Introduction
Acute appendicitis is the most common abdominal
emergency encountered by the general surgeon (1). Subsequent to diagnosis by
histopathological examination, primary neoplasms of the appendix
are identified in ~0.5% of all surgically-removed appendices, with
carcinoid tumors representing >50% of all appendix neoplasms
(2,3).
Carcinoid tumors arise from the neuroendocrine cells of the diffuse
neuroendocrine system, which are identified in numerous locations,
including the lung (25.1%), ovaries (0.5%), biliary system (0.2%)
and throughout the gastrointestinal tract (73.4%) (4). Appendiceal carcinoid tumors are rare
neuroendocrine neoplasms that usually behave as benign tumors,
while certain lesions possess the potential for malignancy and are
therefore able to metastasize (5).
The probability of metastasis of appendiceal carcinoid tumors is
low, ~4.7% of all appendiceal carcinoid tumors (6). Lymphatic spread is the primary route,
and hepatic metastases are rare (2).
Although not a common occurrence, primary carcinoid tumors of the
appendix should be considered as a cause of acute appendicitis
during appendectomy. Surgical resection is recommended for the
treatment of appendiceal carcinoid tumors, and the long-term
prognosis of patients with appendiceal carcinoids is good (6). The present study reports the case of a
22-year-old female patient diagnosed with a carcinoid tumor located
at the tip of the appendix. Written informed consent was obtained
from the patient.
Case report
A 22-year-old female patient was admitted to Taicang
Hospital Affiliated to Soochow University (Taicang, Suzhou, China)
with the complaint of recurrent right lower abdominal pain of a
three-year duration, and an additional exacerbated attack of pain
that had lasted for the three days prior to presentation.
