Introduction
Ovarian metastasis secondary to gastric cancer
(Krukenberg tumor) has been extensively described in the literature
(1,2); however, gastric metastasis from
ovarian carcinoma has rarely been reported. An isolated parenchymal
gastric metastasis from ovarian carcinoma without any other sites
of recurrence is an extremely rare event, with only two cases
reported in China (3,4). Isolated gastric metastasis in the
absence of peritoneal seeding suggests hematogenous spread of the
tumor (3,5). The reports on this route of metastasis
are limited and the majority of these cases were diagnosed in
asymptomatic patients during follow-up by elevated serum
carbohydrate antigen (CA)-125 levels, or by images revealing the
presence of gastric tumors suggestive of gastrointestinal stromal
tumors (3,5–10). The
present report describes a case of an isolated gastric recurrence
from ovarian carcinoma in a 51-year-old asymptomatic patient. The
diagnosis was histologically confirmed following surgical
resection. Written informed consent was obtained from the
patient.
Case report
In April, 2012, a 51-year-old female presented to
the Department of Gynecology of the First Affiliated Hospital of
Nanjing Medical University (Nanjing, China) complaining of lower
abdominal pain of two months in duration. A computed tomography
(CT) scan of the abdomen and pelvis showed bilateral adnexal
complex masses. The patient subsequently underwent a total
abdominal hysterectomy, bilateral salpingo-oophorectomy with pelvic
