Introduction
Submucosal tumors (SMTs) of the rectum are rare, and
account for 7–8% of all leiomyomas arising in the gastrointestinal
tract (1). In Japan, SMTs of the
rectum are particularly rare, accounting for ~1 in every
2,000–3,000 cases of SMTs (2,3). Although gastrointestinal leiomyoma is
commonly detected as a SMT, definitive preoperative diagnosis is
often difficult as the majority of SMTs do not cause symptoms and
are identified incidentally during endoscopic or radiological
examinations. The overlying mucosa typically appears smooth and
normal on endoscopy (4). Therefore,
the suggested diagnostic technique is immunohistochemical analysis
(5); leiomyomas typically exhibit
positivity for desmin and α-smooth muscle actin and negativity for
C-kit, CD4 and S-100. The standard surgical approaches for
anorectal SMTs include transanal, transcoccygeal, transsphincteric
or intersphincteric resection (ISR) for small tumors, and anterior
or abdominoperineal resection for large tumors (1). However, anterior and abdominoperineal
resection are associated with high mortality and morbidity
(5). Recently, laparoscopic surgery,
which is a minimally invasive technique, has been found to be
useful for the treatment of small rectal tumors. It is associated
with increased feasibility and safety with regard to the short term
outcome of patients when compared with the same type of open
surgery; for example, low anterior resection (6). The present study describes the case of a
patient with a rectal leiomyoma who was subjected to a transvaginal
resection to minimize the invasiveness of the surgery.
Case report
In February 2013, a 51-year-old female with no
subjective symptoms presented to the Department of Obstetrics and
Gynecology of Gifu University (Gifu, Japan) with a mass that was
