radiotherapy. J
Obstet Gynaecol Res. 38:461–465. 2012. View Article : Google Scholar
|
|
11
|
Jacobs IA, Chang CK and Salti G: Hepatic
radiofrequency ablation of metastatic ovarian granulosa cell
tumors. Am Surg. 69:416–418. 2003.PubMed/NCBI
|