lymph node dissection and omentectomy for stage III ovarian
adenocarcinoma (International Federation of Gynecology and
Obstetrics). The surgery was followed by four cycles of adjuvant
chemotherapy with paclitaxel and cisplatin. The patient was in good
condition and achieved complete clinical response in June, 2012. In
December, 2013, the patient was admitted to the Department of
Oncology, First Affiliated Hospital of Nanjing Medical University
due to significantly elevated serum CA-125 levels (up to 96.05
U/ml; normal, <35 U/ml), which is an important tumor marker.
Other tumor markers were within the normal range. The patient had
no abdominal discomfort, hematemesis, melena, weight loss or any
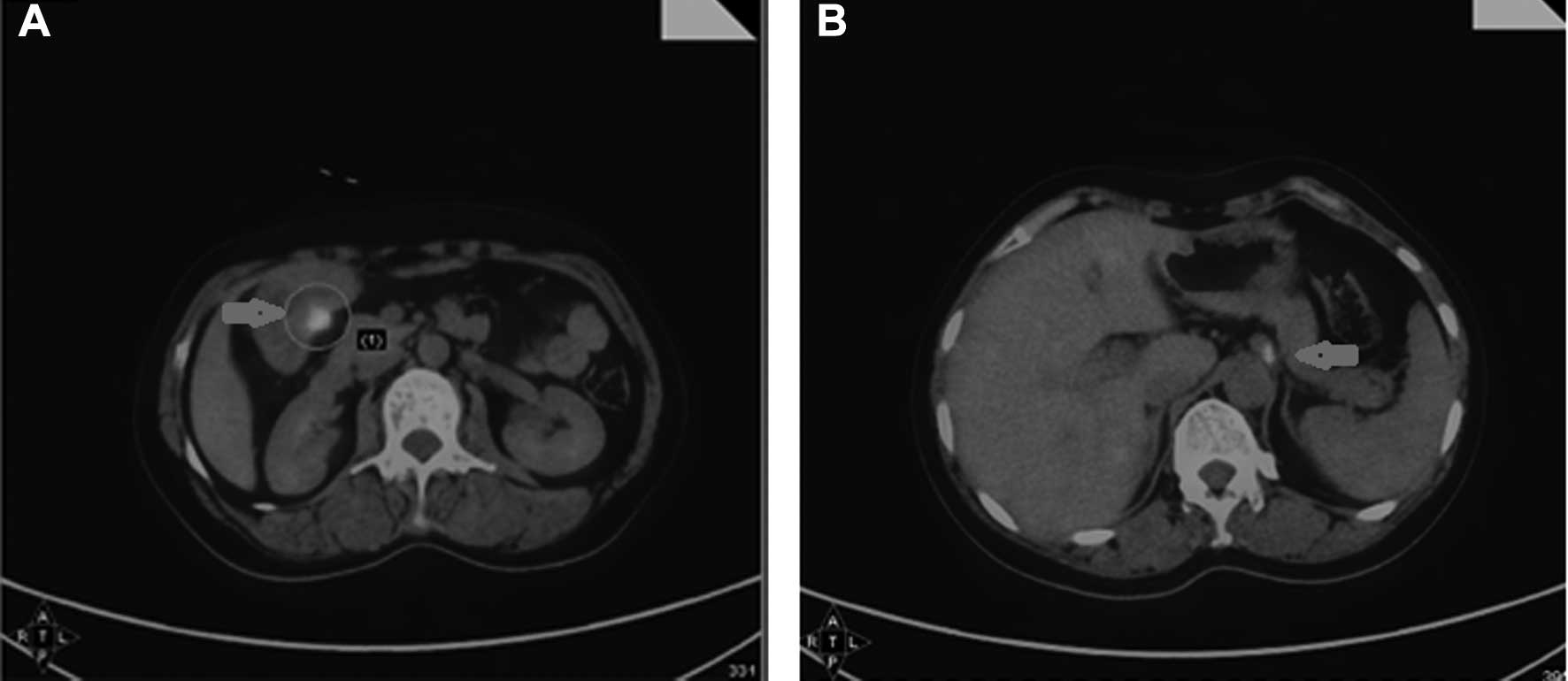
other clinical manifestations. Scanning with
18F-fluorodeoxyglucose positron emission
tomography(18F-FDG PET)/CT ruled out recurrent ovarian
carcinoma, which was suspected due to the high CA-125 levels. The
18F-FDG PET/CT images revealed a high-uptake lesion in
the antrum of the stomach (Fig. 1A)
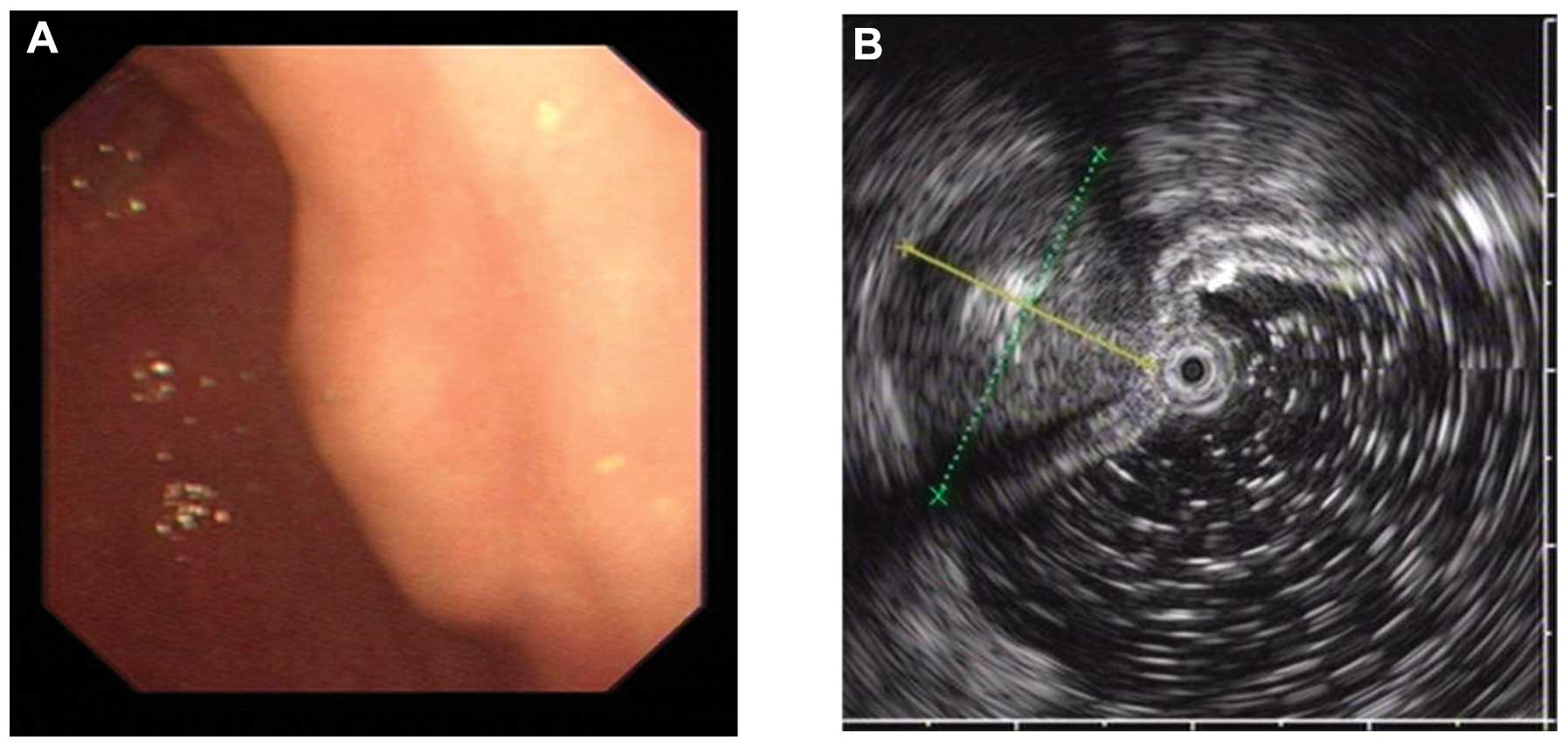
and a high-uptake lymph node behind the pancreas (Fig. 1B). During the subsequent endoscopic
examination, a 1.5×2.0-cm submucosal mass covered with normal
gastric mucosa was identified in the gastric antrum (Fig. 2A). Due to the location of the
lesion, the patient was referred for endoscopic ultrasound
examination, which revealed a hypoechoic mass emanating from the
muscularis propria, with the typical appearance of a
gastrointestinal stromal tumor (Fig.
