Introduction
Well-differentiated (WD) liposarcoma is the most
common subtype of liposarcoma, accounting for 40–45% of all cases
(1). The most frequent site for WD
liposarcoma is in the deep soft tissues of the thigh, followed by
the retroperitoneum, paratesticular region and mediastinum
(2). Other sites are uncommon and
in particular, primary WD liposarcoma of the mesentery is rare.
Multiple mesenteric WD liposarcoma is extremely rare, with only one
reported case in the English literature (2). The present study describes a case of
multiple mesenteric WD liposarcoma, which was complicated by
purulent inflammation and difficult to diagnose pre-operatively,
and discusses the radiological findings. Informed consent for the
study was obtained from the patient’s family.
Case report
A 59-year-old male was admitted to the emergency
department of Yantai Yuhuangding Hospital (Yantai, China) with
progressive distension of the abdomen that had been apparent for
six months, pyrexia of unknown origin and worsening abdominal pain
that had begun five days earlier. A peak body temperature of 38.8°C
was recorded, with an associated loss of appetite and fatigue being
reported. Blood tests revealed neutrophilic leukocytosis, with an
elevated total white blood cell count of 27.94×109/l
(normal, 3.5–9.5×109/l), and a differential count of
86.0% neutrophils, which was consistent with infection. Physical
examination revealed an ill-defined pelvic-abdominal mass with
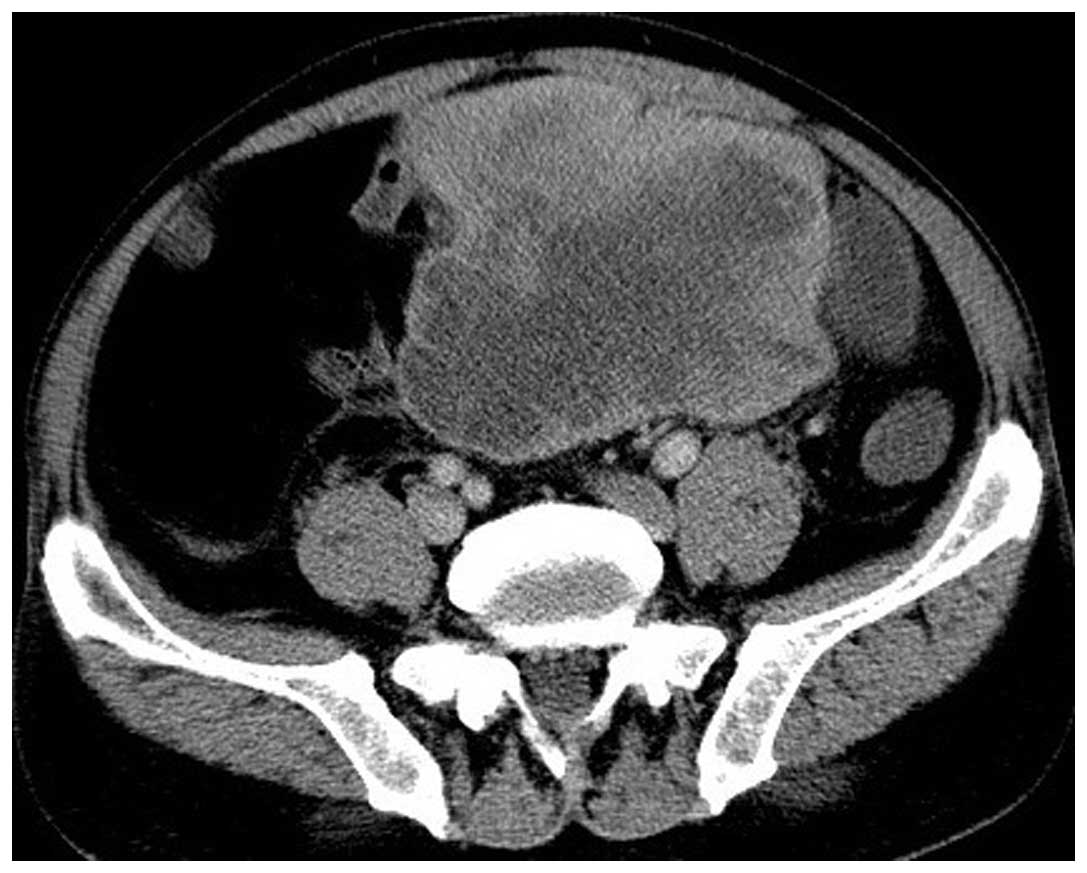
tenderness in the lower abdomen. A non-contrast abdominal computed
tomography (CT) scan performed in the emergency department revealed
a large abdomino-pelvic mass, which extended from the upper pole of
the kidney to the pelvis. The mass was composed of two components,
a main portion of fatty density and a non-adipose solid portion
located within the lower part (Fig.