detected during a health screening. In January 2013, the patient
underwent transvaginal ultrasonography at Mabuchi Ladies Hospital
(Gifu, Japan), which demonstrated a protrusion in the anterior
rectal wall with no mucosal abnormalities. The patient was then
referred to the Department of Obstetrics and Gynecology of Gifu
University in May 2013 for diagnosis and treatment
recommendations.
Computed tomography examination detected the
presence of a tumor of unclear origin that was ~45 mm in diameter,
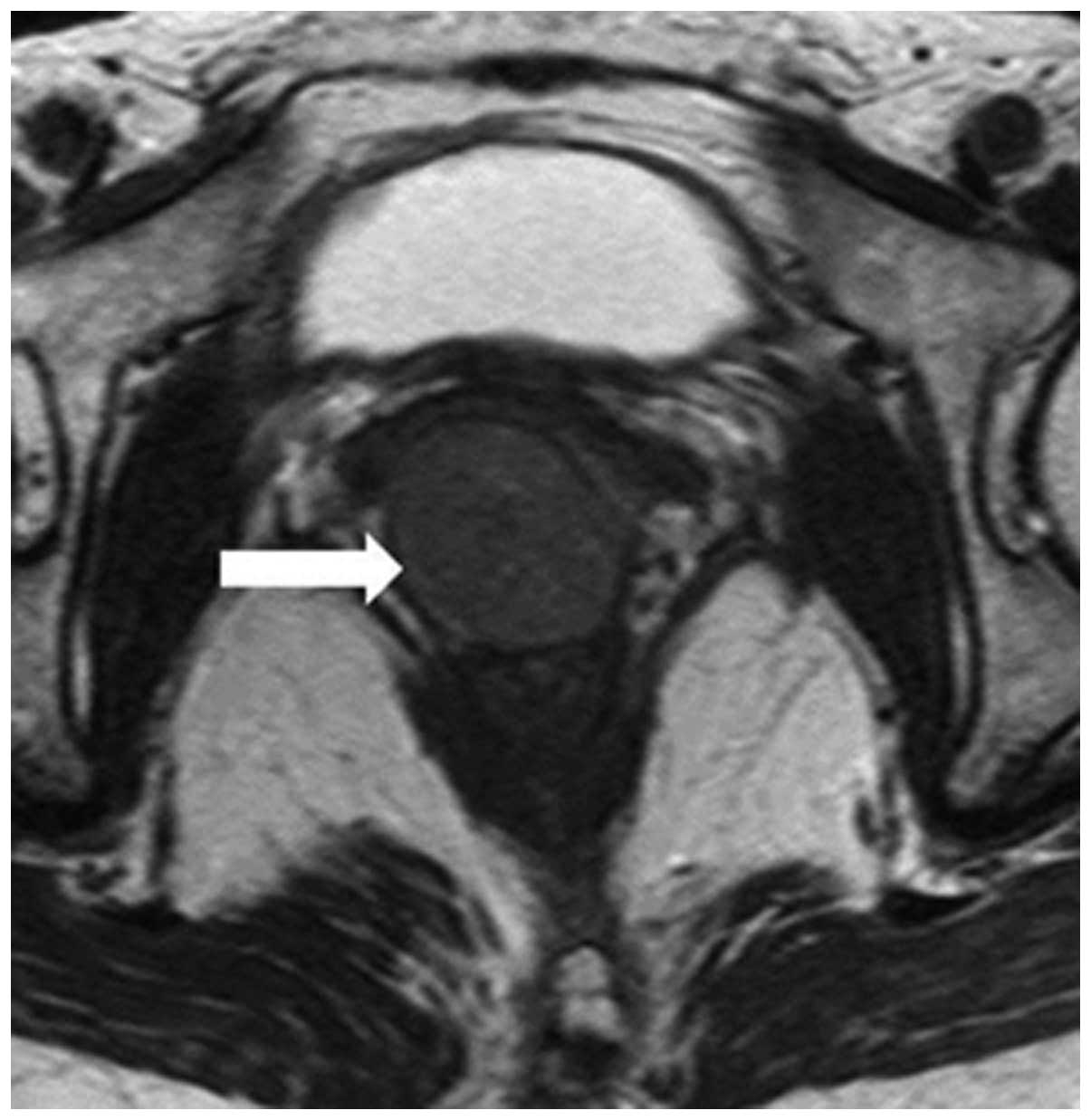
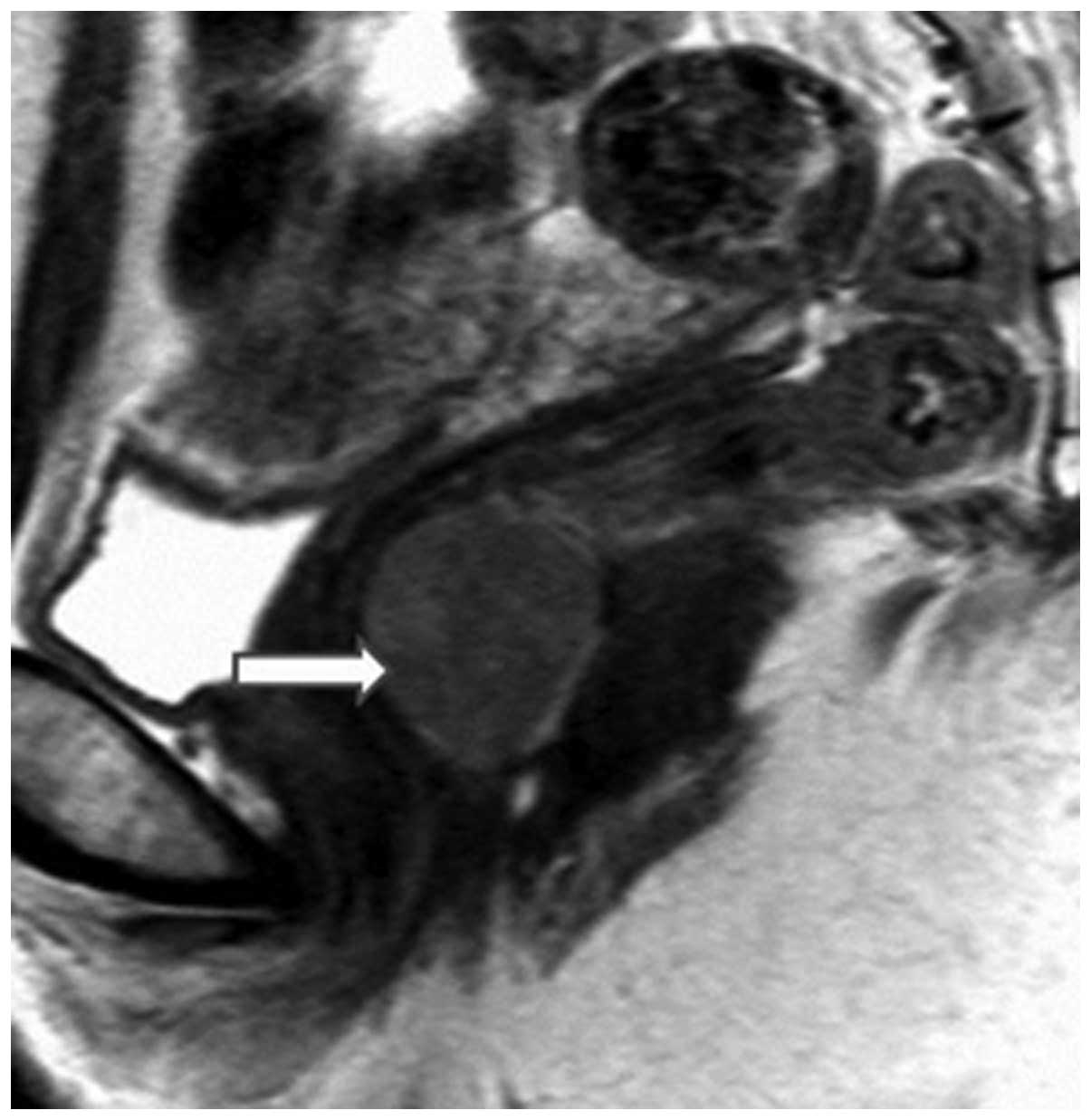
and located between the rectum and vagina (Fig. 1). Magnetic resonance imaging revealed
that the 45-mm tumor was encapsulated by the rectal muscle,
suggesting a rectal SMT, which was suspected to be a
gastrointestinal stromal tumor (GIST) (Figs. 2 and 3).
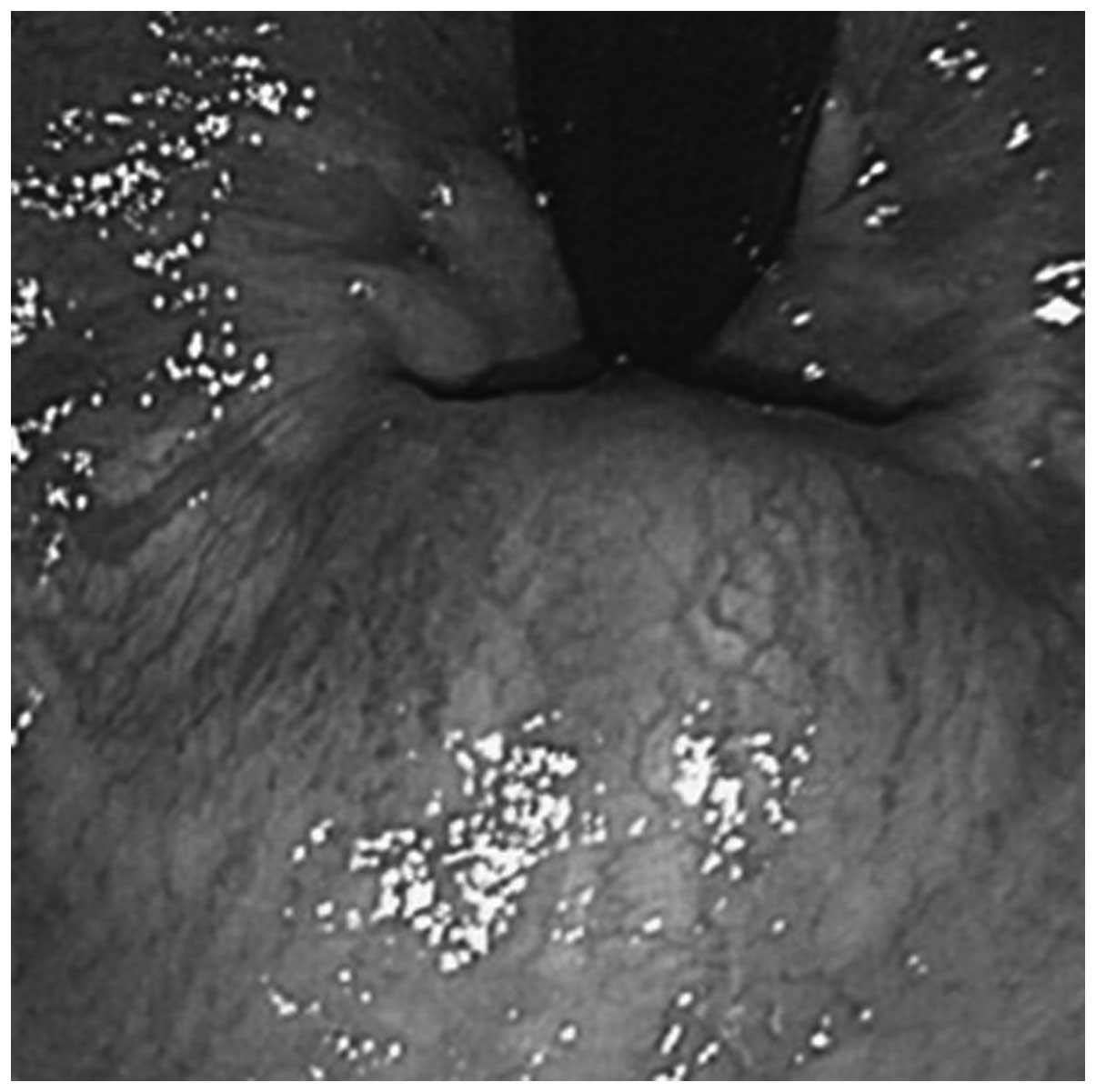
Colonoscopy examination identified a rectal SMT on the anterior