The patient reported a three-year history of
recurrent dull right lower abdominal pain that had not been
considered serious enough to obtain medical assistance. Three days
prior to admittance, the aforementioned symptoms became aggravated
and the patient presented to the Taicang Hospital Affiliated to
Soochow University. Physical examination revealed a body
temperature of 36.5°C, blood pressure of 111/78 mmHg and a pulse
rate of 95 beats/min. During assessment, the patient experienced
light direct tenderness, but no rebound tenderness, in the right
lower abdomen. No palpable masses were observed in the abdomen.
Laboratory tests were performed, yielding the following results:
White blood cell count, 4.4×109 cells/l (normal range,
4–10×109 cells/l); neutrophil proportion, 46.8% (normal
range, 45–80%); hemoglobin level, 130 g/l (normal range, 110–150
g/l); platelet count, 177×109 platelets/l (normal range,
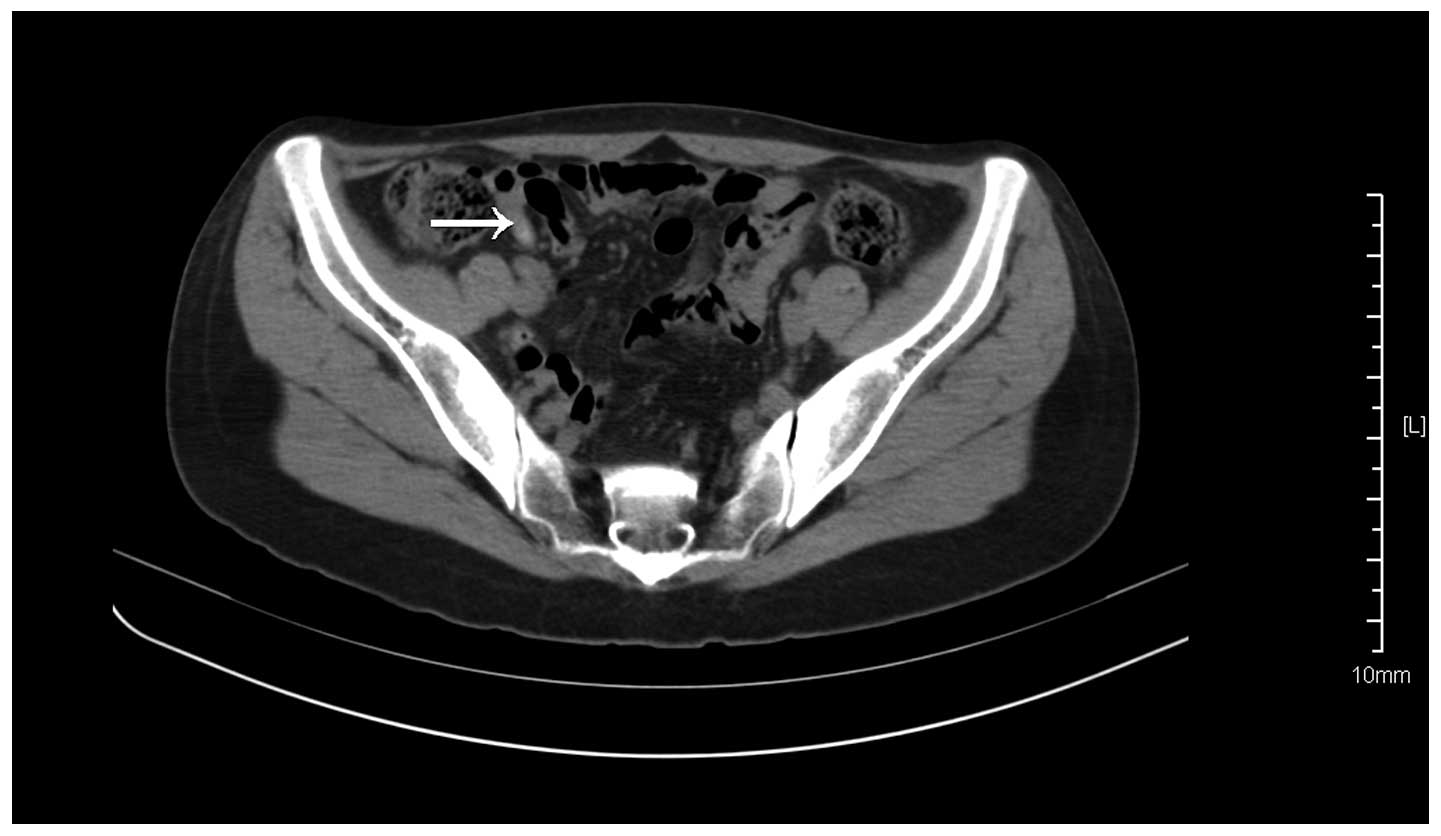
100–300×109 platelets/l). In addition, abdominal
computed tomography revealed appendiceal inflammation, while the
tumor was too small to identify (Fig.
1). The patient possessed no previous medical history and no
family medical history of appendicitis.
The patient underwent surgery for the treatment of
the acute attack of chronic appendicitis. The appendix was
identified as 7 cm long and 0.8 cm in diameter, demonstrating
hyperemia and edema. The resection of the appendix was completed
without complications and the patient recovered four days later.
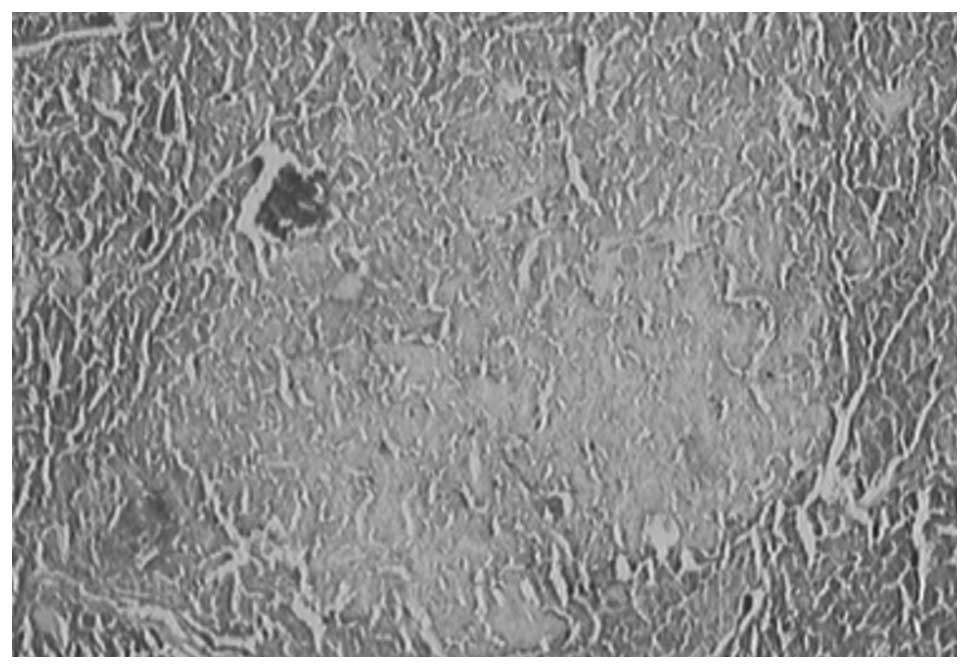
The specimen was examined by physiological analysis and stained
using hematoxylin and eosin. At the tip of the appendix, there was
a well-differentiated grade I neuroendocrine tumor (Fig. 2), measuring 5 mm at the maximum
dimension, that had infiltrated few regions of the muscular layer.
