Introduction
Gastric cancer is one of the most common
malignancies in Asia, and the second most common cause of
cancer-associated mortality in Japan, accounting for 49,830
mortalities and 13.9% of all Japanese cancer mortalities in 2011
(1). Gastric cancer typically
disseminates via hematogenous routes, lymphatic metastasis, local
invasion of adjacent tissues, or transcoelomic or peritoneal spread
(2). Common sites of metastasis
include the regional lymph nodes, liver, peritoneum, lungs and
bones (3). Metastases to the colon
are more rare, and typically originate from kidney, skin, breast,
prostate or ovarian carcinomas (4).
From gastric cancer, colonic metastasis is extremely rare; this
typically presents as linitis plastica or an annular stricture
resembling advanced primary colon cancer (5). There have been reports of cases of
colonic metastases assuming a polypoid or non-polypoid form that
mimics early colon cancer; however, all of these previous cases
were multiple metastases (5–7).
The present study reports a case of a patient with
early gastric cancer who developed a heterochronous, single,
non-polypoid colonic metastasis in the sigmoid colon and unilateral
Krukenberg tumor, composed of poorly differentiated adenocarcinoma
and signet ring cell carcinoma.
Case report
In September 2010, a 58-year-old female presented to
the University of Fukui Hospital (Fukui, Japan) with anemia and was
scheduled for an upper-GI endoscopy. A gastroscopy revealed a
typical type 0-IIc+IIa-like tumor on the lesser curvature of the
gastric body (8). Endoscopic biopsy
specimens revealed a well-differentiated tubular adenocarcinoma.
The patient underwent a distal gastrectomy with D2 lymphadenectomy
and Billroth I reconstruction in October 2010 (Fig. 1A). The histopathological examination
