Introduction
Renal cell carcinoma (RCC) accounts for 3% of all
adult malignancies and 85% of all primary renal tumors; RCC is the
third most common type of urological cancer, after prostate and
bladder cancer (1). Currently, the
incidence of RCC is rising, due to the increased number of
incidental findings by imaging tests. In 2013, it was estimated
that there will be 65,150 new cases of kidney and renal pelvis
cancers and 13,680 cancer-related mortalities in the United States
(2). It has been reported that the
five-year cancer-related survival rate was 90.4% for patients with
localized disease, 62.3% for patients with regional lymph nodes
metastasis, 10.4% for patients with distal metastasis (3). Of the newly diagnosed cases of RCC,
~25–50% will develop metastatic disease subsequent to surgical
resection of the primary renal mass (4). RCC frequently metastasizes to distal
organs, such as lungs, abdomen, bones and brain. Contralateral
adrenal gland and urinary bladder metastasis are rare, and have
been previously described case reports (5,6). To the
best of our knowledge, RCC with metachronous metastasis to the
contralateral adrenal and bladder has not been reported. For
treatment of metastatic renal cell carcinoma, complete resection of
metastases or not remains contraversial (7). Cancer-specific survival rates between
metastases resected and non-resected populations have previously
been reported and prolonged survival was observed with metastases
resection (8,9). In the present study, an unusual case of
clear cell-type RCC (ccRCC) with metachronous metastasis to the
contralateral adrenal gland and urinary bladder 5 years following