2B). The patient subsequently underwent surgical resection of
the gastric lesion and the intumescent lymph nodes. The
intraoperative findings included a 2.5×2×2-cm isolated extrinsic
mass on the wall of the gastric antrum and a 1.0×0.8-cm intumescent
lymph node close to the lesser curvature of the stomach. The
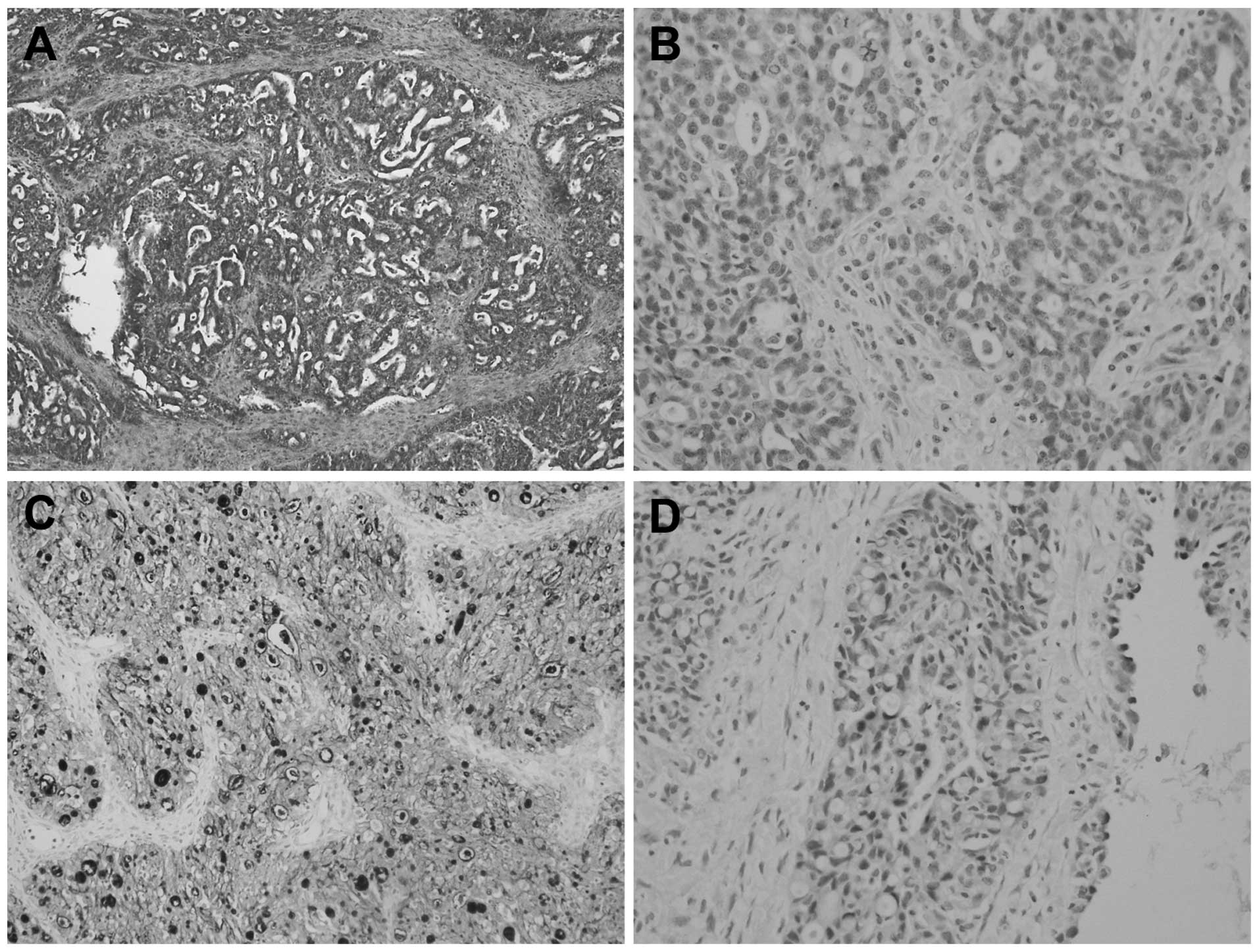
histopathological examination confirmed ovarian cancer relapse
involving the gastric wall without mucosal involvement, although a
lymph node was involved. Immunostaining for progesterone receptor,
estrogen receptor, cytokeratin 7 (CK7) and Wilms’ tumor-1 (WT1) was
positive; while immunostaining for CK20 was negative (Fig. 3). These findings were consistent
with the primary ovarian cancer (Fig.