1). The fatty portion was characterized by an extensive
infiltrative distribution and the absence of delimitation by a
capsule. The mass demonstrated a heterogeneous texture, with coarse
septa, patchy soft-tissue components and punctate calcification.
The non-adipose solid portion was partially ill-defined and
measured 11.6×11.7 cm. The lesion displaced and entrapped the small
bowel loops. A pre-operative diagnosis of abdomino-pelvic
lipomatosis complicated by infection, was established based upon
the clinical characteristics, laboratory results and CT
findings.
The patient was admitted to Yantai Yuhuangding
Hospital and treated conservatively with broad-spectrum
antibiotics. Over the following seven days, the fever remained
constant, with temperatures between 37.8 and 38.6°C, and the
peripheral white blood cell count remained elevated. On the eighth
day post-admission, the mass was re-evaluated using CT intravenous
contrast enhancement, which revealed an increase in the diameter of
the non-adipose solid mass. The longest diameter measured 14.2×16.0
cm (Fig. 2). The non-adipose solid
mass displayed heterogeneous enhancement with hypodense areas,
which indicated hemorrhage, necrosis or abscess formation (Fig. 3). The coarse septa and patchy
non-adipose components demonstrated minimal homogeneous
enhancement.
A laparotomy was performed for symptomatic relief
and to obtain a definitive diagnosis. Intra-operatively, numerous
separated fatty nodules and masses, with sizes ranging between 1
and 15 cm, were attached to the mesentery of the small intestine.
The largest of the masses measured 14×15 cm, was greenish-yellow in
color, and was solid with wide areas of necrosis, hemorrhage and
abscess formation. The other masses were soft, yellow and
homogeneous in consistency. There was no evidence of peritoneal
dissemination, ascites or invasion to adjacent organs in the
abdominal cavity. The majority of the tumors were separated and
removed, but an en bloc resection was impossible to perform due to
the large number of small nodular lesions.
The histological analysis of the solid mass revealed
atypical adipocytes with various sizes of fat vacuoles. The
abundant inflammatory cells consisted predominantly of neutrophils,
which were widely distributed throughout the tumor in the fibrous
septa and the adipocytic areas. There were apparent regions of
extensive necrosis and hemorrhage, which were densely infiltrated
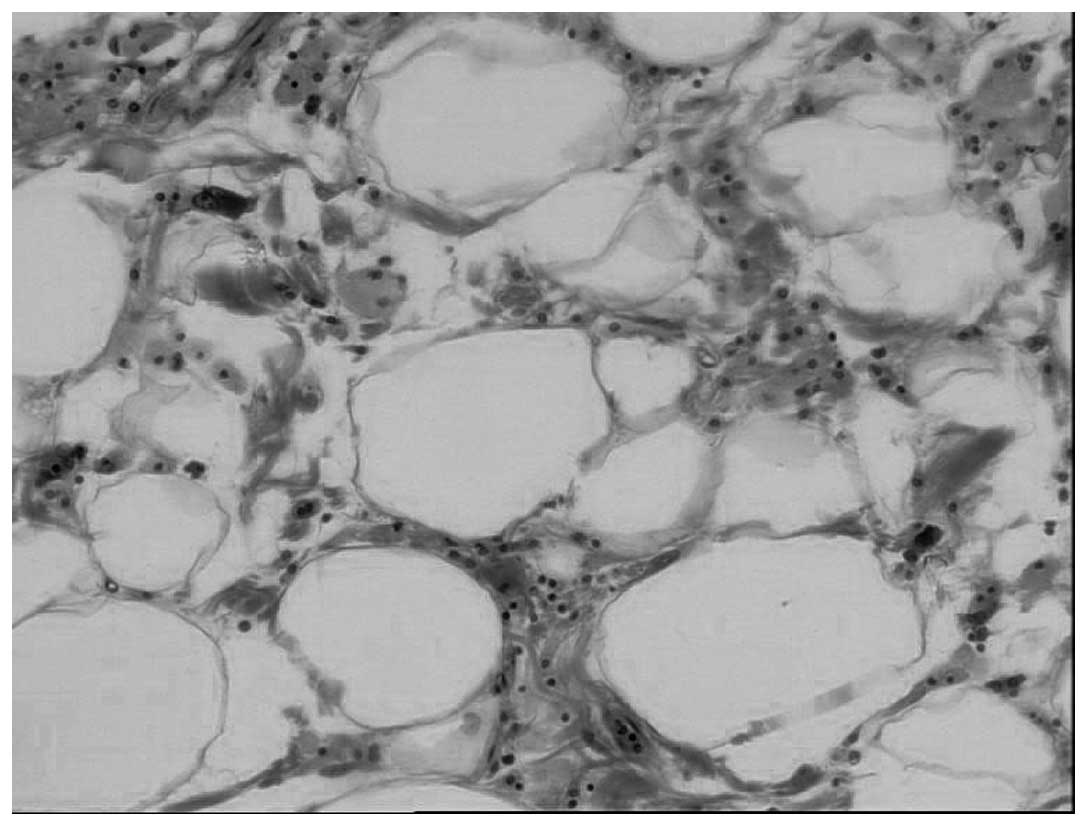
by neutrophils (Fig. 4). The
sections from the other nodules and masses demonstrated
characteristic histopathological features of a WD liposarcoma, and
were composed of atypical adipocytes with various sizes of fat
vacuoles. Unusual stromal cells and bistiocytes were scattered
within the fibrous septa. Rare lipoblasts were also observed in
certain samplings (Fig. 5).