nephrectomy is reported.
Case report
A 55-year-old male was referred to the Department of
Urology of the Zhejiang Xiaoshan Hospital (Hangzhou, China) in
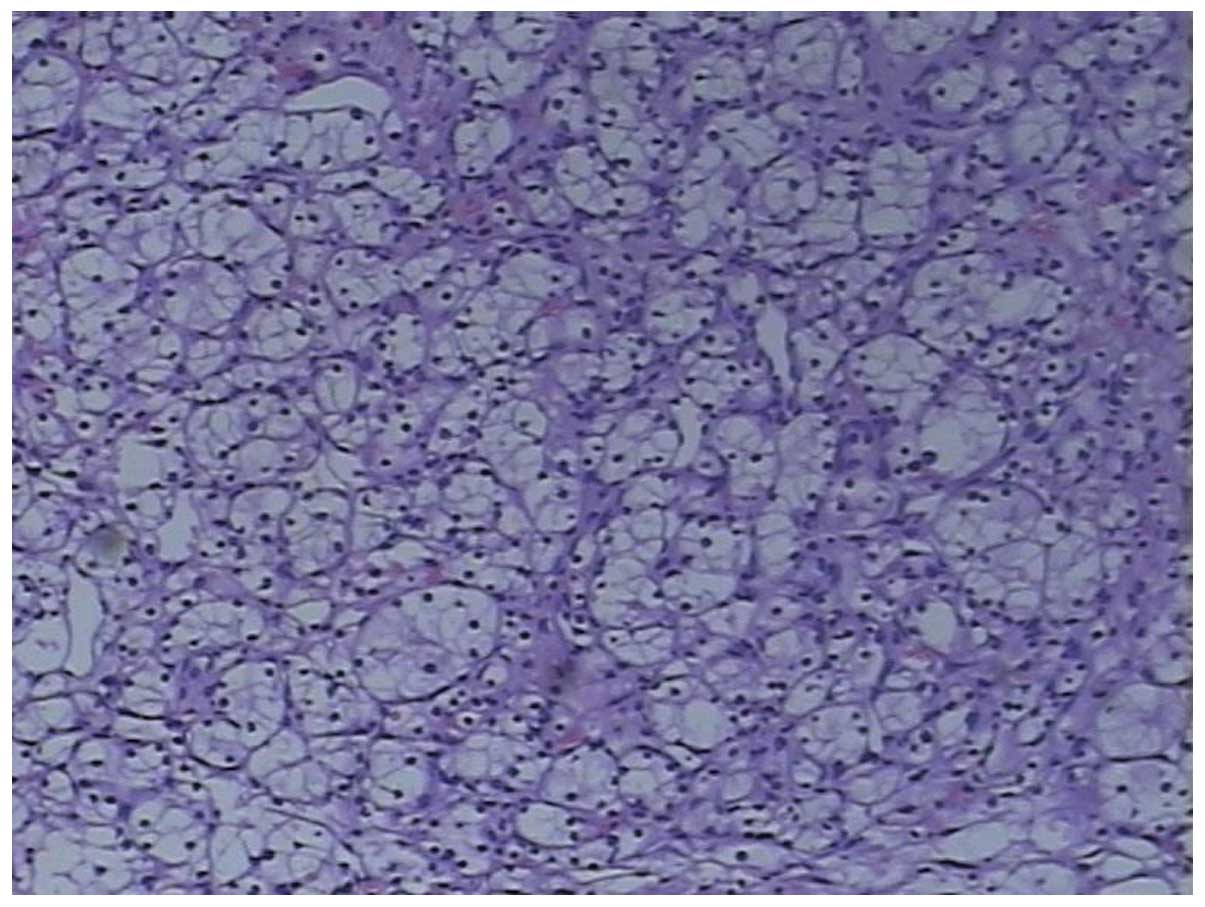
October 2005, exhibiting a case of left-kidney RCC. Radical
nephrectomy was performed (Fig. 1),
and the postoperative pathology findings confirmed cc-type and
pT1aN0M0, according to the
American Joint Committee on Cancer 2009 cancer staging (Fig. 2) (10).
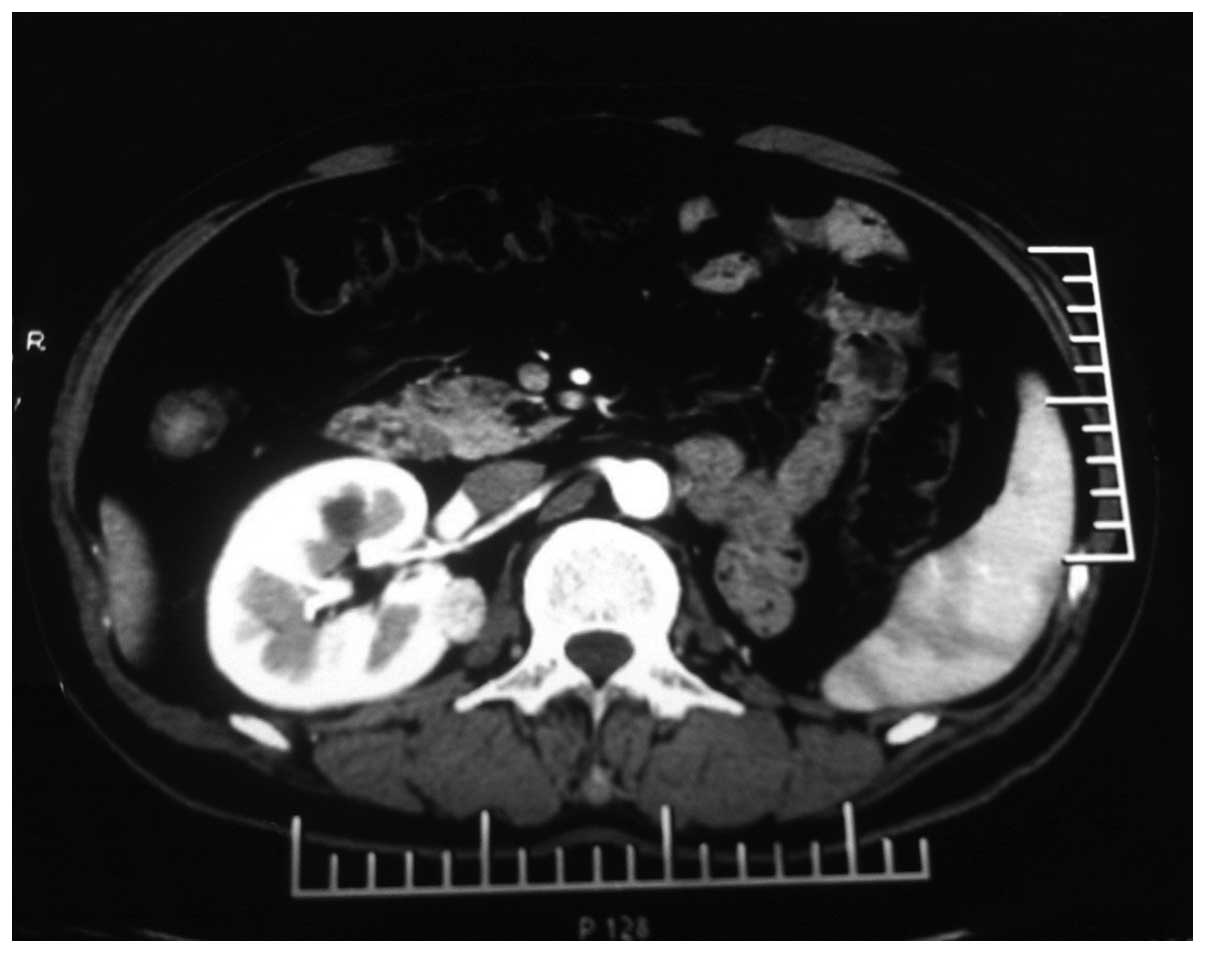
No recurrence was observed during the follow-up period until
November 2010, when upper abdominal computed tomography (CT)
revealed a 40×45-mm enhanced mass in the right adrenal gland
(Fig. 3). Subsequent laboratory tests
demonstrated the tumor to be hormonally inactive. In addition,