4). The patient was discharged on the 10th day after surgery.
At the time of writing, the patient had received another two cycles
of adjuvant chemotherapy, and the CA-125 level had decreased to the
normal range.
Discussion
Gastric metastasis is a rare occurrence. A previous
study on 1,010 patients with malignant tumors reported 17 cases
(1.7%) of metastasis to the stomach (11). The most prevalent primary sites are
the lung, breast, skin (melanoma) and esophagus (12). Ovarian tumor metastasis to the
stomach is uncommon. To the best of our knowledge, only 10 reports
have been published to date (3–10,13,14).
The common metastatic sites throughout the abdominal cavity are the
intestinal omentum, mesentery and serosa (6). Another study including 50 patients
identified 67 distant metastatic sites: Liver, 21; pleura, 11;
lung, eight; central nervous system and skin, seven each;
extra-abdominal lymph nodes and spleen, five each; bone, two; and
breast, one (15). Although the
intraperitoneal route of dissemination is considered to be the most
common, ovarian cancer may also metastatize through the lymphatic
channels and the hematogenous route (16). We consider that the latter route may
account for the ovarian cancer metastasis in our case.
Immunohistochemistry is crucial for distinguishing
primary ovarian adenocarcinoma from metastatic adenocarcinomas,
particularly those of gastrointestinal origin (17). WT1 is expressed at a high frequency
in patients with epithelial ovarian cancer, and it is significant
in determining whether a serous carcinoma is primary or metastatic
(18). CK7 and CK20 are two of the
most commonly used tumor-detecting diagnostic tools in surgical
pathology. CK7 shows diffuse and strong staining in all serous
ovarian tumors, but the majority of metastatic gastrointestinal
carcinomas are negative for CK7 (19). CK20 has been found to be negative in
almost all ovarian tumors (20).
When attempting to differentiate between primary gastric cancer and
metastasis from ovarian cancer, it should be noted that a
monoclonal antibody panel for WT1, CK7 and CK20 may facilitate this
discrimination.
Recurrent ovarian carcinoma remains a therapeutic
issue for physicians. To date, there is no consensus regarding
optimal treatment strategies. Secondary cytoreductive surgery may
be considered for patients who present with recurrence after a long
disease-free period (≥6 months) (21). A recent meta-analysis suggested that
patients with recurrent disease who undergo complete cytoreduction
achieve prolonged survival (22).
The clinical manifestations of gastric metastasis
from ovarian carcinoma are diverse and non-specific. Including the
present case, five cases were asymptomatic (3,4,7,8),
one presented with epigastric pain and fullness (6), three presented with gastrointestinal
hemorrhage (9,10,13),
and one presented with belching and reflux (5). Therefore, when a patient has a history
of ovarian carcinoma, particularly with high CA-125 levels, and the
imaging results reveal a mass in the gastric wall, metastasis from
ovarian carcinoma should be considered. Imaging with
18F-FDG PET/CT and endoscopic ultrasound may be useful
for correctly diagnosing gastric lesions and should be considered
in all cases if available.
Although metastasis of ovarian tumor to the stomach
is rare, clinicians should consider that, in patients with a
history of ovarian cancer, gastric lesions may be secondary
metastases from ovarian cancer.
References
|
1
|
Kiyokawa T, Young RH and Scully RE:
Krukenberg tumors of the ovary: a clinicopathologic analysis of 120
cases with emphasis on their variable pathologic manifestations. Am
J Surg Pathol. 30:277–299. 2006.PubMed/NCBI
|
|
2
|
Al-Agha OM and Nicastri AD: An in-depth
look at Krukenbergtumor: an overview. Arch Pathol Lab Med.