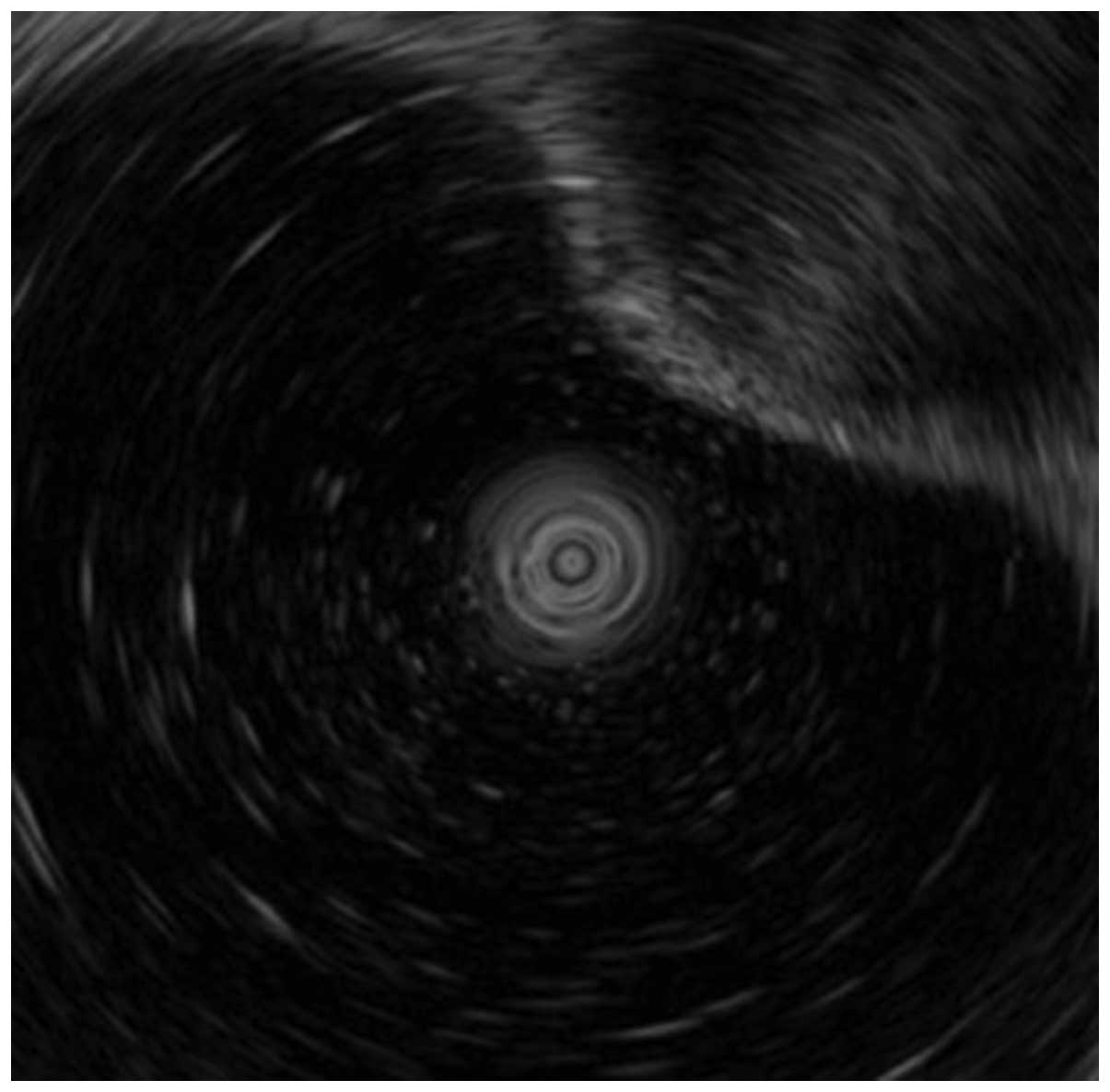
wall of the rectum, located 3 cm from the anal verge (Fig. 4). On endoscopic ultrasound
examination, the tumor appeared to originate from the third layer
of the rectum (Fig. 5). A tumor in
this region is traditionally approached with laparoscopic anterior
rectal resection or ISR, which was considered. However, these
approaches were not followed due to the risks associated with these
procedures in terms of invasiveness and potential anal
dysfunction.
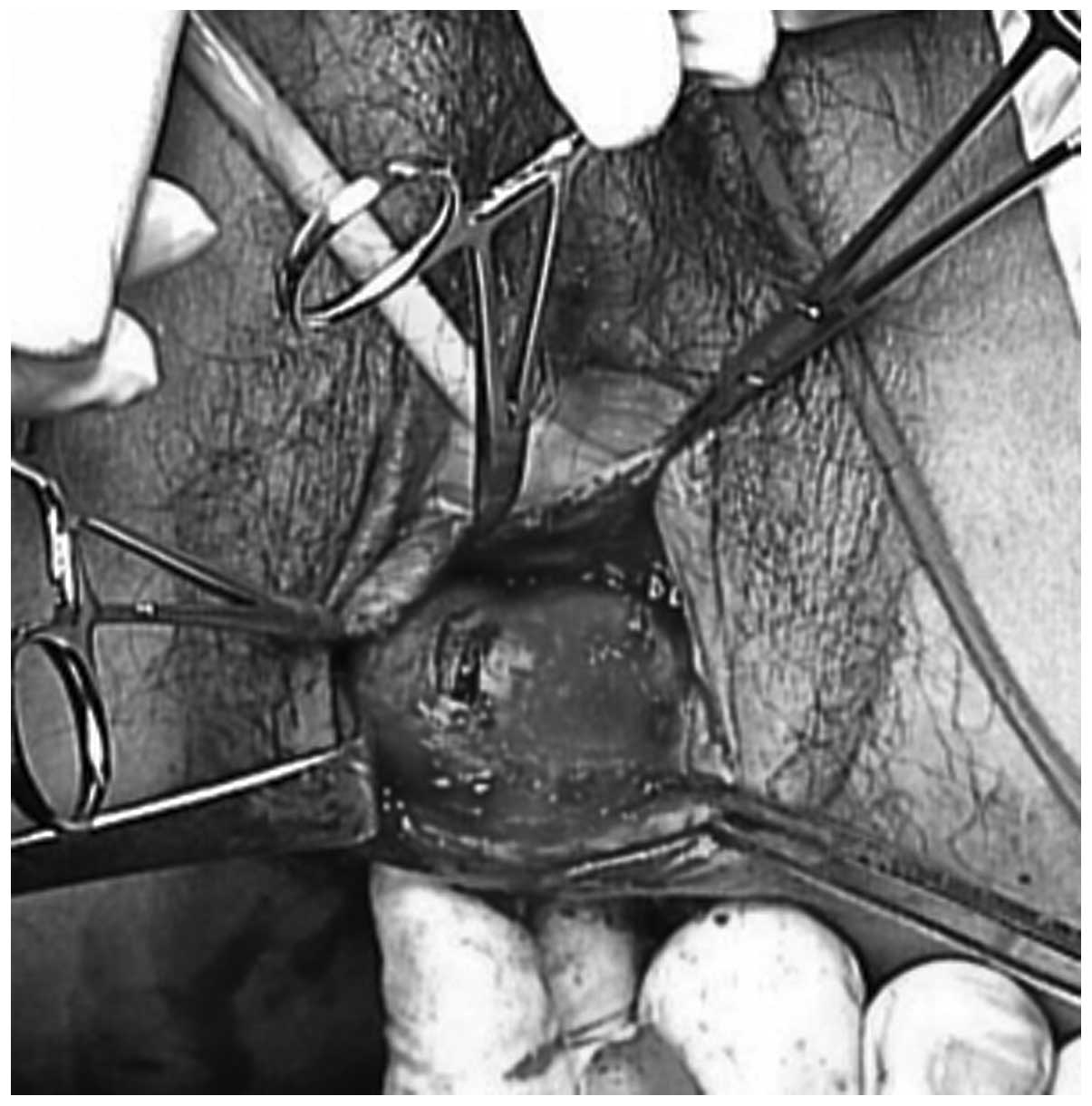
Therefore, the patient was subjected to general
anesthesia and placed in the lithotomy position. The vaginal mucosa
was then incised vertically, exposing the rectovaginal septum
overlying the tumor. The tumor was mobilized, and the capsule
surrounding the tumor was kept intact. To prevent the development
of potential complications, such as post-operative rectovaginal