type-B ultrasound revealed a 1.0-cm solid space-occupying lesion in
the right wall of the bladder. Thoracic CT and bone scan did not
identify any other metastases.
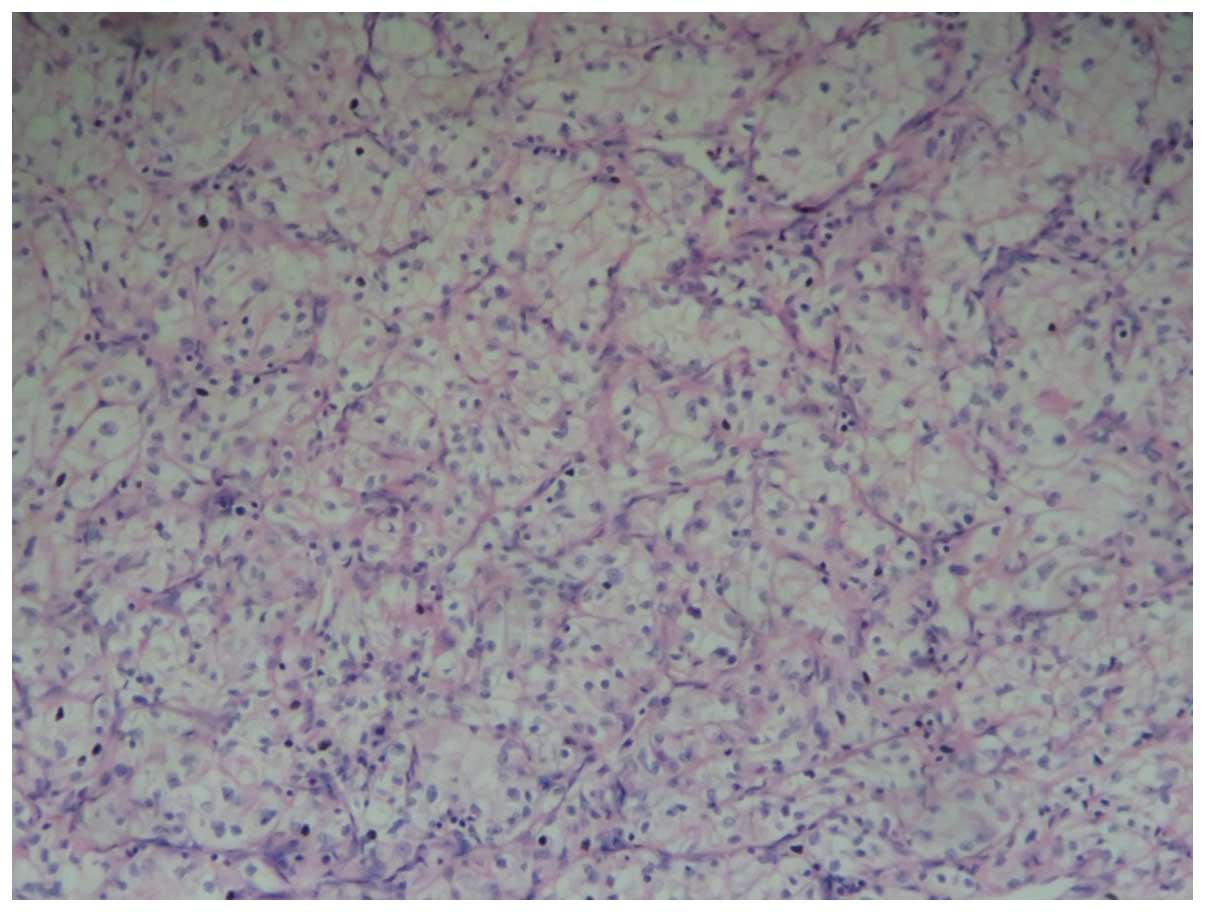
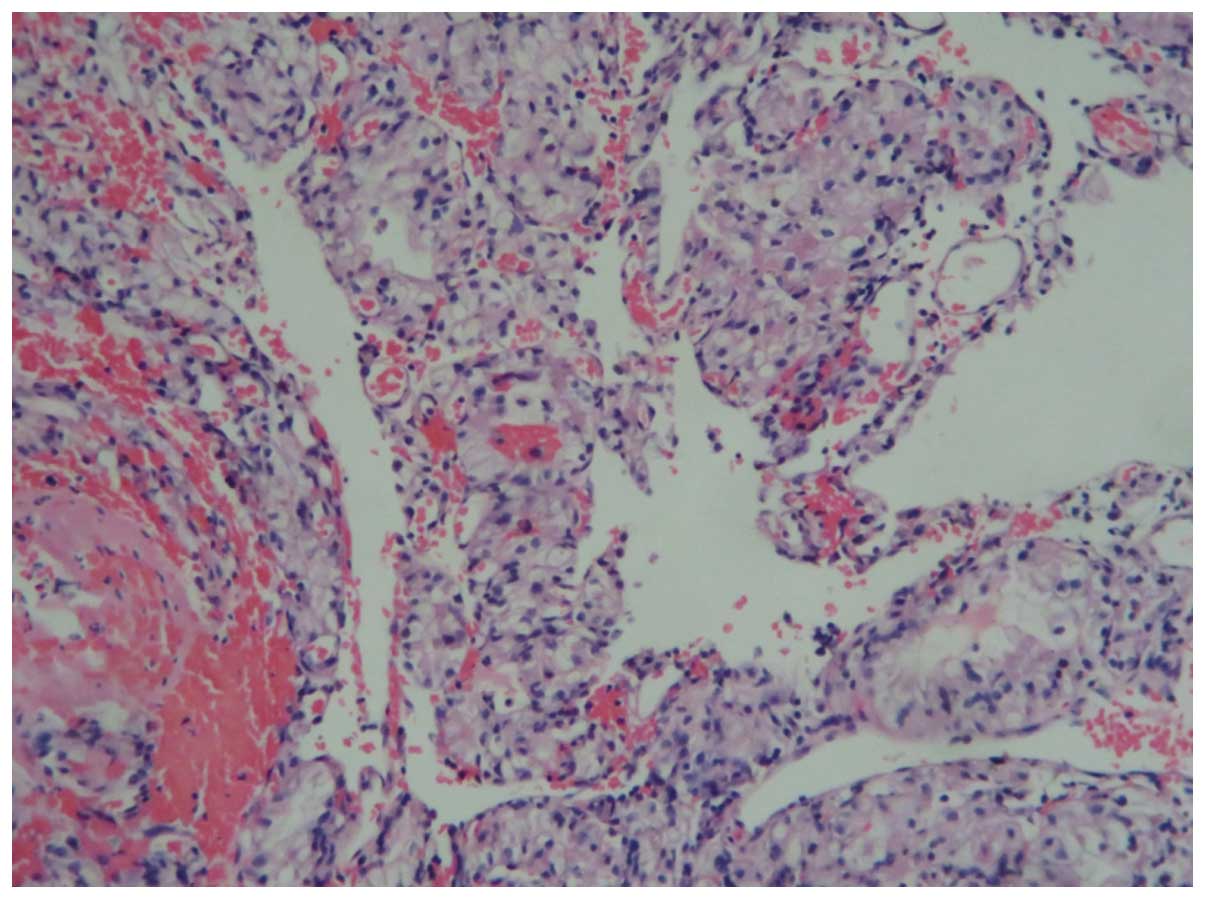
Following hospitalization, laparoscopic right
adrenalectomy and transurethral resection of the bladder tumor were
performed. Histopathological examination of the resected tissues
confirmed cc carcinoma, which was identical to that of the left
renal tumor previously experienced by the patient (Figs. 4–7). CT
and intravesical instillation chemotherapy were regularly reviewed
following surgery. However, 1 year later, CT scanning detected
multiple solid space-occupying lesions in the right kidney
(Fig. 8). Consequently, the patient
was treated with first-line sunitinib targeted therapy.