of the gastric tumor revealed a well-differentiated adenocarcinoma,
with submucosal invasion and no lymph node metastasis (Fig. 1B). However, poorly differentiated
adenocarcinoma and signet ring cell carcinoma were detected in the
deepest part of the lesion in the submucosal layer (Fig. 1B). The tumor was staged as T1bN0M0
according to the Japanese classification of gastric cancer
(8).
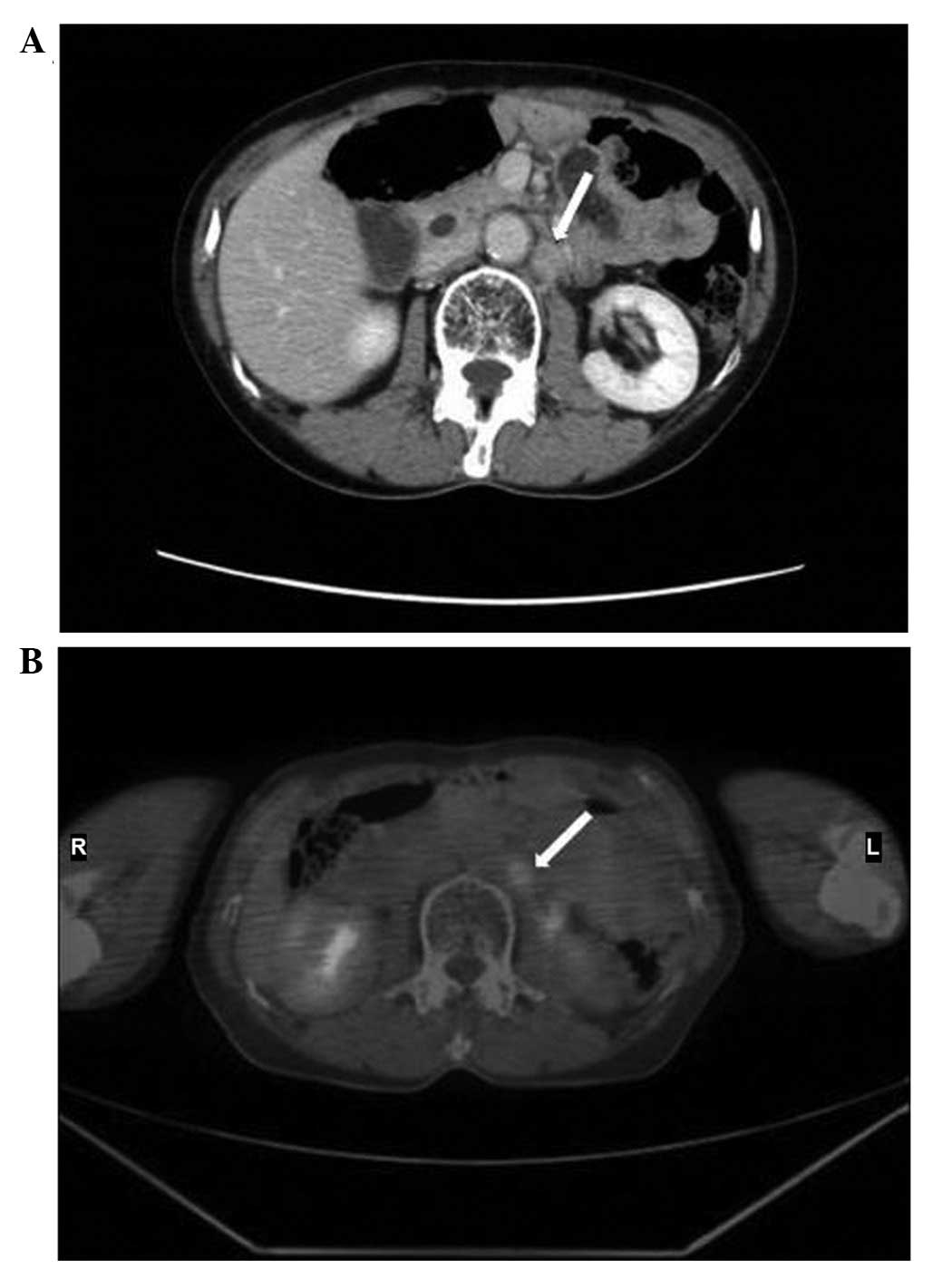
Following surgery, the patient was examined on
outpatient basis. In February 2013, the patient's serum
carcinoembryonic antigen (CEA) level had increased from the normal
range (<5.0 ng/ml) to 42.1 ng/ml. An abdominal computed
tomography (CT) scan and fludeoxyglucose-positron emission
tomography (FDG-PET)/CT revealed recurrent paraaortic lateral lymph
node metastasis (Fig. 2A and B). The
patient received 7 cycles of chemotherapy with S-1 (80
mg/m2/day; days 1–21) and cisplatin (60
mg/m2/day; day 8). Following chemotherapy, radiotherapy
was administered to the paraaortic lymph nodes of levels Th11-L3,
to a total dose 54 Gy (2 Gy/fraction).
Subsequent to chemotherapy and radiation therapy,
abdominal CT and FDG-PET scans were performed for evaluation of the
therapy. The abdominal CT scan revealed an enlarged left ovary, and
FDG-PET/CT indicated abnormal uptake unilaterally in the left ovary
and sigmoid colon (Fig. 3A and B). In
addition, a barium enema examination revealed an elevated lesion
with central depression in the sigmoid colon, located at the site
exhibiting abnormal accumulation on FDG-PET/CT (Fig. 3C). However, no abnormal uptake was
observed in the paraaortic lymph nodes. On the basis of these
findings, a diagnosis of unilateral Krukenberg tumor from gastric
cancer and early colon cancer was determined. The patient underwent
an oophorectomy and sigmoidectomy with D3 lymph node dissection
(Fig. 4A–C).