Immunohistochemically, tumor cells were positive for S-100 and
negative for smooth muscle actin. The final diagnosis was of an
adipocytic subtype of multiple mesenteric WD liposarcoma, with the
largest of the tumors complicated by purulent inflammation. The
patient underwent an uneventful post-operative recovery, and the
pyrexia resolved completely following surgery. The patient was
discharged on post-operative day 10. No radiotherapy or
chemotherapy has been administered in the post-operative period.
There were no complaints or complications during the one-year
follow-up. A definite abdominal mass was not identified by CT scan
performed 12 months after the surgery.
Discussion
Liposarcoma is a sarcoma of mesenchymal origin,
which affects soft tissues of the body, in particular the
extremities and the retroperitoneum. On rare occasions, the tumor
may affect the mesentery. Primary mesenteric liposarcomas usually
arise between 50–70 years of age, and exhibit a higher incidence in
males compared with females (3).
The clinical presentation can vary, but symptoms often include
abdominal pain, distension, the presence of a palpable mass,
constipation, vomiting and weight loss (4). In the present study, the patient
presented with pyrexia of unknown origin, most likely caused by
tumor necrosis and infection.
Histologically, liposarcoma can be divided into five
subtypes, myxoid, pleomorphic, dedifferentiated, round cell or WD
(5). Upon CT, liposarcoma exhibits
contrast enhancement, poor margination, CT attenuation greater than
those of normal fat, and inhomogeneity (6). WD liposarcoma can be subdivided into
the lipoma-like, sclerosing, inflammatory and spindle cell groups
(5). At present, there is no
radiologically reliable method that differentiates between these
subtypes.Upon imaging, WD liposarcoma appears as a soft-tissue
mass, consisting predominantly of adipose cells, with
non-lipomatous components. These non-lipomatous features include
septa, which are often >2 mm, and small foci, <2 cm in size,
consisting of nodular or globular non-adipose tissue (7). In addition, calcifications may be
present within the lesion (8). The
lesion in the present case was predominantly fatty in nature, with
scattered coarse septa, patchy soft-tissue components and punctate
calcification, which is consistent with WD liposarcoma.
Multiple mesenteric WD liposarcoma is an extremely
rare entity, and at present only one case has been reported in the
literature (2). A pre-operative
diagnosis of a multiple mesenteric WD liposarcoma may be
challenging due to the rarity and lack of awareness of the tumor.
The CT features of the lesion in the present study were
characterized by an extensive infiltrative distribution of
dishomogeneous lipomatous tissue in the abdomino-pelvic cavity,
which not only displaced, but also entrapped the small bowel loops.
These CT findings differ from those of simple WD liposarcomas,
which exhibit well-defined and mainly lobulated margins (1). By contrast, the large non-encapsulated
fatty tissue in the abdomino-pelvic cavity in the present case led
to a pre-operative diagnosis of lipomatosis, which is a rare benign
disease characterized by an overgrowth of non-encapsulated fatty
tissue, most commonly in the abdominal and pelvic cavities
(9). The large fatty mass of
lipomatosis lacks widened septa, and with the exception of its
extensive infiltrative distribution, resembles a simple lipoma. In
retrospect, the neglect of the multiple coarse septa within the
fatty tissue mass, as well as the rarity and lack of awareness of
the tumor, are potential reasons as to why multiple WD liposarcoma
was not pre-operatively suggested in the present case.
The unusual aspect of the present case was the
evidence of necrosis, hemorrhage and abscess formation on a WD
liposarcoma. This occurrence appears to be rare, as a PubMed search
using the keywords ‘well-differentiated liposarcoma’ and ‘abscess
or purulent inflammation’ did not yield any results. The
inflammatory tumor in the present study differs from the
inflammatory variant of a WD liposarcoma, radiologically and
histopathologically. CT revealed that the inflammatory tumor in the
present study appeared as a large solid mass with inhomogeneous
contrast-enhancement. The imaging features of inflammatory WD
liposarcoma are not significantly different from their commoner
counterparts (7). Upon microscopic
analysis, the inflammatory tumor in the present study was
characterized by mature adipocytic proliferation, which was
infiltrated by abundant neutrophils. By contrast, the inflammatory
cells consist predominantly of plasma cells and lymphocytes in the
inflammatory variant of WD liposarcoma (10). Therefore, the inflammatory tumor in
the present study does not appear to belong to the spectrum of WD
inflammatory liposarcoma.