The mitotic activity of the lesion was not notable. Assessment of
the Ki-67 proliferative index revealed nuclear staining in ~1% of
cells. The diagnosis of appendiceal carcinoid tumor was confirmed
by positive immunostaining for the neuroendocrine markers
chromogranin A and synaptophysin. Coexisting acute purulent
appendicitis was also present. No further treatment was
administered. Follow-up examination one year after surgery revealed
that the patient was well, with no discomfort.
Discussion
Carcinoid tumors of the appendix are relatively
uncommon neoplasms. It has been previously reported that the
incidence of appendiceal carcinoids ranges between 0.3 and 0.9%, as
determined using histopathological examination performed on excised
appendectomy specimens (7,8). However, appendiceal carcinoids are the
most frequent tumors arising from the appendix, comprising between
32 and 57% of all appendiceal tumors (9). Carcinoid tumors are neoplasms derived
from the subepithelial neuroendocrine cells of the appendix
(10) that rarely cause metastatic
disease.
There is no specific pre-operative clinical
presentation for appendiceal carcinoids. In general, appendiceal
carcinoids are either asymptomatic or present as acute
appendicitis, which is then diagnosed incidentally as appendiceal
carcinoids during surgery (11). In
addition, the carcinoids can result in recurrent episodes of
abdominal pain due to partial obstruction of the appendiceal lumen
by a tumor. The presence of neuroendocrine symptoms, including
flushing, diarrhea and cardiac disease, are rarely reported
(12). In the case of the present
patient, the tumor was located at the tip of the appendix, and the
patient experienced recurrent right lower abdominal pain that had
been present for three years. The surgical procedure was performed
for the treatment of appendicitis, and the carcinoid tumor was
identified incidentally during the histological examination of the
excised surgical specimen.
Appendiceal carcinoids grow slowly, and the overall
prognosis is excellent (13). At
present, tumor size is the most reliable indicator for the
assessment of the malignant potential of lesions. In the majority
of patients with appendiceal carcinoids, the tumor diameter is
<1 cm and appendectomy alone is a sufficient treatment as
carcinoids rarely metastasize. However, tumors measuring ≥2 cm in
diameter may possess the potential for metastasis, and patients
with tumors of this size require right hemicolectomy. For tumors
measuring 1–2 cm in diameter, the surgical options depend on
mesoappendiceal involvement and the histological subtype of the
lesion. Suitable candidates for right hemicolectomy include lesions
where there is histological evidence of mesoappendiceal extension,
tumors that are located at the base of the appendix with positive
margins or involvement of the caecum, and high-grade malignant
carcinoids (14,15). In the present patient, the tumor was
0.5 cm in diameter and therefore appendectomy alone was
performed.
Post-operative follow-up was recommended by the
National Comprehensive Cancer Network 2013 Guidelines following the
excision of appendiceal carcinoids in for patients with tumors that
are >2 cm in diameter. This follow-up procedure comprises a
history and physical examination every 3–12 months post-resection
and every 6–12 months thereafter for ≤10 years, with consideration
of follow-up imaging or laboratory markers, such as
5-hydroxyindoleacetic acid or chromogranin A (16).