Intraoperative findings indicated no peritoneal
dissemination from gastric cancer, and intraoperative peritoneal
washing cytology of the rectouterine pouch was negative for
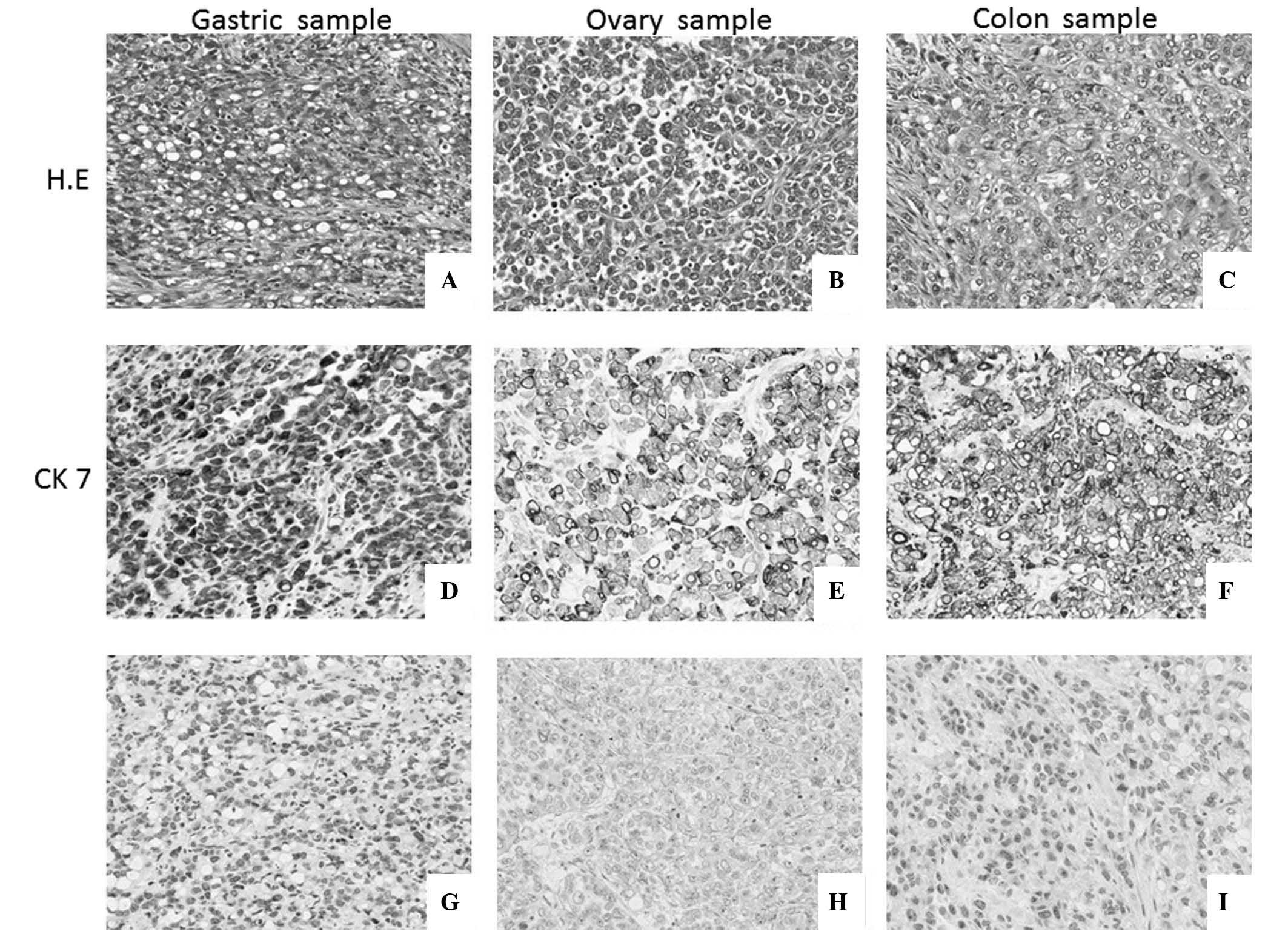
malignancy. On pathological examination, the left ovarian tumor was
revealed to be a poorly-differentiated adenocarcinoma and signet
ring cell carcinoma (Fig. 5A); the
right ovary was unremarkable (Fig.
5B). The sigmoid colon tumor was also revealed to be a
poorly-differentiated adenocarcinoma with scattered signet ring
cell carcinoma (Fig. 5C), which had
spread into the submucosal layer and partly permeated the serosal
layer. Metastasis was detected in the sigmoid mesocolon lymph
nodes, including the inferior mesenteric artery lymph nodes.
Immunohistological staining revealed that the primary gastric
cancer cells, ovarian tumor cells and sigmoid colon tumor cells
were positive for cytokeratin (CK) 7 and negative for CK20
(Fig. 5D–I). Thus, the diagnosis was
determined to be a unilateral Krukenberg tumor and sigmoid colonic
metastasis from gastric cancer.
Following the second surgery, the patient was
administered with further chemotherapy consisting of S-1 (80
mg/m2/day; days 1–14) and docetaxel (40
mg/m2/day; day 1). The patient's clinical course is
close observation; the patient has exhibited stable disease during
this chemotherapy regimen, and is still disease-free with ongoing
S-1 and docetaxel combined chemotherapy as of August 2015.