At present, the patient is generally in good
condition, without obvious drug side effects and discomfort
complaint.
Discussion
RCC possesses a propensity for distal metastasis,
which may occur in all organs, including the lung, lymph node,
liver and bone. However, RCC rarely metastasizes to the adrenal
gland and urinary bladder (4,11). In a previous study of >400 patients
who had undergone radical nephrectomy for RCC, isolated
contralateral adrenal gland metastases accounted for 2.5% of the
total cases (6,12). Additionally, Saitoh et al
(13) reported 1.6% of clinically
detectable bladder metastases in 1,451 autopsy cases of patients
with RCC (5,6,12,14). Nonetheless, ccRCC with metachronous
metastasis to the contralateral adrenal gland and urinary bladder
has not been reported thus far.
Contralateral adrenal gland metastasis is
hypothesized to develop through the hematogenous route. Dieckmann
et al (15) suggested that the
adrenal gland may act as ‘fertile soil’ and ‘raise’ the seeding
tumor cells from the contralateral primary RCC, since the adrenal
gland exhibits high affinity for metastases of RCC (15,16). The
mechanism by which RCC metastasizes to the urinary bladder remains
unclear, although it has been suggested to occur via the
hematogenous route, lymphatic system or urinary stream (5). The hematogenous metastasis pathway may
occur through the systemic circulation or through retrograde venous
dissemination, such as via the gonadal and ureteral vein, when the
renal vein is obstructed by cancer emboli (14). When a tumor invades the kidney pelvis,
or following diagnostic biopsy using an ureteroscope, it may
metastasize via the urinary stream (5). Additionally, direct extension and
seeding implantation have been proposed as potential mechanisms for
metastasis of RCC, since cancer cells have been detected in the
urine of patients with RCC (17).
Patients with distal metastases present a worse
prognosis than those without metastatic tumors, with a 5-year
survival rate of <10% (11),
although radical nephrectomy and resection of a single or limited
metastases may prolong the survival rate by 30% (6). Patients with metastatic RCC may benefit
from minimal invasive surgeries, such as laparoscopic and
endoscopic resection of metastatic neoplasms from RCC (6). However, depending on the tumor size and
the strength of the adhesion to the peripheral organs, minimal
invasive surgeries may not always be possible to perform. Surgical
treatments rarely present complications, and should be recommended
in all cases of RCC for a curative outcome (18). Despite the fact that the majority of
patients with RCC that had undergone surgery succumbed as a result
of RCC, their survival time was longer than those who had not
undergone surgical treatment (6).
In a randomized phase III trial, Motzer et al
(19) reported that the median
progression-free survival of patients treated with sunitinib was 11
months. In the present case, the patient experienced metastasis of
RCC to the contralateral kidney following resection of the adrenal
gland and urinary bladder tumor. Therefore, the patient was advised
to receive first-line sunitinib targeted therapy, which is known to
be an effective treatment for metastatic RCC (20). To date, the patient is generally in
good condition, without any evidence of drug side effects or
complaints of discomfort.
References
|
1
|
Choi JB, Yoon BI, Kim SJ, Cho HJ, Hong SH,
Choi YJ, Kim SW, Hwang TK and Lee JY: Changes in
clinicopathological characteristics of renal cell carcinoma in the
past 25 years: A single-center experience. Korean J Urol.
52:110–114. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Melegari S, Albo G, Rocco B, Verweij F,
Abbinante M and de Cobelli O: Metachronous bladder metastases from
renal cell carcinoma: A case report and review of the literature.