fistulae, the rectal muscle and mucosa were sutured horizontally,
and the vaginal layers were closed vertically (Figs. 6–8). In
addition, a laparoscopic diverting ileostomy via 2 ports was
performed. The total surgical duration was 120 min, and the
estimated blood loss was 120 ml. Pathological examination of the
tumor confirmed the diagnosis of a leiomyoma with clear surgical
margins (Fig. 9). Since the recovery
of the patient did not present any complications, the patient was
discharged on day 10 post-surgery, and the diverting ileostomy was
closed 3 months later. Currently, the Department of Surgical
Oncology of Gifu University is using manometry to examine the
post-operative sphincter status of all the patients who underwent
ISR and ultra-low anterior resection at their premises. Fecal
incontinence in these post-operative patients is evaluated with
three-dimensional vector manometry to determine the median of the
maximum resting and squeeze pressures in the anal sphincter. In
addition, the modified Fecal Incontinence Quality of Life (mFIQL)
scale and Wexner score (7) are used
to assess the patients. The defecatory function is assessed in
terms of frequency of bowel movements and continence. The median
maximum resting pressure measured for the patient of the current
report was 25.0 mmHg (normal range, 50.3–92.2 mmHg), and the
maximum squeeze pressure was 118.6 mmHg (normal range, 100.3–240.8
mmHg). The mFIQL and Wexner scores of the patient at 3 months
following the closure of the stoma were each 0 points, indicating
the absence of fecal incontinence. Furthermore, thus far, the
patient has not experienced any anal dysfunction or discomfort
post-operatively. Written informed consent was obtained from the
patient for the publication of the present case report and any
accompanying images.