It should be noted that the presence of large,
low-density fat with a large, non-adipose mass may raise the
possibility of a dedifferentiated liposarcoma, which is a biphasic
WD liposarcoma with a high-grade pleomorphic sarcoma (11). Upon CT, the solid lesions of
dedifferentiated liposarcomas are well-demarcated, with distinct
planes between fat and solid tumor. The solid mass observed in the
present case however was partially ill-defined. Furthermore, in the
present case, the re-evaluated CT scan, which was performed eight
days after the initial scan, identified a remarkable enlargement of
the solid mass. Based upon these CT findings, as well as the
presence of leukocytosis and neutrophilia, the most likely
diagnosis should be of inflammatory WD liposarcoma, rather than
dedifferentiated liposarcoma.
To summarize, the present study reported a case of
multiple mesenteric WD liposarcoma, which was complicated by
purulent inflammation. The CT features of these multiple tumors
were characterized by extensive infiltrative distribution of
lipomatous tissue with coarse septa and patchy soft-tissue
components. The inflammatory tumor appeared as a large, solid mass
and demonstrated heterogeneous enhancement with hypodense areas,
which corresponded to hemorrhage, necrosis and abscess formation.
Multiple mesenteric WD liposarcoma is an extremely rare entity.
This variant should be considered when evaluating a massive
infiltration of dishomogeneous lipomatous tissue in the abdominal
and pelvic cavity. The present study also revealed that
abdomino-pelvic WD liposarcoma can be complicated by purulent
inflammation. Radiologists should therefore consider this when
establishing differential diagnoses for patients with a fever of
unknown origin and the occurrence of a primarily fatty, WD
liposarcoma in close proximity to a non-lipomatous mass, as
observed in the present study.
References
|
1
|
Laurino L, Furlanetto A, Orvieto E and Dei
Tos AP: Well-differentiated liposarcoma (atypical lipomatous
tumors). Semin Diagn Pathol. 18:258–262. 2001.
|
|
2
|
Sachidananda S, Krishnan A, Ramesh R and
Kuppurao S: Primary multiple mesenteric liposarcoma of the
transverse mesocolon. Ann Coloproctol. 29:123–125. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Moyana TN: Primary mesenteric liposarcoma.
Am J Gastroenterol. 83:89–92. 1988.PubMed/NCBI
|
|
4
|
Sato T, Nishimura G, Nonomura A and Miwa
K: Intra-abdominal and retroperitoneal liposarcomas. Int Surg.
84:163–167. 1999.PubMed/NCBI
|
|
5
|
Dei Tos AP and Pedeutour F: Atypical
lipomatous tumor/well-differentiated liposarcoma. Pathology and
Genetics of Tumours of Soft Tissue and Bone, WHO Classification of
Tumours. Fletcher CDM, Unni K and Mertens F: IARC Press; Lyon: pp.
35–46. 2002
|
|
6
|
Hirakoba M, Kume K, Yamasaki M, Kanda K,
Yoshikawa I and Otsuki M: Primary mesenteric liposarcoma
successfully diagnosed by preoperative imaging studies. Intern Med.
46:373–375. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
O’Regan KN, Jagannathan J, Krajewski K,
Zukotynski K, Souza F, Wagner AJ and Ramaiya N: Imaging of
liposarcoma: classification, patterns of tumor recurrence, and
response to treatment. AJR Am J Roentgenol. 197:W37–W43. 2011.
View Article : Google Scholar
|
|
8
|
Kransdorf MJ, Bancroft LW, Peterson JJ, et
al: Imaging of fatty tumors: distinction of lipoma and
well-differentiated liposarcoma. Radiology. 224:99–104. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Secko M and Zehtabchi S: Complicated
diffuse lipomatosis mimicking ascites. Am J Emerg Med. 26:3792008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kraus MD, Guillou L and Fletcher CD:
Well-differentiated infl ammatory liposarcoma: an uncommon and
easily overlooked variant of a common sarcoma. Am J Surg Pathol.
21:518–527. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Murphey MD, Arcara LK and Fanburg-Smith J:
From the archives of the AFIP: imaging of musculoskeletal
liposarcoma with radiologic-pathologic correlation. Radiographics.
25:1371–1395. 2005. View Article : Google Scholar : PubMed/NCBI
|