Discussion
Gastric cancer is one of the most fatal types of
cancer, particularly in East Asian countries, including Japan. In
clinical practice, the major routes of recurrence of gastric cancer
following radical resection include hematogenous spread, peritoneal
seeding, lymph node metastasis and local recurrence. Distant
metastasis most frequently arises via the hematogenous route.
Colonic metastases are uncommon, typically
originating from stomach, breast, skin (melanomas), renal,
prostatic or ovarian carcinomas (4).
In cases where colonic metastases arise from gastric
adenocarcinoma, the hematogenous route is the most common mode of
metastasis; metastatic deposits invade the submucosal lymphatic
system, extending to form a linitis plastica appearance or an
annular stricture (9). However, in
the present case, lymphatic spread was considered to be the route
of colonic metastasis from gastric cancer cells, which were
determined to consist of poorly differentiated adenocarcinoma and
signet ring cells in the deepest submucosal layer of the primary
gastric cancer. The following features indicated a lymphatic route
of metastasis: i) Metastatic paraaortic lateral lymph nodes were
detected prior to the second surgery; ii) pathologically metastatic
lymph nodes were detected in the sigmoid mesocolon, considered to
originate from paraaortic lymph node metastasis via lymphatic
vessels; iii) no intraoperative indications of peritoneal
metastasis were observed, and free cancer cells were not detected
by cytological examination of the peritoneal washings; and iv) a
Krukenberg tumor was diagnosed; although Krukenberg tumors may also
be induced by complex mechanisms, lymph node metastasis is
considered to be the most potent risk factor for their recurrence
(10–12).
Secondary gastric carcinomatous deposits (metastatic
tumors) in the colorectum invariably appear as single or multiple
strictures; this stricture appearance is similar to that of primary
colorectal cancer or inflammatory bowel disease. In rare cases,
flat or depressed lesions or polyps arising from colonic metastasis
of poorly differentiated gastric cancer and signet ring cell
carcinoma have been reported; however, all previously reported
cases presented as multiple synchronous lesions, which further
serves to accent the novelty of the current presentation of single
colonic depressed metastasis (4,13–15).
It is thought that the confirmed diagnosis of
metastatic colon cancer has the most useful pathological finding.
Immunohistochemical analyses may be performed to differentiate
between gastric and colonic primary tumors, with CK7 and CK20
commonly used as tumor markers (16).
CK7 expression has been observed in the majority of types of
carcinoma, in carcinoid tumors originating from lungs and
gastrointestinal tract (17), and in
Merkel cell tumors of the skin (18).
CK20+ staining is observed in the vast majority of cases
of colorectal carcinoma (17) and
Merkel cell tumors (19), in addition
to a high proportion of cases of gastric carcinoma,
cholangiocarcinoma, pancreatic carcinoma and transitional cell
carcinoma (16). In a previous study,
all colorectal cancer samples metastatic to the ovary were
CK7−/CK20+, while the majority of gastric
carcinomas metastatic to the ovary exhibied a
CK7+/CK20− staining pattern (20). In the present case, the following
features were observed: i) Sigmoid colon tumor cells with similar
appearance to the pathology of the previous gastric cancer; ii) no
tumor cells in the colonic mucosa, and proliferating tumor cells in
the colonic submucosal layer; and iii) positive CK7 expression and
negative CK20 expression on immunohistochemical analysis of the
primary gastric cancer cells, metastatic ovarian tumor cells and
sigmoid colon tumor cells. Due to the aforementioned findings, a
diagnosis of unilateral Krukenberg tumor and sigmoid colonic
metastasis from gastric cancer was confirmed.
In conclusion, the present study reports the case of
a patient with a unilateral Krukenberg tumor and sigmoid colonic
metastasis derived from early gastric cancer. Although this is an
extremely rare presentation, doctors must be aware of the possible
occurrence of colonic metastasis from gastric cancer, particularly
poorly-differentiated adenocarcinoma and signet ring cell
carcinoma. It is necessary to postoperatively examine patients
diagnosed with gastric cancer considering all possibilities,
including colonic metastasis.
References
|
1
|
Hamashima C, Ogoshi K, Okamoto M, Shabana
M, Kishimoto T and Fukao A: A community-based, case-control study
evaluating mortality reduction from gastric cancer b∂y endoscopic
screening in Japan. PLoS One. 8:e790882013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Baston OV: The function of the vertebral
veins and their role in the spread of metastases. Ann Surg.