Discussion
Rectal surgery, and particularly surgery on the
lower rectum, is associated with more complications than other
surgical procedures performed on more proximal portions of the
gastrointestinal tract. These complications include anastomotic
leakage, bleeding, impaired anal sphincter function and fecal
incontinence. The resection of tumors of the rectum is difficult
and invasive due to the location of the rectum on the pelvic floor
(8). Surgical procedures on the lower
rectum normally require dissection down to the levator ani muscle,
which may result in anal dysfunction or discomfort (1). Therefore, a less invasive procedure is
desirable (9,10).
SMTs of the rectum are relatively rare, and include
GISTs, carcinoids, leiomyomas, leiomyosarcomas, malignant
lymphomas, neurinomas and lipomas. Sasaki et al (11) reported the recurrence of relapse in 5
out of 76 patients with SMTs, and Kusminsky and Bailey (12) reported a recurrence rate of 31% in
affected patients.
The main problem associated with a rectal leiomyoma
is the histological diagnosis, since the pathological image does
not usually correspond to the biological malignancy (11). In the present study, the diagnosis of
a suspected GIST was confirmed by endoscopic ultrasound
examination.
Although rectal GISTs and SMTs exhibit malignant
potential, patients with rectal GISTs present with equivalent
survival rates, regardless of whether a local or complete bowel
resection is performed (11). This is
possibly due to the preference of this type of tumor for
metastasizing hematogenously rather than via the lymphatic system.
Similarly, regional lymphadenectomy confers no additional benefit.
Vorobyov et al (13) described
a vaginal approach for the removal of a leiomyoma that was located
in the rectovaginal wall in 1 out of 36 patients treated for rectal
tumors. The study also reported the following rates of surgery
performed by different methods: Electroexcision, 33.3%; transanal
excision, 27.8%; removal of the rectum via the pararectal approach,
16.7%; abdominal resection, 13.9%; extirpation of the rectum, 5.6%;
and trans-vaginal excision, 2.7%. In addition, the study noted that
complications in the early post-operative period were observed in
33.5% of patients. Visser et al (14) also reported that these procedures were
associated with a high complication rate, particularly with regards
to fistulae, which occurred in 21% of patients.
Transvaginal local excision for rectal carcinoma was
also performed by Fu et al (8)
in a series of 18 patients with T1 and T2 rectal cancer. For this
approach, the average distance from the dentate line best fit is ~4
cm. The potential complication of rectovaginal fistula was reported
in 1 out of the 18 patients, and was treated conservatively. The
use of the transvaginal approach was also reported by Hellan and
Maker (15) for the excision of an
anterior anorectal 5×5×8-cm GIST, and by Hara et al
(16) for the excision of an anterior
anorectal GIST that was ~5 cm in size. None of these studies
described any complications post-surgery or the requirement for a
diverting ileostomy. Furthermore, no recurrence was observed.
Preventing recurrence and enhancing the quality of
life of patients with small GISTs or leiomyoma are of importance
due to the low malignancy associated with these conditions, as
resection may not be necessary if such tumors are asymptomatic.
Therefore, in order to prevent the potential creation of a
rectovaginal fistula in the present patient during the restoration
of the injured part of the rectum, a diverting ileostomy was
created via laparoscopic surgery. The anal function of the patient
following surgery was examined throughout the post-operative
course, and was observed to be excellent, as indicated by the mFIQL
and Wexner scores (7,17). To the best of our knowledge, the
present study is the first case reporting the use of a transvaginal
resection for the excision of a lower rectal tumor. This
transvaginal approach for the excision of an anterior anorectal SMT
in the lower rectum provides a reasonable alternative to
traditional surgical procedures, which usually are affected by
post-operative complications.
In conclusion, the present study reports the case of
a patient with an SMT of the lower rectum that was successfully
resected transvaginally. This approach is less invasive than
conventional methods and offers a low risk of anal dysfunction.