Ecancermedicalscience. 4:1752010.PubMed/NCBI
|
|
4
|
Chung PH, Srinivasan R, Linehan WM, Pinto
PA and Bratslavsky G: Renal cell carcinoma with metastases to the
gallbladder: Four cases from the National Cancer Institute (NCI)
and review of the literature. Urol Oncol. 30:476–481. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kagota M, Irie K, Hosaka K and Takezaki T:
Bladder metastasis of renal cell carcinoma; a case study. Hinyokika
Kiyo. 53:571–574. 2007.PubMed/NCBI
|
|
6
|
Lau WK, Zincke H, Lohse CM, Cheville JC,
Weaver AL and Blute ML: Contralateral adrenal metastasis of renal
cell carcinoma: Treatment, outcome and a review. BJU Int.
91:775–779. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Brinkmann OA, Semik M and Gosherger G: The
role of residual tumor resection in patients with metastatic renal
cell carcinoma and partial remission following immunotherapy. Eur
Urol. 6:641–645. 2007. View Article : Google Scholar
|
|
8
|
Alt AL, Bllrjian SA, Lohse CM, Costello
BA, Leibovich BC and Blute ML: Survival after complete surgical
resection of multiple metastases from renal cell carcinoma. Cancer.
117:2873–2882. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kwak C, Park YH, Jeong CW, Lee SE and Ku
JH: Metastasectomy without systemic therapy in metastatic renal
cell carcinoma: Comparison with conservative treatment. Urol Int.
79:145–151. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Martínez-Salamanca JI, Huang WC, Millán I,
Bertini R, Bianco FJ, Carballido JA, Ciancio G, Hernández C,
Herranz F, Haferkamp A, et al: International Renal Cell
Carcinoma-Venous Thrombus Consortium: Prognostic impact of the 2009
UICC/AJCC TNM staging system for renal cell carcinoma with venous
extension. Eur Urol. 59:120–127. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shoji S, Mukai M, Yazawa N, Sekido Y,
Nagata Y, Uchida T and Terachi T: Metastasis to gallbladder and
adrenal gland of renal cell carcinoma. Oncol Lett. 1:507–509. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Moslemi MK, Saghafi H and Firoozabadi MH:
Renal cell carcinoma with simultaneous bilateral adrenal
metastasis: Ipsilateral radical nephrectomy with contralateral
adrenal preservation. Case Rep Oncol. 3:372–379. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Saitoh H: Distant metastasis of renal cell
adenocarcinoma. Cancer. 48:1487–1491. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shiraishi K, Mohri J, Inoue R and Kamiryo
Y: Metastatic renal cell carcinoma to the bladder 12 years after
radical nephrectomy. Int J Urol. 10:453–455. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Dieckmann KP, Wullbrand A and Krolzig G:
Contralateral adrenal metastasis in renal cell cancer. Scand J Urol
Nephrol. 30:139–143. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sagalowsky AI, Kadesky KT, Ewalt DM and
Kennedy TJ: Factors influencing adrenal metastasis in renal cell
carcinoma. J Urol. 151:1181–1184. 1994.PubMed/NCBI
|
|
17
|
Joshi DP, Shah RB, Montie JE and Lee CT:
Isolated recurrent renal cell carcinoma metastatic to the bladder.
J Natl Med Assoc. 94:912–914. 2002.PubMed/NCBI
|
|
18
|
Utsumi T, Suzuki H, Nakamura K, Kim W,
Kamijima S, Awa Y, Araki K, Nihei N, Naya Y and Ichikawa T: Renal
cell carcinoma with a huge solitary metastasis to the contralateral
adrenal gland: A case report. Int J Urol. 15:1077–1079. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Motzer RJ, Hutson TE, Tomczak P,
Michaelson MD, Bukowski RM, Oudard S, Negrier S, Szczylik C, Pili
R, Bjarnason GA, et al: Overall survival and updated results for
sunitinib compared with interferon alfa in patients with metastatic
renal cell carcinoma. J Clin Oncol. 27:3584–3590. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Coppin C, Kollmannsberger C, Le L,
Porzsolt F and Wilt TJ: Targeted therapy for advanced renal cell
cancer (RCC): A Cochrane systematic review of published randomised
trials. BJU Int. 108:1556–1563. 2011. View Article : Google Scholar : PubMed/NCBI
|