112:138–149. 1940. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Rodriguez Salas N, González PC, Rivera T,
López AA, Martín Marino A and Lara Alvarez MA: Colonic anastomosis
and colonic polyp mucosal metastasis of signet ring cell gastric
adenocarcinoma. Clin Transl Oncol. 12:238–239. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ogiwara H, Konno H, Kitayama Y, Kino I and
Baba S: Metastases from gastric adenocarcinoma presenting as
multiple colonic polyps: Report of case. Surg Today. 24:473–475.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Katon RM, Brendler SJ and Ireland K:
Gastric linitis plastica with metastases to the colon: A mimic of
Crohn's disease. J Clin Gastroenterol. 11:555–560. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Metayer P, Antonietti M, Oumrani M, Hemet
J, Lemoine F and Basuyau J: Metastases of gastric adenocarcinoma
presenting as colonic polyposis. Report of a case. Dis Colon
Rectum. 34:622–623. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Iwabuchi M, Hiwatashi N, Suzuki T, Teshima
S, Saito T, Suzuki H, Mori Y, Ishibashi J, Chida N and Tadokoro K:
Multiple depressed-type colonic cancer (IIc)-like configurations:
metastases from gastric cancer. Dig Endosc. 14:73–77. 2002.
View Article : Google Scholar
|
|
8
|
Japanese Gastric Cancer Association:
Japanese classification of gastric carcinoma: 3rd English edition.
Gastric Cancer. 14:101–112. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Feczko PJ, Collins DD and Mezwa DG:
Metastatic disease involving the gastrointestinal tract. Radiol
Clin North Am. 31:1359–1373. 1993.PubMed/NCBI
|
|
10
|
D'Angelica M, Gonen M, Brennan MF,
Turnbull AD, Bains M and Karpeh MS: Patterns of initial recurrence
in completely resected gastric adenocarcinoma. Ann Surg.
240:808–816. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yoo CH, Noh SH, Shin DW, Choi SH and Min
JS: Recurrence following curative resection for gastric carcinoma.
Br J Surg. 87:236–242. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Berek JS and Natarajan S: Ovarian and
fallopian tube cacner. J Korean Gastric Cancer Assoc. 1:106–112.
2001.
|
|
13
|
Lee HC, Yang MT, Lin KY, Tu HY, Zhang TA
and Chen PH: Metastases from gastric carcinoma to colon in the form
of multiple flat-elevated lesions: A case report. Kaohsiung J Med
Sci. 20:552–557. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hiraga Y, Yasui W, Kumamomto T, Watanabe
M, Kobayakawa M, Eguchi N, Nakamura T, Kawamura H, Nakai S and
Kamei F: Colonic metastases of signet-ring cell carcinoma
presenting as multiple small depressed lesions like erosions:
Report of a case. Nippon Shokakibyo Gakkai Zasshi. 99:615–621.
2002.(In Japanese). PubMed/NCBI
|
|
15
|
Metayer P, Antonietti M, Oumrani M, Hemet
J, Lemoine F and Basuyau J: Metastases of a gastric adenocarcinoma
presenting as colonic polyposis. Report of a case. Dis Colon
Rectum. 34:622–623. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gao B, Xue X, Tai W, Zhang J, Chang H, Ma
X, Qi Y, Cui L, Yan F and Pan L: Polypoid colonic metastases from
gastric stump carcinoma: A case report. Oncol Lett. 8:1119–1122.
2014.PubMed/NCBI
|
|
17
|
Kummar S, Fogarasi M, Canova A, Mota A and
Ciesielski T: Cytokeratin 7 and 20 staining for the diagnosis of
lung and colorectal adenocarcinoma. Br J Cancer. 86:1884–1887.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jaeger T, Ring J and Andres C:
Histological, immunohistological, and clinical features of merkel
cell carcinoma in correlation to merkel cell polyomavirus status. J
Skin Cancer. 2012:9834212012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chu P, Wu E and Weiss LM: Cytokeratin 7
and cytokeratin 20 Expression in Epithelial Neoplasms: A Survey of
435 cases. Pathol. 13:962–972. 2000.
|
|
20
|
Park SY, Kim HS, Hong EK and Kim WH:
Expression of cytokeratins 7 and 20 in primary carcinomas of the
stomach and colorectum and their value in the differential
diagnosis of metastatic carcinomas to the ovary. Hum Pathol.
33:1078–1085. 2002. View Article : Google Scholar : PubMed/NCBI
|