Therefore, the transvaginal resection of rectal tumors should be
considered more often.
References
|
1
|
Hatch KF, Blanchard DK, Hatch GF III,
Wertheimer-Hatch L, Davis GB, Foster RS Jr and Skandalakis JE:
Tumors of the rectum and anal canal. World J Surg. 24:437–443.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Anderson PA, Dockerty MB and Buie LA:
Myomatous tumors of the rectum (leiomyomas and myosarcomas).
Surgery. 28:642–650. 1950.PubMed/NCBI
|
|
3
|
Serra J, Ruiz M, Lloveras B, Guillaumes S,
Garriga J and Trias R: Surgical outlook regarding leiomyoma of the
rectum. Report of three cases. Dis Colon Rectum. 32:884–887. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yasuda K, Nakajima M, Yoshida S, Kiyota K
and Kawai K: The diagnosis of submucosal tumors of the stomach by
endoscopic ultrasonography. Gastrointest Endosc. 35:10–15. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Miettinen M, Furlong M, Sarlomo-Rikala M,
Burke A, Sobin LH and Lasota J: Gastrointestinal stromal tumors,
intramural leiomyomas, and leiomyosarcomas in the rectum and anus:
A clinicopathologic, immunohistochemical, and molecular genetic
study of 144 cases. Am J Surg Pathol. 25:1121–1133. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fujimoto Y, Akiyoshi T, Kuroyanagi H,
Konishi T, Ueno M, Oya M and Yamaguchi T: Safety and feasibility of
laparoscopic intersphincteric resection for very lower rectal
cancer. J Gastrointest Surg. 14:645–650. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hashimoto H, Shiokawa H, Funahashi K,
Saito N, Sawada T, Shirouzu K, Yamada K, Sugihara K, Watanabe T,
Sugita A, et al: Development and validation of a modified fecal
incontinence quality of life scale for Japanese patients after
inter-sphincteric resection for very low rectal cancer. J
Gastroenterol. 45:928–935. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fu T, Liu B, Zhang S, Wang D and Zhang L:
Trans-vaginal local excision of rectal carcinoma. Curr Surg.
60:538–542. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Rullier E, Laurent C, Carles J, Saric J,
Michel P and Parneix M: Local recurrence of low rectal cancer after
abdominoperineal and anterior resection. Br J Surg. 84:525–528.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wibe A, Syse A, Andersen E, Tretli S,
Myrvold HE and Søreide O: Norwegian Rectal Cancer Group:
Oncological outcomes after total mesorectal excision for cure for
cancer of the lower rectum: Anterior vs. abdominoperineal
resection. Dis Colon Rectum. 47:48–58. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sasaki K, Gotoh Y, Nakayama Y, Hayasaka H,
Ishiyama Y and Miyashita H: Leiomyoma of the rectum. Int Surg.
70:149–152. 1985.PubMed/NCBI
|
|
12
|
Kusminsky RE and Bailey W: Leiomyomas of
the rectum and anal canal: Report of six cases and review of the
literature. Dis Colon Rectum. 20:580–599. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Vorobyov GI, Odaryuk TS, Kapuller LL,
Shelygin YA and Kornyak BS: Surgical treatment of benign, myomatous
rectal tumors. Dis Colon Rectum. 35:328–331. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Visser BC, Varma MG and Welton ML: Local
therapy for rectal cancer. Surg Oncol. 10:651–652. 2001. View Article : Google Scholar
|
|
15
|
Hellan M and Maker VK: Trans-vaginal
excision of a large rectal stromal tumor: An alternative. Am J
Surg. 191:121–123. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hara M, Takayama S, Arakawa A, Sato M,
Nagasaki T and Takeyama H: Trans-vaginal resection of a rectal
gastrointestinal stromal tumor. Surg Today. 42:909–912. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jorge JM, Wexner SD, Morgado PJ Jr, James
K, Nogueras JJ and Jagelman DG: Optimization of sphincter function
after the ileoanal reservoir procedure. A prospective, randomized
trial. D is Colon Rectum. 37:419–423. 1994. View Article : Google Scholar
|