130:1725–1730. 2006.PubMed/NCBI
|
|
3
|
Zhou JJ and Miao XY: Gastric metastasis
from ovarian carcinoma: A case report and literature review. World
J Gastroenterol. 18:6341–6344. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Xia BR and Yang Y: Ovarian carcinoma
metastasis to the parenchyma of the stomach at the time of
diagnosis: a case report and literature review. J Pract Oncol.
27:239–241. 2013.(In Chinese).
|
|
5
|
Obeidat F, Mismar A, Shomaf M, Yousef M
and Fram K: Gastric perforation secondary to metastasis from
ovarian cancer: Case report. Int J Surg Case Rep. 4:541–543. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kang WD, Kim CH, Cho MK, et al: Primary
epithelial ovarian carcinoma with gastric metastasis mimic
gastrointestinal stromal tumor. Cancer Res Treat. 40:93–96. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pernice M, Manci N, Marchetti C, Morano G,
Boni T, Bellati F and Panici PB: Solitary gastric recurrence from
ovarian carcinoma: a case report and literature review. Surg Oncol.
15:267–270. 2006. View Article : Google Scholar
|
|
8
|
Jung HJ, Lee HY, Kim BW, et al: Gastric
metastasis from ovarian adenocarcinoma presenting as a submucosal
tumor without ulceration. Gut Liver. 3:211–214. 2009. View Article : Google Scholar
|
|
9
|
Wallace W, Mulholland K and Epanomeritakis
E: Bleeding gastric varices - a rare complication of ovarian
cancer. Int J Clin Pract. 59:119–120. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sangha S, Gergeos F, Freter R, Paiva LL
and Jacobson BC: Diagnosis of ovarian cancer metastatic to the
stomach by EUS-guided FNA. Gastrointest Endosc. 58:933–935. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Menuck LS and Amberg JR: Metastatic
disease involving the stomach. Am J Dig Dis. 20:903–913. 1975.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Campoli PM, Ejima FH, Cardoso DM, et al:
Metastatic cancer to the stomach. Gastric Cancer. 9:19–25. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Akce M, Bihlmeyer S and Catanzaro A:
Multiple gastric metastases from ovarian carcinoma diagnosed by
endoscopic ultrasound with fine needle aspiration. Case Rep
Gastrointest Med. 2012:6105272012.PubMed/NCBI
|
|
14
|
Taylor RR, Phillips WS, O’Connor DM and
Harrison CR: Unusual intramural gastric metastasis of recurrent
epithelial ovarian carcinoma. Gynecol Oncol. 55:152–155. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Cormio G, Rossi C, Cazzolla A, Resta L,
Loverro G, Greco P and Selvaggi L: Distant metastases in ovarian
carcinoma. Int J Gynecol Cancer. 13:125–129. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ansell SM, Rapoport BL, Falkson G, Raats
JI and Moeken CM: Survival determinants in patients with advanced
ovarian cancer. Gynecol Oncol. 50:215–220. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kriplani D and Patel MM:
Immunohistochemistry: A diagnostic aid in differentiating primary
epithelial ovarian tumors and tumors metastatic to the ovary. South
Asian J Cancer. 2:254–258. 2013. View Article : Google Scholar
|
|
18
|
Hylander B, Repasky E, Shrikant P,
Intengan M, Beck A, Driscoll D, et al: Expression of Wilms tumor
gene (WT1) in epithelial ovarian cancer. Gynecol Oncol. 101:12–17.
2006. View Article : Google Scholar
|
|
19
|
Berezowski K, Stastny JF and Kornstein MJ:
Cytokeratins 7 and 20 and carcinoembryonic antigen in ovarian and
colonic carcinoma. Mod Pathol. 9:426–429. 1996.PubMed/NCBI
|
|
20
|
Wauters CC, Smedts F, Gerrits LG, Bosman
FT and Ramaekers FC: Keratins 7 and 20 as diagnostic markers of
carcinomas metastatic to the ovary. Hum Pathol. 26:852–855. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Eisenkop SM, Friedman RL and Spirtos NM:
The role of secondary cytoreductive surgery in the treatment of
patients with recurrent epithelial ovarian carcinoma. Cancer.
88:144–153. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Bristow RE, Puri I and Chi DS:
Cytoreductive surgery for recurrent ovarian cancer: a
meta-analysis. Gynecol Oncol. 112:265–274. 2009. View Article : Google Scholar
|