Overall, the long-term prognosis of appendiceal
carcinoids is extremely good. Sandor and Modlin evaluated 1570
carcinoid tumors of the appendix that were treated at the American
National Cancer Institute between 1973 and 1991. It was reported
that the five-year survival rates of patients with localized,
regional metastases and distant metastases in appendiceal
carcinoids were 94.0, 84.6 and 33.7%, respectively, and the overall
five-year survival rate was 85.9% (9). Another study with a large cohort
performed by Modlin et al reported that patients with local
disease demonstrate a five-year survival rate of 92%, those with
regional metastases demonstrated a five-year survival rate of 81%
and the few with distant metastases demonstrated a five-year
survival rate of 31% (10).
Carcinoid tumors are the most common neoplasms of
the appendix, but demonstrate no specific clinical presentation.
The presence of these tumors should be considered, particularly
during surgical procedures.
References
|
1
|
Ruffolo C, Fiorot A, Pagura G, Antoniutti
M, Massani M, Caratozzolo E, Bonariol L, Calia di Pinto F and Bassi
N: Acute appendicitis: what is the gold standard of treatment?
World J Gastroenterol. 19:8799–8807. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Deans GT and Spence RA: Neoplastic lesions
of the appendix. Br J Surg. 82:299–306. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pickhardt PJ, Levy AD, Rohrmann CA Jr and
Kende AI: Primary neoplasms of the appendix manifesting as acute
appendicitis: CT findings with pathologic comparison. Radiology.
224:775–781. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Modlin IM and Sandor A: An analysis of
8305 cases of carcinoid tumors. Cancer. 79:813–829. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Parkes SE, Muir KR, al Sheyyab M II,
Cameron AH, Pincott JR, Raafat F and Mann JR: Carcinoid tumours of
the appendix in children 1957–1986: Incidence, treatment and
outcome. Br J Surg. 80:502–504. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Moertel CG, Weiland LH, Nagorney DM and
Dockerty MB: Carcinoid tumor of the appendix: treatment and
prognosis. N Eng J Med. 317:1699–1701. 1987. View Article : Google Scholar
|
|
7
|
Moertel CG, Dockerty MB and Judd ES:
Carcinoid tumors of the vermiform appendix. Cancer. 21:270–278.
1968. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Connor SJ, Hanna GB and Frizelle FA:
Appendiceal tumors: Retrospective clinicopathologic analysis of
appendiceal tumors from 7,970 appendectomies. Dis Colon Rectum.
41:75–80. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sandor A and Modlin IM: A retrospective
analysis of 1570 appendiceal carcinoids. Am J Gastroenterol.
93:422–428. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Modlin IM, Lye KD and Kidd M: A 5-decade
analysis of 13,715 carcinoid tumors. Cancer. 97:934–959. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Roggo A, Wood WC and Ottinger LW:
Carcinoid tumors of the appendix. Ann Surg. 217:385–390. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Markgraf WH and Dunn TM: Appendiceal
carcinoid with carcinoid syndrome. Am J Surg. 107:730–732. 1964.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Thirlby RC, Kasper CS and Jones RC:
Metastatic carcinoid tumor of the appendix. Report of a case and
review of the literature. Dis Colon Rectum. 27:42–46. 1984.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Syracuse DC, Perzin KH, Price JB, Wiedel
PD and Mesa-Tejada R: Carcinoid tumors of the appendix.
Mesoappendiceal extension and nodal metastases. Ann Surg.
190:58–63. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gouzi JL, Laigneau P, Delalande JP,
Flamant Y, Bloom E, Oberlin P and Fingerhut A: The French
Associations for Surgical Research: Indications for right
hemicolectomy in carcinoid tumors of the appendix. Surg Gynecol
Obstet. 176:543–547. 1993.PubMed/NCBI
|
|
16
|
National Comprehensive Cancer Network
(NCCN), . NCCN Clinical Practice Guidelines v2.2013. Neuroendocrine
tumors. http://www.nccn.org/professionals/physician_gls/pdf/neuroendocrine.pdfAccessed.
May 15–2013
|